
Abstract
Background
Hepatitis B virus (HBV) infection is an important cause of morbidity and mortality with a very high burden in Africa. The risk of developing chronic infection is marked if the infection is acquired perinatally, which is largely preventable through a birth dose of HBV vaccine. We examined the cost-effectiveness of a birth dose of HBV vaccine in a medical setting in Ethiopia.
Methods
We constructed a decision analytic model with a Markov process to estimate the costs and effects of a birth dose of HBV vaccine (the intervention), compared with current practices in Ethiopia. Current practice is pentavalent vaccination (DPT-HiB-HepB) administered at 6, 10 and 14 weeks after birth. We used disability-adjusted life years (DALYs) averted to quantify the health benefits while the costs of the intervention were expressed in 2018 USD. Analyses were based on Ethiopian epidemiological, demographic and cost data when available; otherwise we used a thorough literature review, in particular for assigning transition probabilities.
Results
In Ethiopia, where the prevalence of HBV among pregnant women is 5%, adding a birth dose of HBV vaccine would present an incremental cost-effectiveness ratio (ICER) of USD 110 per DALY averted. The estimated ICER compares very favorably with a willingness-to-pay level of 0.31 times gross domestic product per capita (about USD 240 in 2018) in Ethiopia. Our ICER estimates were robust over a wide range of epidemiologic, vaccine effectiveness, vaccine coverage and cost parameter inputs.
Conclusions
Based on our cost-effectiveness findings, introducing a birth dose of HBV vaccine in Ethiopia would likely be highly cost-effective. Such evidence could help guide policymakers in considering including HBV vaccine into Ethiopia’s essential health services package.
Similar content being viewed by others

Background
Hepatitis B virus (HBV) infection remains an important cause of morbidity and mortality globally. According to 2015 estimates by the World Health Organization (WHO), about 260 million individuals (3.5% of the world’s population) were living with chronic HBV infection in the world [1]. Most HBV infections (68%) occurred in the African and Western Pacific regions where the HBV prevalence was the highest (6.1% in the African region and 6.2% in Western Pacific among the general population, respectively) [1]. In 2015, viral hepatitis led to 1.34 million deaths globally, of which 66% were resulting from complications of chronic HBV infection such as cirrhosis (53%) and hepatocellular carcinoma (34%) [1].
The prevalence of HBV infection is estimated at 7.4% among the general population of Ethiopia, which is at the highest end of intermediate endemicityFootnote 1 [2]. Likewise, according to a meta-analysis of prevalence studies in Ethiopia, the prevalence of HBV infection among pregnant women was estimated at 4.7% that is lower than estimates from other African countries such as Nigeria, Cameroon and Ghana where the prevalence of HBV infection among pregnant women ranged from 9.8 to 14.1% [3]. Pregnant women infected with HBV can potentially transmit the virus to their infants usually during birth. The risk of transmission to the newborn is largely dependent on the presence or absence of the hepatitis B virus envelope antigen (HBeAg) in HBV-infected pregnant women. In Africa, infants born to mothers who are positive for both hepatitis B surface antigen (HBsAg) and HBeAg carry a 28% risk of transmission with a lower risk (8%) in mothers who have lost HBeAg [4]. A study on the risk of mother to child transmission (MTCT) of HBV in Ethiopia has shown a higher transmission rate [5]. Perinatally infected infants are at the highest risk of chronic HBV infection that occurs in 80–90% of infected infants [6].
Measures to control viral hepatitis have progressively increased globally [1]. Most countries including Ethiopia have introduced hepatitis B vaccine into their routine infant immunization programs. The birth dose of hepatitis B (HepB-BD) vaccine is the main modality in the prevention of mother to child HBV transmission. Ideally, the birth dose should be given within 24 h of birth but can still be partially effective even if given beyond, its effectiveness diminishing with the passage of time [7]. Unfortunately, as of 2015, only 10% of African countries had introduced HepB-BD vaccine, and it is not yet introduced in Ethiopia [1]. Furthermore, other preventive measures such as hepatitis B immunoglobulin or medications for the treatment of HBV infection are not yet part of Ethiopia’s essential health service package [8]. In the absence of universal HepB-BD vaccine or other effective interventions, perinatally acquired HB infection remains a major cause of chronic liver disease when infected children reach adulthood [9].
The fight against viral hepatitis is gathering momentum globally. Combating hepatitis is included in the Sustainable Development Goals (SDG 3.3) [10]. The World Health Assembly in 2016 adopted a Global Health Sector Strategy on viral hepatitis with elimination as its overarching goal [1]. In line with the global response, Ethiopia’s Federal Ministry of Health (FMoH) has developed guidelines aiming at scaling up viral hepatitis preventive measures, and standardized screening and management of patients with viral hepatitis toward improved outcome [11].
Evidence on the cost-effectiveness of HepB-BD vaccine is scarce in sub-Saharan Africa. A cost-effectiveness analysis (CEA) of adding HepB-BD vaccine in Mozambique has shown that it could be highly cost-effective within the Mozambique health system [12]. Yet, CEA results may vary with the setting, the epidemiology of HBV and intervention costs. Therefore, in this paper, we evaluate the incremental cost-effectiveness of adding HepB-BD vaccine to the three-dose regimen given to infants at 6, 10 and 14 weeks after birth. The evidence we generate serve as a useful input for Ethiopian policymakers in considering including HepB-BD vaccine into the national essential health services package.
Methods
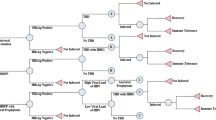
We constructed a decision analytic model with a Markov process (Additional file 1 and Fig. 1) to estimate intervention costs and health impact of an infected individual over a lifetime. We used TreeAge Pro 2018 software for the analysis. As demonstrated in the Additional file 1 and Fig. 1, the model reflects the natural history of perinatally acquired HBV-infection [13]. We compared two strategies. In the novel strategy (HepB-BD vaccine-plus) all infants receive HepB-BD vaccine (monovalent) within 24 h of delivery and continue on with the pentavalent vaccine (DPT-HiB-HepB) series starting at the age of 6 weeks. We assumed 50% of the target birth cohort will be born in health care facilities and receive the birth dose in a medical setting; following the latest skilled birth attendance rate in Ethiopia [14]. We further assumed that the government rolls-out HepB-BD vaccine to the whole birth cohort and therefore incur costs but vaccine effectiveness would vary depending on the skilled birth attendance rate in Ethiopia. In the current strategy, the birth cohort will only receive the existing pentavalent vaccination schedule at 6, 10 and 14 weeks after birth.

Markov process showing the different health states
In the model, we assumed HepB-BD vaccine would prevent against MTCT of HBV infection during birth/delivery (vertical transmission), otherwise the two strategies would have similar efficacy on infections that occur later in life (horizontal transmissions). We used data on HBV prevalence among pregnant women, vaccine effectiveness, and the risk of perinatal transmission to calculate the percentage of children born with HBV infection. Infected infants either develop acute symptomatic infection with a risk of fulminant hepatitis or remain asymptomatic (Additional file 1). Even though symptomatic acute infections occur less frequently in infants, we accounted for their costs and health consequences in our model (see Additional file 1) [15, 16]. Perinatally infected infants develop acute symptomatic infections early in life, therefore we calculated disability-adjusted life years (DALYs)Footnote 2 (based on life expectancy at birth adjusted for health state valuations from WHO-CHOICE) for only fatal cases and did not account for the lost quality of life for the duration of acute illness [17, 18]. The majority (90%) of the asymptomatic cases and about 33% of those surviving fulminant hepatitis will develop chronic HBV infection [4, 15]. Most perinatally infected individuals enter the immunoactive phase and develop HBeAg positive chronic hepatitis with elevated liver enzyme (alanine aminotransferase) levels only after 10–30 years of infection [19]. Therefore, we started the Markov process at age 20 years. Individuals with chronic HBV infection are simulated within the Markov process either as an inactive carrier or with chronic active hepatitis (CAH). Individuals who do not require antiviral therapy are considered inactive carriers and CAH are those who fulfill the treatment criteria (irrespective of the HBeAg status). A study in Ethiopia has evaluated treatment eligibility and response to antiviral management of chronic hepatitis B infection [20]. In this study, among individuals 18–25 years of age with chronic HBV infection, nearly a quarter of patients (25%) were eligible to antiviral treatment (ALT > 80 U/L and viral load > 2000 IU/mL). Therefore, in our model 75% of the individuals with chronic HBV infection began the Markov process as inactive carriers while 25% as CAH. Even though there are studies that document clearance of HBsAg (in 6–17% of the cases) in Caucasian children who acquired chronic HBV infection horizontally, such data for perinatally infected children in sub-Saharan Africa were lacking where there is limited access to antiviral treatment [21, 22]. Therefore, our model did not account for state transitions from either inactive carriers or CAH to HBsAg clearance (no infection).
We ran the Markov process for 51 cycles, which corresponds to the average life expectancy of both males and females at age 20 years in Ethiopia [17]. Every Markov cycle lasts 1 year allowing infected individuals to pass through different morbid states based on their transition probabilities. In each annual cycle, infected individuals could incur costs related to medical care and health outcomes depending on their health state. Subsequently for each strategy, the costs and effects accrued in each of the decision trees and the Markov cycles are added and compared to calculate the incremental cost-effectiveness ratio (ICER).
Epidemiologic, probability and effectiveness data
The overall prevalence of HBsAg among pregnant women in Ethiopia was estimated at 4.7% [3]. The risk of perinatal transmission varies by the maternal HBeAg status, where HBeAg-positive mothers carry a higher risk of transmission [4]. Prevalence of HBeAg among HBsAg-positive pregnant women in Ethiopia is unknown; therefore we used the mean prevalence from several sub-Saharan African countries [4]. Table 1 summarizes epidemiologic and probability data inputs used in our model. Individuals infected with HBV may develop a spectrum of disease conditions with different probabilities (see Fig. 1 and Additional file 1). Local data on transition probabilities among different health states were not available. Therefore we used data from settings that are similar to the Ethiopian context when available (Table 1) [23, 24]. Similar to what has been used in acute symptomatic infections, DALYs averted were the measure of effectiveness for chronic HBV states, inline with WHO recommendations since chronic HBV infection results in both premature mortality and morbidity [23, 25]. Evidence on disability weights for the different disease states were gathered from the Global Burden of Diseases (GBD) study database but other sources were also sought when such data were not available in the GBD database (Table 2) [24, 26].
Vaccine effectiveness data based on a randomized controlled trial (RCT) were not available locally and from other comparable sub-Saharan African countries. Therefore we used data from other settings that were based on a systematic review of the efficacy of hepatitis B immunization for newborn infants of HBsAg-positive mothers where the protective efficacy of the vaccine was 72% (95% CI 60 to 80%) in preventing perinatal HBV transmission [27]. Vaccine adverse effects that are usually mild were not factored into the model [6]. Deaths due to other causes (background mortality) were integrated in the model using the World Health Organization’s life tables for Ethiopia [17].
Costs
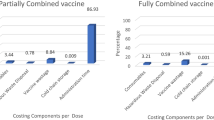
Costs were estimated from a health provider perspective and only included direct medical costs. We estimated the incremental cost of introducing HepB-BD vaccine in its monovalent form. We preferred the monovalent form of the vaccine in order to minimize wastage rates. Both recurrent and capital costs were included using an ingredients-based approach following WHO guidelines [28]. Recurrent costs included costs of vaccines, syringes, safety boxes, transport and maintenance, and cold chain storage while social mobilization and training costs were under capital costs (Table 3). We used the latest UNICEF price data for vaccines, auto-disable (AD) syringes and safety box adjusted for wastage rates and freight costs [29, 30]. Data on wastage rates and freight costs were retrieved from a study on economic evaluation of HBV vaccine in low-income countries [23]. Local data on other aspects of recurrent costs (transport and maintenance and cold chain storage) and capital costs for HepB-BD vaccine were not available therefore we used 2008 estimates from Mozambique adjusted to the 2018 USD values [12, 31].
The medical care costs included initial assessment and diagnosis costs, antiviral drug costs, costs associated with monitoring those on treatment and not on treatment, and cost of managing decompensated cirrhosis (DCC) and hepatocellular carcinoma (HCC) (Table 3). In order to calculate the costs of initial assessment and diagnosis, we used the national guidelines on viral hepatitis to identify required laboratory tests and imaging modalities and frequency of health care visits [11]. We collected laboratory cost data from local sources. The median supplier price for the antiviral drug of choice (Tenofovir) was used to compute for annual drug cost after accounting for transportation costs [32, 33]. Hospital admission cost data for DCC and HCC were not locally available; therefore we used estimates from The Gambia adjusted to the 2018 USD values [31, 34]. Costs for acute symptomatic conditions were based on expert estimates. All costs were expressed in 2018 USD. Both future costs and health outcomes were discounted at 3% annual rate following WHO recommendations [25].
Sensitivity analyses
We conducted a series of one-way sensitivity analyses where we varied key input parameters one at a time over plausible ranges to test the robustness of our findings (Table 1). Based on the findings in a one-way sensitivity analysis, we proceeded and conducted two-way and three-way sensitivity analyses for parameters that are likely to change the result in a critical way. Furthermore, a multivariate sensitivity analysis was conducted using Monte Carlo simulations with n = 10,000 simulation runs. We varied all key parameters (vaccine effectiveness, vaccine utilization, risk of perinatal transmission in HBeAg-mothers, risk of perinatal transmission in HBeAg + mothers, prevalence of HBV infection among mothers, cost of medical care, average cost per vaccinated child, prevalence of HBeAg in pregnant women, transition probability of CAH to inactive carrier state) simultaneously [35]. Lastly, we also ran the model without discounting future health benefits or costs (one at a time), and without discounting both health benefits and costs [35].
Results
Compared to the current strategy, an additional HepB-BD vaccine would have an incremental cost-effectiveness ratio of 110 USD per DALY averted (Table 4). Leaving effects and both effects and costs undiscounted decreased the ICER to 67 USD and 49 USD per DALY averted, respectively.
The one-way sensitivity analyses showed that the ICERs would range from cost savings to maxima of USD625 per DALY averted. The highest ICER was observed for a 10% vaccine utilization, followed by a 2% risk of perinatal transmission when the mother was HBeAg negative and a 2.5% prevalence of HBV infection among mothers with an ICER of USD373 to 328 per DALY averted (Table 5). With two-way sensitivity analyses, we found that various combinations of vaccine effectiveness with other parameters would change the ICER in a substantial way as follows (Table 5). ‘’Vaccine effectiveness’ and ‘average cost per vaccinated child’ an ICER of 262; ‘vaccine effectiveness’ and ‘prevalence of HBV infection among mothers’ an ICER of 421; ‘vaccine effectiveness’ and ‘risk of perinatal transmission when mother was HBeAg negative’ an ICER of USD475 per DALY averted; and ‘Vaccine effectiveness’ and ‘vaccine utilization’ would have ICER of USD663 per DALY averted. The three-way sensitivity analyses also showed that most parameter variations resulted in an ICER value of < USD485 per DALY averted except for some combinations of the following critical parameter inputs: vaccine utilization, risk of perinatal transmission when mother was HBeAg positive, risk of perinatal transmission when mother was HBeAg negative, average cost per vaccinated child and prevalence of HBV infection among mothers with an ICER ranging from USD947 to 1493 per DALY averted. On the contrary, a combination of the following parameters: risk of perinatal transmission when mother was HBeAg negative, annual cost of CAH and prevalence of HBV infection among mothers at their favorable parameter inputs became cost savings (hence ICER < 0). The univariate sensitivity analysis demonstrated that introducing HepB-BD vaccine in Ethiopia is less likely to be highly cost-effective (at a threshold of 0.31 times the GDP per capita in Ethiopia, USD240 in 2018) when the vaccine utilization drops below 35% [36, 37].
Figure 2 shows the results of the probabilistic sensitivity analysis and the uncertainty surrounding our cost-effectiveness estimates, with overlapping costs and effectiveness ranges. Regardless, the distribution pattern is relatively distinct with higher costs and effectiveness for the novel strategy (with birth dose). The willingness-to-pay (WTP) threshold has an impact on the probability of intervention being cost-effective. At WTP threshold of greater than US$110 per DALYs averted, the four-dose regimen (with birth dose) is most likely to be cost-effective.

Probabilistic sensitivity analysis (n = 10,000 simulations)
For a birth cohort of 3.34 million in 2018 in Ethiopia, we calculated a total of 10,020 DALYs would be averted at a cost of nearly USD 2.5 million for HBV vaccine introduction (without accounting for the cost saving from prevention of disease states) [38].
Discussion
We conducted a cost-effectiveness analysis of HepB-BD vaccine in its monovalent form (compared with current practices) in Ethiopia and found incremental cost-effectiveness ratio of USD110 per DALY averted. The ICER for HepB-BD is lower than the willingness-to-pay thresholds suggested by Ochalek J et al. < 0.31 times the GDP per capita in Ethiopia [37]. This makes investing in HepB-BD vaccine highly cost-effective in an Ethiopian setting, especially in light of the cost-effectiveness of comparable interventions for low-income countries in sub-Saharan Africa [39,40,41]. Our cost-effectiveness findings remained robust to a number of sensitivity analyses (e.g. Table 5). Among the key parameters tested in sensitivity analyses, vaccine utilization was the main driver behind the cost-effectiveness results, followed by risk of perinatal transmission associated with HBeAg status, average cost per vaccinated child, prevalence of HBV infection among mothers, and treatment cost of CAH. In addition, our findings are comparable to those of other studies that studied the cost-effectiveness of birth dose of HB vaccine in Mozambique [12, 42].
Despite demonstrating that HepB-BD vaccine is highly cost-effective in an Ethiopian setting, our analysis presents a number of important limitations. First, local data on vaccine effectiveness, health state transition probabilities, and the cost of different health states were not readily available which may decrease the accuracy behind our ICER estimates. Second, we only assessed the cost of tenofovir as the treatment of choice in our analysis but using other drugs such as entecavir might be an alternative cost-effective therapy [43]. Treatment of chronic HBV infection with entecavir consumes more resources as compared to treatment with tenofovir, which might have resulted in a less cost-effective estimate in our analysis [44]. Due to lack of community-based data on treatment eligibility, we used a study conducted in a hospital setting, which might over represent symptomatic cases [20]. Third, some aspects of vaccine delivery costs (such as transport and maintenance, cold chain storage and capital costs) were based on estimates from other settings that may not reflect the reality in Ethiopia. Fourth, another important limitation is associated with limiting vaccine delivery in the medical setting. Skilled birth attendance rate is low and many women in Ethiopia give birth at home without skilled assistance, especially those women residing in rural areas [14]. Making HBV vaccine accessible to the whole population might require a community-level engagement, which might have additional cost implications. Cost estimates of such outreach strategies were not available and not included in our model. Including the cost of outreach strategies in the analysis may result in higher ICER related to additional resource requirements such as transport, fuel and staff allowance [45]. We also assumed that additional health professionals would not be required to administer the birth dose of HB vaccine and therefore we have not included related costs. Even though health work force per population is low in Ethiopia, recent evidence suggests that there is underutilization of available health workforce in the country [46, 47]. Lastly, there may be additional important benefits such as the equity benefits of vaccinations including the prevention of expensive out-of-pocket medical treatment for liver cancer and associated medical impoverishment into the future [48].
Successful implementation of HepB-BD vaccine is largely dependent on the timing of its administration. Timely administration (within 24 h of birth) of the vaccine may require integration with maternal and child health (MCH) programs rather than through the Expanded Program on Immunization (EPI). The suggested change in the delivery of HepB-BD vaccine requires redesigning the MCH (immediate post-partum services) and EPI programs and could include other birth dose vaccines such as Bacille Calmette-Guérin (BCG) and the birth dose of oral polio vaccine (OPV-0). This will entail not only additional work on midwives (or other health personnel rendering immediate post-partum services) but also logistic implications for vaccine storage and delivery within the maternity setting. Further, this might require training of health personnel and awareness-raising campaigns nationally in Ethiopia. With additional efforts on social mobilization, the introduction of HepB-BD vaccine may positively contribute to the improvement in the coverage of skilled birth attendance and other birth dose vaccines in Ethiopia.
Besides, resources for health care are scarce in Ethiopia. The total health expenditure per capita in Ethiopia was about US$33 for the years 2016/2017 [49]. The annual budget required to introduce the birth dose of HBV vaccine in Ethiopia costs an additional 0.023 US$ per capita which is nearly 0.1% of the 2016/17 annual total health expenditure (3.1 billion US$) for Ethiopia. In the last decade, Ethiopia has enjoyed a substantial economic development and aspires to be a middle-income country by 2035 [50]. Along with the economic development, the government of Ethiopia envisions to attain population health status commensurate with the best performing middle-income countries [50]. Realization of such ambitious targets requires the government’s commitment for more health care resource allocations.
Conclusions
Birth dose of HB vaccine is one of the most important preventive strategies recommended by the WHO and the national viral hepatitis control and prevention guidelines in Ethiopia. Given the formidable resource constraints in low-income countries such as Ethiopia, evidence on cost-effectiveness of interventions is vital towards setting priorities. Currently, the Ethiopian government is revising its essential health services package (EHSP). Given the substantial health dividend in investing in the birth dose of HB vaccine in Ethiopia and the fact that it is highly cost-effective, it should be considered for inclusion in the Ethiopia’s EHSP.
Notes
The endemicity of hepatitis B virus is determined by the prevalence of HBsAg in the general population of a defined geographic area: prevalence of HBsAg > 8% is high endemicity, 2–7% intermediate endemicity, and HBsAg prevalence < 2% is low endemicity [6].
Most of the deaths from perinatally acquired acute fulminant hepatitis occur during infancy. Using a life table for Ethiopia, adjusted for health state valuations, we computed the DALYs lost associated with each death (54.3 years). This value was used in the model to quantify the DALYs lost associated with deaths due to fulminant hepatitis.
Abbreviations
- ALT:
-
Alanine aminotransferase
- CAH:
-
Chronic active hepatitis
- CEA:
-
Cost-effectiveness analysis
- DALYs:
-
Disability adjusted life years
- DCC:
-
Decompensated cirrhosis
- EPI:
-
Expanded program on immunization
- FMOH:
-
Federal ministry of health
- HBeAg:
-
Hepatitis B virus envelope antigen
- HBsAg:
-
Hepatitis B surface antigen
- HBV:
-
Hepatitis B virus
- HCC:
-
Hepatocellular carcinoma
- HepB-BD:
-
Birth dose of hepatitis B
- ICER:
-
Incremental cost-effectiveness ratio
- MCH:
-
Maternal and child health
- MTCT:
-
Mother to child transmission
- UNICEF:
-
United nation children’s fund
- WHO:
-
World Health Organization
References
World Health Organization. Global Hepatitis Report 2017. Geneva: World Health Organization; 2017.
Belyhun Y, Maier M, Mulu A, Diro E, Liebert UG. Hepatitis viruses in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2016. https://doi.org/10.1186/s12879-016-2090-1.
Kebede KM, Abateneh DD, Belay AS. Hepatitis B virus infection among pregnant women in Ethiopia: a systematic review and meta-analysis of prevalence studies. BMC Infect Dis. 2018. https://doi.org/10.1186/s12879-018-3234-2.
Edmunds WJ, Medley GF, Nokes DJ, et al. Epidemiological patterns of hepatitis B virus (HBV) in highly endemic areas. Epidemiol Infect. 1996;117:313–25.
Tegegne D, Desta K, Tegbaru B, Tilahun T. Seroprevalence and transmission of hepatitis B virus among delivering women and their new born in selected health facilities, Addis Ababa, Ethiopia: a cross sectional study. BMC Res Notes. 2014;7(1):239.
World Health Organization. Hepatitis B vaccines-WHO position paper. Wkly Epidemiol Rec. 2009;84(40):405–20.
Cui F, Li L, Hadler SC, et al. Factors associated with effectiveness of the first dose of hepatitis B vaccine in China: 1992–2005. Vaccine. 2010;28(37):5973–8.
Federal Democratic Republic of Ethiopia Ministry of Health. Health Sector Transformation Plan (HSTP) (2015/2016–2019/2020). Addis Ababa: Federal Ministry of Health; 2015.
Shimakawa Y, Lemoine M, Njai HF, et al. Natural history of chronic HBV infection in West Africa: a longitudinal population-based study from The Gambia. Gut. 2016. https://doi.org/10.1136/gutjnl-2015-309892.
World Health Organization. SDG 3: ensure healthy lives and promote wellbeing for all at all ages. 2019. https://www.who.int/sdg/targets/en/. Accessed 14 May 2019.
Federal Democratic Republic of Ethiopia. National guideline for prevention and control of viral hepatitis in Ethiopia. Addis Ababa: Federal Ministry of Health; 2016.
Klingler C, Thoumi AI, Mrthinjayam VS. Cost-effectiveness analysis of an additional birth dose of hepatitis B vaccine to prevent perinatal transmission in a medical setting in Mozambique. Vaccine. 2012;31:252–9.
Fattovich G. Natural history of hepatitis B. J Hepatol. 2003;39(Suppl 1):50–8.
Ethiopian Public Health Institute [Ethiopia] and ICF. Ethiopia Mini-Demographic and Health Survey 2019: Key Indicators. Rockville: EPHI and ICF; 2019.
Margolis HS, Coleman PJ, Brown RE, et al. Prevention of hepatitis B virus transmission by immunization. An economic analysis of current recommendations. JAMA. 1995;20(4):992–1000.
de Franchis R, Hadengue A, Lau G, et al. EASL international consensus conference on hepatitis B, 13–14 September, 2002, Geneva, Switzerland Consensus statement (long version). J Hepatol. 2003;39(Suppl 1):3–25.
World Health Organization. Global Health Observatory, Life tables. 2019. http://apps.who.int/gho/athena/data/GHO/LIFE. Accessed 8 Jan 2019.
World Health Organization. Cost-effectiveness and Strategic Planning (WHO-CHOICE): Health State Valuation. 2018. http://www.who.int/choice/demography/health_valuations/en/. Accessed 22 May 2018.
Ribeiro RM, Lo A, Perelson AS, et al. Dynamics of hepatitis B virus infection. Microbes Infect. 2002;4:829–35.
Desalegn H, Abera H, Berhe N, et al. Treatment of chronic hepatitis B in sub-Saharan Africa: 1-year results of a pilot program in Ethiopia. BMC Med. 2018. https://doi.org/10.1186/s12916-018-1229-x.
Bortolotti F, Guido M, Bartolacci S, et al. Chronic hepatitis B in children after e antigen seroclearance: final report of a 29-year longitudinal study. Hepatology. 2006;43:556–62.
Bortolotti F, Jara P, Crivellaro C, et al. Outcome of chronic hepatitis B in Caucasian children during a 20-year observation period. J Hepatol. 1998;29:184–90.
Kim SY, Salomon JA, Goldie SJ. Economic evaluation of hepatitis B vaccination in low-income countries: using cost-effectiveness affordability curves. Bull World Health Organ. 2007;85(11):833–42.
Fan L, Owusu-Edudei K Jr, Schillie SF, Murphy TV. Cost-effectiveness of active-passive prophylaxis and antiviral prophylaxis during pregnancy to prevent perinatal hepatitis B virus infection. Hepatology. 2016;63(5):1471–80.
Tan-Torres Edejer T, Baltussen R, Adam T, et al. Making choices in health WHO guide to cost-effectiveness analysis. Geneva: World Health Organization; 2003.
Institute of Health Metrics and Evaluation (IHME). Global Burden of Disease 2017: Disability weights. 2018. http://ghdx.healthdata.org/record/ihme-data/gbd-2017-disability-weights. Accessed 8 Nov 2018.
Lee C, Gong Y, Brok J, et al. Hepatitis B immunisation for newborn infants of hepatitis B surface antigen-positive mothers. Cochrane Database Syst Rev. 2006;2:004790.
World Health Organization. Guidelines for estimating costs of introducing new vaccines into the national immunization system. Geneva: World Health Organization; 2002.
UNICEF. Supplies and logistics. Vaccine price Data. HepB. 2019. https://www.unicef.org/supply/files/2018_03_01_HepB.pdf. Accessed 19 Feb 2019.
UNICEF. 2019. Supplies and logistics. Auto-Disable (AD) and Re-Use Prevention (RUP) Syringes and Safety Boxes—current price data.
US inflation Calculator. 2019. https://www.usinflationcalculator.com/. Accessed 19 Feb 2019.
Management Science for Health (MSH). International Drug Price Indicator Guide. 2015 Edition. 2016. http://www.msh.org/blog/2014/07/30/2013-international-drug-price-indicator-guide-now-available. Accessed 1 Feb 2018.
World Health Organization. Health Services Delivery Costs. 2018. http://www.who.int/choice/cost-effectiveness/inputs/health_service/en/. Accessed 20 Feb 2019.
Nayagam S, Conteh L, Sicuri E, et al. Cost-effectiveness of community-based screening and treatment for chronic hepatitis B in The Gambia: an economic modeling analysis. Lancet Glob Health. 2016;4:e568–78.
Briggs A. Probabilistic analysis of cost-effectiveness models: statistical representation of parameter uncertainty. Value Health. 2005;8:1–2.
World Bank. GDP per capita (Current US$) 2019. 2019. https://data.worldbank.org/indicator/NY.GDP.PCAP.CD. Accessed 19 July 2019.
Ochalek J, Lomas J, Claxton K. Estimating health opportunity costs in low-income and middle-income countries: a novel approach and evidence from cross-country data. BMJ Glob Health. 2018. https://doi.org/10.1136/bmjgh-2018-000964.
The Government of Federal Democratic Republic of Ethiopia. 2017. Proposal for Support Submitted to the Global Alliance for Vaccines and Immunization (GAVI) and The Vaccine Fund. Addis Ababa, Ethiopia: Federal Ministry of Health. Woods B, Revill P, Sculpher M, et al. Country-Level Cost-Effectiveness Thresholds: Initial Estimates and the Need for Further Research. Value Health. 2016;https://doi.org/10.1016/j.jval.2016.02.017.
Laxminarayan R, Mills AJ, Breman JG, et al. Advancement of global health: key messages from the disease control priorities project. Lancet. 2006;367(9517):1193–208.
Memirie ST, Tolla MT, Desalegn D, et al. A cost-effectiveness analysis of maternal and neonatal health interventions in Ethiopia. Health Policy Plann. 2019. https://doi.org/10.1093/heapol/czz034.
Tolla MT, Norheim OF, Memirie ST, et al. Prevention and treatment of cardiovascular disease in Ethiopia: a cost-effectiveness analysis. Cost Eff Resour Alloc. 2016;14:10.
Griffiths UK, Hutton G, Pascoal EDD. The cost-effectiveness of introducing hepatitis B vaccine into infant immunization services in Mozambique. Health Policy Plann. 2005;20(1):50–9.
Hill A, Gotham D, Cooke G, et al. Analysis of minimum target prices for production of entecavir to treat hepatitis B in high-and low-income countries. J Virus Erad. 2015;1:103–10.
Ruggeri M, Basile M, Coretti S, et al. Economic analysis and budget impact of tenofovir and entecavir in the first-line treatment of hepatitis B virus in Italy. Appl Health Econ Health Policy. 2017;15:479–90.
World Health Organization. In-depth evaluation of the reaching every district approach in the African region. Reaching every district approach in the African region valuation report, 2007.
Mann C, Dessie E, Adugna M, and Berman P. 2016. Measuring efficiency of public health centers in Ethiopia. Harvard T.H. Chan School of Public Health and Federal Democratic Republic of Ethiopia Ministry of Health. Boston, Massachusetts and Addis Ababa, Ethiopia.
Mann C, Dessie E, Adugna M, Berman P. 2016. Measuring efficiency of public primary hospitals in Ethiopia. Harvard T.H. Chan School of Public Health and Federal Democratic Republic of Ethiopia Ministry of Health. Boston, Massachusetts and Addis Ababa, Ethiopia.
Chang AY, Riumallo-Herl C, Perales NA, et al. The equity impact vaccines may have on averting deaths and medical impoverishment in developing countries. Health Aff. 2018;37(2):316–24.
Federal Democratic Republic of Ethiopia Ministry of Health. Ethiopia Health Accounts 2016/2017. Addis Ababa: Ministry of Health; 2019.
Admasu K, Tamire A, Tsegaye S. Envisioning the future of the health sector: an update. Federal Democratic Republic of Ethiopia Ministry of Health Quarterly Health Bulletin. 2014;6:3–12.
Acknowledgements
We would like to thank the research advisory council of the maternal and child health directorate of the Federal Ministry of Health, Ethiopia for their constructive feedback in the development of the manuscript. We are also grateful to Stéphane Verguet for valuable comments and edits on the manuscript.
Funding
This work was supported by the Bill & Melinda Gates Foundation through the Disease Control Priorities-Ethiopia project [OPP1162384] and Fenot-Harvard T. H. Chan School of Public Health, Ethiopia Project [OPP1135922].
Author information
Authors and Affiliations
Contributions
STM, TG, YT and MN initiated the study. STM conceptualized and coordinated the research and did the analysis with TG. HD, MN and MNa helped with the acquisition of data. STM wrote the first draft of the manuscript. TG, HM, YT, LT, MZ, FT, MNa, and MN reviewed the manuscript and provided advice and suggestions. STM had final responsibility to submit for publication. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was not required for this study as it is based on publicly available data. The study didn’t involve individual level data.
Consent for publication
All authors read and approved the final manuscript.
Competing interests
The funding agents had no role in the design, analysis and write-up of the manuscript. The views expressed in the manuscript reflect only the authors’ view and not that of any organization. The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Decision tree structure.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Memirie, S.T., Desalegn, H., Naizgi, M. et al. Introduction of birth dose of hepatitis B virus vaccine to the immunization program in Ethiopia: an economic evaluation. Cost Eff Resour Alloc 18, 23 (2020). https://doi.org/10.1186/s12962-020-00219-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12962-020-00219-7