
Abstract
Background
Sedentariness is an important risk factor for poor health. The main objective of this work was to examine the prospective association between television viewing time and indicators of physical function, mobility, agility, and frailty.
Methods
Data came from two independent cohorts of community-dwelling older adults: the Seniors-ENRICA (n = 2392, 3.5 year follow-up), and the ELSA (n = 3989, 3.9 year follow-up). At baseline, television viewing and other sedentary behaviors were ascertained using interviewer-administered questionnaires. In the Seniors-ENRICA cohort overall physical function at baseline and follow-up was assessed using the physical component summary (PCS) of the SF-12 Health Survey. Measures for incident mobility and agility limitations in both cohorts were based on standardized questions, and incident frailty was measured with the Fried criteria. Analyses were adjusted for the main confounders, including physical activity at baseline. Results across cohorts were pooled using a random effects model.
Results
Lower (worse) scores in the PCS were observed among those in the highest (vs. the lowest) tertile of television viewing time (b-coefficient:-1.66; 95% confidence interval:-2.81,-0.52; p-trend = 0.01). Moreover, the pooled odds ratios (95% CIs) for mobility limitations for the second and third (vs. the lowest) tertile of television viewing were 1.00 (0.84, 1.20) and 1.17 (1.00, 1.38); p-trend = 0.12, respectively. The corresponding results for agility limitations were 1.18 (0.97, 1.44) and 1.25 (1.03, 1.51); p-trend = 0.02. Results for incident frailty were 1.10 (0.80, 1.51) and 1.47 (1.09, 1.97); p-trend = 0.03. No association between other types of sedentary behavior (time seated at the computer, while commuting, lying in the sun, listening to music/reading, internet use) and risk of functional limitations was found.
Conclusions
Among older adults, longer television viewing time is prospectively associated with limitations in physical function independently of physical activity.
Similar content being viewed by others


Background
Aging comes with a decline in most physiological systems culminating in limited physical capacity. According to the 2004 Survey of Health, Ageing and Retirement in Europe, around 43% of European men and 60% of European women aged ≥50 years reported at least one limitation in mobility and functioning. Further, about 9% of men and 12% of women reported ≥1 limitations in activities of daily living [1]. This presents a major challenge to public health, as functional impairments are an important predictor of disability [2,3,4,5], institutionalization [4], hospitalization [3, 6] and death [7]. Hence, identifying modifiable determinants of functional ability decline is critical.
Older people spend most of their awake time in sedentary activities, defined by a low energy expenditure (≤1.5 METs) while sitting or reclined [8]. Sedentary time has been associated with an increased risk of cardiovascular disease, type 2 diabetes, cancer, all-cause and cause-specific mortality [9]. Among older adults, a growing body of evidence associates sedentary behaviors with functional limitations [10,11,12,13,14,15,16,17,18]. However, most of this evidence is limited by cross-sectional designs [10,11,12,13,14,15]. Additionally, the few existing prospective studies are either based on patients with osteoarthritis, [17, 18] focus on physical performance, [16, 17] or lack a standardized definition of frailty [18]. These prospective findings link sedentary time (measured by accelerometry [17, 18] or defined as self-reported television (TV) viewing time [16]) to declines in gait speed and chair stand rates [17], incident frailty [18] and lower usual walking speed in older adults [16].
Since time spent watching TV is the main component of sedentary time among older adults, [17, 19, 20] this study assesses the prospective association between the amount of TV viewing time and a range of validated measures of physical function (i.e. overall functioning, limitations in mobility or agility, and frailty). We analyze data from 2 independent cohorts of community-dwelling older adults: the Study on Nutrition and Cardiovascular Risk Factors in Spain (Seniors-ENRICA), and the English Longitudinal Study of Aging (ELSA) cohorts. Additionally, as far as we are aware, this study is the first to examine the prospective association between other types of sedentary activities (time seated at the computer, while commuting, lying in the sun, listening to music and reading) and the risk of functional limitations.
Methods
Study population and design
Seniors-ENRICA cohort
Baseline data collection was conducted between 2008 and 2010 as part of a larger cross-sectional study named ENRICA, in which participants were selected by stratified cluster sampling of the non-institutionalized adult population of Spain. Information was collected in three stages: a phone interview, -designed to collect data on socio-demographic factors, lifestyle and morbidity-, plus two home visits. During the first home visit, nurses collected blood and urine samples. Information on functional limitations was obtained during the second home visit [21]. Participants aged ≥60 years (N = 3289) were then invited to participate in a prospective study called Seniors-ENRICA [22]. Those who accepted (N = 2614) were followed through 2012, when a second wave of data was collected. Ninety-five participants (3.6%) died during follow-up. Of the remaining 2519 participants, we excluded 18 for lacking complete data on sedentary time variables and an additional 19 who had missing information on potential confounders. Further, for analyses involving the physical component summary (PCS) of the 12-item Short-Form Health Survey (SF-12), we excluded 90 individuals who lacked information on this variable, either at baseline or at follow-up. Our final sample consisted of 2392 participants (subsample 1). Similarly, for analyses based on mobility limitations, agility limitations or frailty, we excluded individuals with no complete information on these items (n = 184, n = 117 and n = 555, respectively), as well as those who had mobility limitations (n = 734), agility limitations (n = 848), of were already frail (n = 40) at baseline. Thus, analyses were performed on 1564 (subsample 2), 1517 (subsample 3) and 1887 (subsample 4) participants, respectively. All participants provided written informed consent, and the Clinical Research Ethics Committee of ‘La Paz’ University Hospital in Madrid approved the study.
ELSA cohort
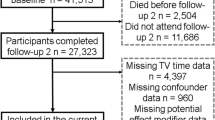
Established in 2002–2003, ELSA is a biennial longitudinal study representative of men and women aged ≥50 living in private households in England [23]. Participants are interviewed every 2 years and have a nurse visit every 4 years. Information on socio-demographic, psychological, cognitive and health factors is collected using computer-assisted interviews and self-completion questionnaires. ELSA is harmonized with ageing studies in other countries to facilitate international comparisons. For the current analyses we used information from 6118 participants aged ≥60 years who participated in wave 4 (2008–2009) and were followed through wave 6 (2012–2013). In both waves, information was collected using personal interviews, and measures of physical function and anthropometry were performed during nurse visits. From the initial sample, we excluded 169 individuals without complete data on sedentary time, 77 with implausible values on sedentary time (all of them above the 99 percentile of the distribution), and 53 with no information on potential confounders. For analyses examining mobility limitations, agility limitations, or frailty, we also excluded participants with no information on those items at baseline or at follow-up (n = 1074, n = 1074, and n = 1633, respectively), as well as those with mobility limitations (n = 1667), agility limitations (n = 1743), or frailty at baseline (197). Therefore, analyses were performed on 3078 (subsample 5), 3002 (subsample 6) and 3989 (subsample 7) participants, respectively. The National Research Ethics Service (MREC/01/2/91) provided the ethical approval for ELSA.
Study variables
A description of the main variables included in the manuscript by study cohort can be found in Table 1.
Sedentary behavior
In the Seniors-ENRICA study, information on sedentary behaviors was obtained using the Nurses’ Health Study questionnaire validated in Spain [24]. Specifically, participants were asked to recall the usual number of hours/day spent a) watching TV; b) sitting in front of a computer; c) reading; d) listening to music; e) commuting; f) sunbathing in summer; and g) sunbathing in winter. In the ELSA study, participants were asked to recall “How many hours of television do you watch on an ordinary day or evening, that is, Monday to Friday?” and “How many hours of television do you normally watch in total over the weekend, that is, Saturday and Sunday?” Average daily time spent watching TV was calculated as [(weekday TV time x 5) + (Weekend TV time)]/7. Additionally, participants were asked if they used a computer for internet or email.
In both cohorts TV viewing time was divided into sex-specific tertiles with the highest reflecting the highest level of sedentary behavior. The use of tertiles avoids the assumption that there is a linear relationship between sedentary time and the studied outcomes. More specifically, we have used sex-specific tertiles because of the different distribution of the studied sedentary behaviors across sexes, and to avoid creating exceedingly small subgroups.
Functional limitations
Overall physical functioning
The PCS questionnaire was used in the Seniors-ENRICA cohort to assess overall function. The 4 items of the PCS evaluate four health dimensions: physical functioning, role-physical, bodily pain and general health. Subjects’ answers to any given item receive a numerical score which, after coding, is ranked on a scale of 0–100. The PCS score is then standardized to a national norm with a mean of 50 and a standard deviation (SD) of 10 to allow comparing the PCS for each study participant against the mean score in the Spanish population. A higher score indicates better physical function [25]. The SF-12 questionnaire was not available in the ELSA cohort.
Mobility limitation
In the Seniors-ENRICA study we considered someone reporting mobility limitation when they provided an affirmative answer to any of the following questions: 1)“Do you experience any difficulty in picking up/carrying a shopping bag?”, 2)“Do you experience any difficulty in climbing one flight of stairs?”, or 3)“Do you experience any difficulty in walking several city blocks (a few hundred meters)?” [5] In the ELSA study the questions we used to define mobility limitation were slightly different. An individual was considered to report mobility limitation if they answered affirmatively to at least one of the following: 1)“Do you experience difficulty lifting/carrying weights over 10 pounds?” 2)“Do you experience difficulty climbing one flight of stairs without resting?”, or 3)“Do you experience any difficulty walking 1/4 mile unaided?”
Agility limitation
This variable was assessed using the question “Do you experience any difficulty in bending/kneeling” in the Seniors-Enrica [26], and the question “Do you experience any difficulty stooping/kneeling/crouching?” in the ELSA study.
Frailty
According to the criteria proposed by Fried et al [27], individuals meeting ≥3 of the following criteria were considered frail: 1) Weakness: defined in both studies as the cohort-specific lowest quintile of grip strength adjusted for sex and body mass index (BMI); strength was measured with a hand held dynamometer, and the highest value in two (seniors-ENRICA) or three (ELSA) consecutive measures was used in the analyses; 2) Exhaustion: defined in both cohorts as an affirmative response to any of two statements taken from the Center for Epidemiologic Studies Depression Scale: “I felt that everything I did was a big effort in the last week” or “I could not get going in the last week” [28]; 3) Weight loss: defined in the Seniors-ENRICA study as an unintentional loss of ≥4.5 kg of body weight in the preceding year, and in the ELSA cohort as either loss of ≥10% of body weight since wave 2 or current BMI < 18.5 kg/m2; 4) Low physical activity: defined in the Seniors-ENRICA cohort as walking ≤2.5 h/week in men and ≤2 h/week in women. In the ELSA-study an overall measure of physical activity (PA) was derived by multiplying the frequency of vigorous, moderate and mild exercise by the metabolic equivalent (MET) value for each activity (6, 3 and 1.5, respectively). Low PA was defined as the lowest sex-specific quintile of the distribution of this overall measurement. Finally, the fifth criterion was slow walking speed, assessed in both cohorts by measuring the time taken to walk a distance of 8 feet at usual pace. The test was repeated and the mean of the two measurements calculated. Walking speeds in the lowest quintile of the distribution according to sex and height were defined as low gait speed.
Other variables
For both cohorts, baseline data included information on age, sex, educational status, and self-reported tobacco consumption. Participants also reported whether they had previously suffered from any of the following diseases: cardiovascular disease (ischemic heart disease, stroke, or heart failure), diabetes, chronic lung disease (asthma or chronic bronchitis), or osteomuscular disease (osteoarthritis or arthritis).
Baseline weight and height were measured using standard methods. We calculated BMI as (weight in kg)/(height in m)2. Normal weight was defined as a BMI <25, overweight as a BMI between 25-29.9, and obesity as a BMI ≥30.
In the Seniors-ENRICA cohort, food consumption was assessed with a computerized validated diet history developed from that used in the EPIC-cohort study in Spain [29], and adherence to the Mediterranean diet was summarized using the Mediterranean Diet Adherence Score (MEDAS) index. [30] We used Spanish food composition tables to calculate energy intake [29]. Unfortunately the ELSA-study did not include a diet history.
For Seniors-ENRICA participants, PA information was gathered using the EPIC-cohort questionnaire [31] and summarized according to the Cambridge Physical Activity Index. [32] The Cambridge index includes four categories of the sum duration of walking, cycling, and sports (hours/week); this sum is then cross-tabulated with occupational PA categories to assign participants into one of four groups (inactive, moderately inactive, moderately active, and active). Alternatively, the average number of hours/week spent in vigorous PA was used. How we defined the overall measure of PA for ELSA study is described above (see Frailty section).
Statistical analysis
The association between baseline TV viewing time (modeled as tertiles) and PCS at follow-up was assessed using linear regression. In addition, we used logistic regression to evaluate how TV viewing time was associated with incident agility or mobility limitations and with frailty. Two regression models were built in each case. Model 1 adjusted for age, sex, and education; model 2 further adjusted for BMI, tobacco consumption, PA (using either the Cambridge index or the average number of hours/week spent in vigorous PA in the seniors-ENRICA cohort; and an overall measurement of PA in the ELSA study), cardiovascular disease, diabetes, chronic lung disease, and osteomuscular disease. In the Seniors-ENRICA study, model 2 also controlled for total energy intake and the MEDAS index. Linear regression models with follow-up PCS scores as dependent variable further adjusted for baseline PCS scores. Finally, the association between TV viewing time and onset of each individual frailty criterion was evaluated using logistic regression models controlling for the same covariates as in model 2 above. All aforementioned potential confounders were time-constant variables measured at baseline
We performed a random effects meta-analysis to combine the effect sizes obtained in both cohorts. Between-cohort heterogeneity was tested with the Chi-square-based Q statistic and quantified with the use of the I2 statistic [33]. Linear trends were evaluated using the generalized least squares for trend estimations of summarized dose-response data.
Using likelihood ratio tests, we tested for the potential interaction between TV watching tertiles and indicator variables for the following subgroups: sex (men/women), BMI (<25/25-29.9/≥30), leisure time PA (inactive/active), and diabetes (no/yes). These analyses were adjusted for the same covariates as model 2 above.
Results
Tables 2 and 3 show the distribution of TV viewing time according to baseline characteristics of study participants in the Seniors-ENRICA and ELSA cohorts, respectively. Results are shown for the different sub-samples evaluated. Overall, women, participants with lower educational level, higher BMI and lower MEDAS index, as well as smokers and those who were inactive or suffered from diabetes or osteomuscular disease, spent more time watching TV than their counterparts. Mean TV time at baseline was also higher among individuals who developed mobility limitations, agility limitations or frailty (data not shown).
In the Seniors-ENRICA cohort, mean (SD) baseline and follow-up PCS scores were 45.5 (11.7) and 44.5 (12.4), respectively. Also, 30.0% of participants developed mobility limitations, 44.8% developed agility limitations, and 7.3% developed frailty over a mean (SD) follow-up period of 3.3 (0.6) years. Corresponding figures for the ELSA cohort were 47.1%, 48.4%, and 5.1% over a mean (SD) follow-up of 3.9 (0.2) years.
In Table 4, we present results regarding TV time and limitations in physical function. As results from basically-adjusted models (sociodemographic variables only), and fully- adjusted models were similar, we emphasize fully-adjusted results throughout. Compared to individuals in the lowest tertile of TV time, those in the highest tertile showed lower PCS scores (b-coefficient:-1.66; 95%CI:-2.81,-0.52); p-trend = 0.01). Further adjustment for the mental component summary of the SF-12 (b-coefficient: -1.81; (95%CI:-2.94,-0.67); p-trend < 0.01), yielded comparable results.
The pooled odds ratios [ORs] (95%CI) for mobility limitations comparing the second and third to the lowest tertile of TV viewing were1.00 (0.84, 1.20) and 1.17 (1.00, 1.38), respectively. Corresponding ORs for agility limitations were 1.18 (0.97, 1.44) and 1.25 (1.03, 1.51); and 1.10 (0.80, 1.51) and 1.47 (1.09, 1.97) for incident frailty. Effect modification by sex, BMI, diabetes, or PA level was not observed in any of the cohorts (see Additional files 1 and 2: Tables S1 and S2).
Results for the association between TV time and each individual frailty criterion are shown in Table 5. The OR (95%CI) from pooled analyses showed a non-statistically significant increased risk of exhaustion (1.16 (0.98, 1.38)) and low PA (1.17 (0.90, 1.52)) among individuals in the third tertile of TV time. Further, we observed an increased risk of weakness (p = 0.02) as time spent watching TV lengthened.
As ancillary analyses, we examined associations between five types of sedentary activities (other than watching TV) such as time seated at the computer, while commuting, lying in the sun, listening to music, and reading, and the risk of functional limitations (Seniors-ENRICA study); and the association between internet usage (no/yes) and the risk of functional limitations (ELSA cohort). Fully-adjusted analyses yielded no associations between most of these activities and physical function (Table 6). However, computer use seemed to have certain beneficial effect in both cohorts. Time seated at the computer showed a trend toward more favorable SF-12 scores (p = 0.05), and internet usage was associated with a decreased risk of agility limitations (OR: 0.76; 95% CI:0.62,0.93) and frailty (OR:0.64; 95% CI:0.43,0.95).
Discussion
Our results show an association between time spent watching TV and an increased risk for unfavorable outcomes in physical functioning. These associations persisted after accounting for a range of covariates, including physical activity.
Cross-sectional studies have recently linked time spent watching TV with lower (worse) PCS scores (SF-36) [12], lower mean grip strength, [11, 14] lower timed Up-&-Go scores [11], and higher prevalence of IADL [10] and ADL [13] limitations in older adults. Further, evidence from newly-published longitudinal research deems sedentary time as a likely risk factor for functional decline [16,17,18]. Of these studies, two are based on the Osteoarthritis Initiative database, and connect accelerometer-based total sedentary time with declines in gait speed and chair stand rates [17], as well as with incident frailty, defined as low gait speed (<0.6 m/second) or inability to perform a single chair stand [18]. The third study, using data from 8,623 community-based participants enrolled in the EPIC-Norfolk, ascertained that watching TV for longer times is associated with lower usual walking speed, but not with lower grip strength [16].
Our results support the existence of a direct association between sedentary time and physical weakness, while contributing evidence indicating that time spent watching TV may be an important risk factor of agility limitations and frailty. Our results also suggest that health policy interventions should target heavy television viewers. In this subpopulation, just relatively small reductions in time in front of the TV set (i.e., moving from the third to the second tertile of TV viewing) could substantially reduce the risk of suffering physical limitations. Whereas the adverse consequences of excessive time spent watching TV could be palliated by increasing moderate or vigorous physical activity [34],the fact that our associations were independent of physical activity level suggests that harmful effects may also be reduced with no substantial modification of total activity For instance, by replacing time spent seated or reclined watching TV with time in a standing position browsing the computer screen. Future research should assess the feasibility and effectiveness of such interventions.
In contrast to our TV time-related findings, we failed to discern additional associations between other sedentary activities and functional limitations. Findings from previous cross-sectional research in older adults discriminated between associations of passive sedentary time (TV time, listening or talking while sitting, and sitting around) and mentally-active sedentary time (consisting of computer-use and reading books or newspapers) with health-related attributes, such as obesity and moderate-vigorous activity [20]. Similarly, cross-sectional findings from the ELSA cohort (wave 4) indicate that whereas internet usage was associated with stronger grip strength, time spent watching TV was linked to weaker strength, supporting our TV time-related results. The reasons behind these contrasting associations are not known. A potential explanation is that watching TV entails specific health risks beyond those expected from being seated [35]. Also, one could speculate that the amount of time spent watching TV is more easily recalled than other sedentary activities, that the time spent in these behaviors is relatively small (making it difficult to assess their full impact on health), or that these behaviors differ from TV watching in their association with potential confounders; thus adjusting for the same set the covariates may lead to different residual confounding.
TV watching could influence the risk of functional limitations through several mechanisms. First, longer periods of time spent sitting have been associated with a greater risk of sarcopenia [36], a major cause of functional limitations in the elderly [37, 38]. Actually, time spent sitting or lying down is the only state characterized by absence of muscle contraction, which may affect muscle metabolism independently of total PA. In fact, experimentally reducing normal spontaneous standing and ambulatory time had a much greater effect on the regulation of skeletal muscle lipoprotein lipase (important for controlling plasma triglyceride catabolism, HDL cholesterol, and other metabolic risk factors) than adding vigorous exercise training on top of normal non-exercise activity [39]. Second, sedentary behavior has been related to a higher risk of several pathologic conditions (e.g., cardiovascular disease), themselves important risk factors for functional limitations [40]. Finally, there is some evidence that sedentariness increases inflammation [41] which, in turn, may play a role in the development of functional limitations [42].
Cross-sectional studies focusing on characteristics of sedentary behavior other than its duration showed that daily breaks in sedentary time are associated with better leg function [43], improved lower limb extensor muscle quality [44], higher scores in the Senior Fitness Test [45], and lower risk for ADL impairments [45]. In this context, several intervention studies evaluating the feasibility of increasing the number of breaks in prolonged sedentary time are being conducted, with encouraging results [46, 47]. Recently, a published meta-analysis of randomized controlled trials also showed the effectiveness of step-counter use in walking programs to reduce sedentary time among older adults [48]. Future research should assess whether appropriate interventions addressing sedentariness can reduce the risk of functional limitations.
Our analysis has several strengths. First, the Seniors-ENRICA and ELSA cohorts had a prospective design, which allows for the appropriate time sequence between sedentary time and functional limitations. Second, in both cohorts physical function was ascertained with validated measures, including a standardized definition of frailty according to the Fried criteria, and physical performance tests were conducted by trained staff under standardized conditions. Finally, we considered a wide variety of function impairments, from less severe problems such as mobility or agility limitations, to more severe, such as frailty.
The main limitation of the study was its reliance on self-reported information. And, we could not evaluate the presence of breaks in sedentary time, which, as mentioned above, may be an important factor in the associations examined. Also, we could not evaluate the association between sedentary time and PCS score in the ELSA cohort since the SF-12 questionnaire was not available. Finally, although we adjusted our results for a large number of potential confounders, certain residual confounding cannot be ruled out because TV watching is strongly associated with the presence of unhealthy behaviors (i.e. unhealthy diet) [49], and with lower socioeconomic status [50], factors that have been associated with impaired physical function.
Conclusions
Our study suggests that time spent watching TV is associated with an increased risk of several functional limitations in older adults. Thus, our study adds to current knowledge on sedentary behavior and its harmful effects by focusing on outcomes other than diseases, and suggests that replacing TV time by time spent standing or in light or more intense physical activity, according to the abilities of each individual, could delay physical impairment in the old age. Notwithstanding this, prospective studies including objective measures of sedentary behavior and characterization of breaks in sedentary time should further evaluate the relationship between sedentary behavior and physical limitations.
References
Mackenbach JP, Avendano M, Andersen_Ranberg K, Aro AR. Physical health. In: Börsch-Supan A, Brugiavini A, Jürges H, Mackenbach J, Siegrist J, Weber G, editors. Health, Ageing and Retirement in Europe: First Results From the Survey of Health, Ageing and Retirement in Europe. Mannheim: Mannheim Research Institute for the Economics of Aging (MEA); 2005. p. 82–8.
Seidel D, Brayne C, Jagger C. Limitations in physical functioning among older people as a predictor of subsequent disability in instrumental activities of daily living. Age Ageing. 2011;40:463–9.
Legrand D, Vaes B, Mathei C, Adriaensen W, Van PG, Degryse JM. Muscle strength and physical performance as predictors of mortality, hospitalization, and disability in the oldest old. J Am Geriatr Soc. 2014;62:1030–8.
Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85–94.
Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332:556–61.
Cawthon PM, Fox KM, Gandra SR, et al. Do muscle mass, muscle density, strength, and physical function similarly influence risk of hospitalization in older adults? J Am Geriatr Soc. 2009;57:1411–9.
Cooper R, Kuh D, Hardy R. Objectively measured physical capability levels and mortality: systematic review and meta-analysis. BMJ. 2010;341:c4467.
Owen N. Sedentary behavior: understanding and influencing adults’ prolonged sitting time. Prev Med. 2012;55:535–9.
Biswas A, Oh PI, Faulkner GE, et al. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med. 2015;162:123–32.
Chen T, Narazaki K, Haeuchi Y, Chen S, Honda T, Kumagai S. Associations of Sedentary Time and Breaks in Sedentary Time With Disability in Instrumental Activities of Daily Living in Community-Dwelling Older Adults. J Phys Act Health. 2016;13(3):303–9. doi:10.1123/jpah.2015-0090.
Cooper AJ, Simmons RK, Kuh D, Brage S, Cooper R. Physical activity, sedentary time and physical capability in early old age: British birth cohort study. PLoS One. 2015;10:e0126465.
Dempsey PC, Howard BJ, Lynch BM, Owen N, Dunstan DW. Associations of television viewing time with adults’ well-being and vitality. Prev Med. 2014;69:69–74.
Dunlop DD, Song J, Arnston EK, et al. Sedentary time in US older adults associated with disability in activities of daily living independent of physical activity. J Phys Act Health. 2015;12:93–101.
Hamer M, Stamatakis E. Screen-based sedentary behavior, physical activity, and muscle strength in the English longitudinal study of ageing. PLoS One. 2013;8:e66222.
Manns P, Ezeugwu V, Armijo-Olivo S, Vallance J, Healy GN. Accelerometer-Derived Pattern of Sedentary and Physical Activity Time in Persons with Mobility Disability: National Health and Nutrition Examination Survey 2003 to 2006. J Am Geriatr Soc. 2015;63:1314–23.
Keevil VL, Wijndaele K, Luben R, Sayer AA, Wareham NJ, Khaw KT. Television viewing, walking speed, and grip strength in a prospective cohort study. Med Sci Sports Exerc. 2015;47:735–42.
Semanik PA, Lee J, Song J, et al. Accelerometer-monitored sedentary behavior and observed physical function loss. Am J Public Health. 2015;105:560–6.
Song J, Lindquist LA, Chang RW, et al. Sedentary Behavior as a Risk Factor for Physical Frailty Independent of Moderate Activity: Results From the Osteoarthritis Initiative. Am J Public Health. 2015;105:1439–45.
Healy GN, Clark BK, Winkler EA, Gardiner PA, Brown WJ, Matthews CE. Measurement of adults’ sedentary time in population-based studies. Am J Prev Med. 2011;41:216–27.
Kikuchi H, Inoue S, Sugiyama T, et al. Distinct associations of different sedentary behaviors with health-related attributes among older adults. Prev Med. 2014;67:335–9.
Rodriguez-Artalejo F, Graciani A, Guallar-Castillon P, et al. Rationale and methods of the study on nutrition and cardiovascular risk in Spain (ENRICA). Rev Esp Cardiol. 2011;64:876–82.
Graciani A, Garcia-Esquinas E, Lopez-Garcia E, Banegas JR, Rodriguez-Artalejo F. Ideal Cardiovascular Health and Risk of Frailty in Older Adults. Circ Cardiovasc Qual Outcomes. 2016;9:239–45.
Steptoe A, Breeze E, Banks J, Nazroo J. Cohort profile: the English longitudinal study of ageing. Int J Epidemiol. 2013;42:1640–8.
Martinez-Gonzalez MA, Lopez-Fontana C, Varo JJ, Sanchez-Villegas A, Martinez JA. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005;8:920–7.
Vilagut G, Valderas JM, Ferrer M, Garin O, Lopez-Garcia E, Alonso J. Interpretation of SF-36 and SF-12 questionnaires in Spain: physical and mental components. Med Clin (Barc). 2008;130:726–35.
Rosow I, Breslau N. A Guttman health scale for the aged. J Gerontol. 1966;21:556–9.
Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–56.
Radloff LS. The CES-D Scale: A Self-Report Depression Scale for Resarch in the General Population. Applied Psychological Measurement. 1977;1:385–401.
Guallar-Castillon P, Sagardui-Villamor J, Balboa-Castillo T, et al. Validity and reproducibility of a Spanish dietary history. PLoS One. 2014;9:e86074.
Schroder H, Fito M, Estruch R, et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J Nutr. 2011;141:1140–5.
Pols MA, Peeters PH, Ocke MC, Slimani N, Bueno-de-Mesquita HB, Collette HJ. Estimation of reproducibility and relative validity of the questions included in the EPIC Physical Activity Questionnaire. Int J Epidemiol. 1997;26 Suppl 1:S181–9.
Wareham NJ, Jakes RW, Rennie KL, et al. Validity and repeatability of a simple index derived from the short physical activity questionnaire used in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Public Health Nutr. 2003;6:407–13.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Ekelund U, Steene-Johannessen J, Brown WJ, et al. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet. 2016;388:1302–10.
Stamatakis E, Davis M, Stathi A, Hamer M. Associations between multiple indicators of objectively-measured and self-reported sedentary behaviour and cardiometabolic risk in older adults. Prev Med. 2012;54:82–7.
Gianoudis J, Bailey CA, Daly RM. Associations between sedentary behaviour and body composition, muscle function and sarcopenia in community-dwelling older adults. Osteoporos Int. 2015;26:571–9.
Roubenoff R. Sarcopenia: a major modifiable cause of frailty in the elderly. J Nutr Health Aging. 2000;4:140–2.
Woo J, Leung J, Sham A, Kwok T. Defining sarcopenia in terms of risk of physical limitations: a 5-year follow-up study of 3,153 chinese men and women. J Am Geriatr Soc. 2009;57:2224–31.
Hamilton MT, Hamilton DG, Zderic TW. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes. 2007;56:2655–67.
Guralnik JM, LaCroix AZ, Abbott RD, et al. Maintaining mobility in late life. I. Demographic characteristics and chronic conditions. Am J Epidemiol. 1993;137:845–57.
Hamer M, Smith L, Stamatakis E. Prospective association of TV viewing with acute phase reactants and coagulation markers: English Longitudinal Study of Ageing. Atherosclerosis. 2015;239:322–7.
Friedman EM, Christ SL, Mroczek DK. Inflammation Partially Mediates the Association of Multimorbidity and Functional Limitations in a National Sample of Middle-Aged and Older Adults: The MIDUS Study. J Aging Health. 2015;27:843–63.
Davis MG, Fox KR, Hillsdon M, Sharp DJ, Coulson JC, Thompson JL. Objectively measured physical activity in a diverse sample of older urban UK adults. Med Sci Sports Exerc. 2011;43:647–54.
Chastin SF, Ferriolli E, Stephens NA, Fearon KC, Greig C. Relationship between sedentary behaviour, physical activity, muscle quality and body composition in healthy older adults. Age Ageing. 2012;41:111–4.
Sardinha LB, Santos DA, Silva AM, Baptista F, Owen N. Breaking-up sedentary time is associated with physical function in older adults. J Gerontol A Biol Sci Med Sci. 2015;70:119–24.
Fitzsimons CF, Kirk A, Baker G, Michie F, Kane C, Mutrie N. Using an individualised consultation and activPAL feedback to reduce sedentary time in older Scottish adults: results of a feasibility and pilot study. Prev Med. 2013;57:718–20.
Gardiner PA, Eakin EG, Healy GN, Owen N. Feasibility of reducing older adults’ sedentary time. Am J Prev Med. 2011;41:174–7.
Qiu S, Cai X, Ju C, et al. Step Counter Use and Sedentary Time in Adults: A Meta-Analysis. Medicine (Baltimore). 2015;94:e1412.
Harris JL, Bargh JA, Brownell KD. Priming effects of television food advertising on eating behavior. Health Psychol. 2009;28:404–13.
Stamatakis E, Hillsdon M, Mishra G, Hamer M, Marmot M. Television viewing and other screen-based entertainment in relation to multiple socioeconomic status indicators and area deprivation: the Scottish Health Survey 2003. J Epidemiol Community Health. 2009;63:734–40.
Acknowledgments
Not applicable.
Funding
This work was supported by FIS grant no. 12/1166 and 13/0288 (Instituto de Salud Carlos III, State Secretary of R + D + I and FEDER/FSE), MINECO R + D + I grant DEP2013-47786-R, the FRAILOMIC Initiative (European Union FP7-HEALTH-2012-Proposal no. 305483-2), the Ageing Trajectories of Health: Longitudinal Opportunities and Synergies (ATHLOS) project, the CIBER of Epidemiology and Public health (CIBERESP) and the CIBER of Mental Health (CIBERSAM). The ATHLOS project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 635316. ELSA waves have been funded jointly by UK government departments and the National Institute on Aging, in the USA. The funding agencies had no role in study design, data analysis, interpretation of results, manuscript preparation or in the decision to submit this manuscript for publication.
Availability of data and materials
Researchers can apply to the ELSA Linked Data Access Committee for permission to use this data. Other datasets analysed during the current study available from the corresponding author on reasonable request.
Authors’ contributions
EGE and FRA conceived the study. EGE performed the statistical analyses and drafted the manuscript. FRA and ELG conducted the research. All authors reviewed the manuscript for important intellectual content. EGE and FRA had primary responsibility for final content. All authors have read the manuscript, accept responsibility for the manuscript’s content and agree the work is ready for submission to this Journal.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
All participants provided written informed consent, and the Clinical Research Ethics Committee of ‘La Paz’ University Hospital in Madrid approved the study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional files
Additional file 1: Table S1.
Stratified results for the association between tertiles of TV viewing time and incident limitations in physical function in older adults from the Seniors-ENRICA cohort. (DOCX 17 kb)
Additional file 2: Table S2.
Stratified results for the association between tertiles of TV viewing time and incident limitations in physical function in older adults from the ELSA cohort. (DOCX 17 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
García-Esquinas, E., Andrade, E., Martínez-Gómez, D. et al. Television viewing time as a risk factor for frailty and functional limitations in older adults: results from 2 European prospective cohorts. Int J Behav Nutr Phys Act 14, 54 (2017). https://doi.org/10.1186/s12966-017-0511-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-017-0511-1