
Abstract
Background
Carcinoembryonic antigen (CEA) is one of the most widely used tumor markers, and its value in the surveillance of post-operative colorectal cancer is well established. Fluorodeoxyglucose-positron emission tomography (FDG-PET) has been clinically used in colorectal cancer imaging including preoperative staging, evaluation of therapeutic response, detection of disease recurrence, and investigation of unexplained rising tumor markers.
Case presentation
We report a case of resected colorectal cancer presented with rising CEA levels in 5 years, and FDG-PET revealed no definitive evidence of recurrence except abnormal focal FDG uptake in the right thyroid lobe. However, fine needle aspiration cytology (FNAC) of the thyroid nodule showed negative for malignancy. Progressively rising CEA levels were noted over the following 5 years, but serial follow-up examinations did not find evidence of recurrence. Fluorodeoxyglucose-positron emission tomography/computed tomography (FDG-PET/CT) was performed subsequently and again showed focal FDG uptake in the right thyroid lobe. This time, FNAC revealed positive for malignancy, in favor of medullary thyroid carcinoma (MTC). The patient underwent total thyroidectomy and modified radical neck dissection, and MTC with cervical nodal metastasis (pT3N1) was diagnosed. He had cervical lymph nodes recurrence 2 years later, which was resected.
Conclusions
This case reminded us that FDG-PET/CT may detect occult tumors resulting in CEA elevation other than colorectal cancer. Moreover, FNA has a higher false negative rate in detecting MTC than other forms of thyroid cancer. Repeat FNAC for the initial negative cytology result and measure of serum calcitonin for the early MTC detection could be more helpful to avoid the delay in MTC diagnosis.
Similar content being viewed by others


Background
Carcinoembryonic antigen (CEA) is one of the most widely used tumor markers, and its value in the surveillance of post-operative colorectal cancer is well established [1, 2]. However, it is also overexpressed in many different tumors, such as lung cancer and neuroendocrine pancreatic tumor. Fluorodeoxyglucose-positron emission tomography (FDG-PET) has several well-recognized applications in colorectal cancer imaging including preoperative staging, evaluation of therapeutic response, detection of disease recurrence, and investigation of unexplained rising tumor markers [3, 4]. In addition, the whole body scan of FDG-PET may detect occult metachronous tumors.
Case presentation
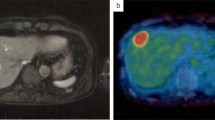
A 56-year-old man with a history of colorectal cancer (CRC) status post curative resection presented with high serum CEA level up to 68 μg/L (normal limit < 5 μg/L, measured by radioimmunoassay) 5 years after surgery. To investigate for possibility of cancer recurrence, distant metastasis, or other tumors, we performed FDG-PET (Siemens Ecat Exact HR+ scanner). It demonstrated mildly focal increased FDG uptake in the right lobe of the thyroid gland, and maximum standardized uptake value (maxSUV) was 2.5 (Fig. 1). We did not observe other pathologic FDG uptake in the PET images. Therefore, the patient underwent ultrasound-guided fine needle aspiration (FNA) of the hypermetabolic thyroid nodule, and the cytology revealed negative for malignancy.

The first time FDG-PET scan of the patient of resected colorectal cancer with elevated CEA level (68 µg/L) showed focal FDG uptake in the right thyroid lobe (arrow)
Progressively rising CEA levels up to 184 μg/L were noted over the following 5 years. However, serial follow-up abdominal ultrasound, computed tomography (CT), and colonoscopy did not find evidence of recurrent disease of CRC. Subsequently, we performed FDG-PET/CT (GE Discovery LS PET/CT hybrid scanner) again and observed a hypermetabolic focus in the right thyroid lobe (maxSUV 3.5), which corresponded to the hypodense nodule and calcification shown on CT images (Fig. 2). This time, repeat FNA of the thyroid was done and revealed positive for malignancy, in favor of medullary thyroid cancer (MTC). The patient underwent bilateral total thyroidectomy and modified radical neck dissection. The histopathology revealed right thyroid medullary carcinoma with a tiny microscopic focus suggesting papillary carcinoma (pT3). Two right neck lymph nodes are metastasized by medullary carcinoma (pN1). The CEA level dropped to 30 μg/L two and a half months after surgery.

The second time FDG-PET/CT scan of the same patient with progressively elevated CEA levels up to 184 µg/L showed persistent focal FDG uptake in the right thyroid lobe (arrow), corresponding to the hypodense nodule and calcification shown on CT
The subsequent follow-up showed fluctuating CEA levels (3.7 ~ 15.5 μg/L) and progressively rising calcitonin levels (up to 843 ng/L) in the first year to the second year after surgery. Ultrasound and FNAC revealed recurrent cervical lymphadenopathy. The patient received lymph nodes dissection and recurrent nodal metastasis from MTC which was proven. At this point, the patient continued regular follow-up in our hospital and the CEA and calcitonin levels remained within normal limits.
Discussion
CEA is a glycoprotein present in normal mucosal cells, and its increased serum level is associated with adenocarcinoma, especially CRC. CEA level is useful in assessing prognosis, detecting recurrence, and monitoring treatment in patients with CRC [1, 2]. However, it may be elevated in a wide variety of other tumors and benign conditions, such as MTC, lung cancer, neuroendocrine pancreatic tumor, smoking, and infections. A recent systematic review has raised some doubts about the clinical usefulness of CEA in detecting recurrence after intended curative surgery for CRC, which included a total of 42 studies and 9834 CEA testing outcomes during follow-up [5]. Results point toward that CEA did not effectively detect treatable recurrences at an early stage. Besides, the low reliability of positive predictive value may lead to the high false positive rate. Therefore, considerations of factors and diseases known to influence CEA results and identification whether the increase in CEA is part of a fluctuating pattern or if it rises progressively are necessary.
FDG-PET and FDG-PET/CT are widely used for diagnosis, staging, evaluating therapeutic response, and detecting recurrence of a wide variety of cancers, including CRC. Many studies have demonstrated the value of PET in the detection of CRC recurrence in the post-operative patients with rising CEA [6,7,8]. Sometimes, the full-body scan of FDG-PET may detect occult synchronous or metachronous tumors. Focal FDG uptake within the thyroid gland can be associated with malignancy, most commonly papillary thyroid carcinoma [9]. Chen et al. had described thyroid incidentaloma identified by FDG-PET occurred with a frequency of 1.2% in 4803 physical check-up examinees, and 14% were proven to be malignant (all papillary carcinomas) [10]. Therefore, a hypermetabolic nodule in the thyroid gland could be either benign or malignant etiology, and further work-up with an ultrasound, FNA, or excisional biopsy is necessary.
The ultrasound-guided FNA of thyroid is a safe, inexpensive, minimally invasive procedure for determining thyroid malignancy and is an integral part of thyroid nodule evaluation. Limitations of FNA are related to the skill of the operator and the expertise of the cytopathologist. In a review of seven large series totaling 18,183 thyroid FNAs, Gharib et al. found the sensitivity of FNA for diagnosis of thyroid cancer ranges from 65 to 98% (mean, 83%), specificity ranges from 72 to 100% (mean, 92%), false negative rate ranges from 1 to 11% (mean 5%), and false positive rate ranges from 1 to 8% (mean 2.9%) [11]. According to the 2015 American Thyroid Association’s guidelines [12], repeat FNAC should be undertaken for the initial non-diagnostic cytology result of thyroid nodule in order to reduce the risk of false negative results.
MTC is a rare neuroendocrine malignancy arising from calcitonin-secreting parafollicular C cells in the thyroid gland. It accounts for approximately 3 to 10% of all thyroid neoplasms [13]. Reported sensitivity of FNA for diagnosis of MTC ranges from 53 to 89%, which is less than that of all thyroid cancer. On the other hand, serum calcitonin has an excellent sensitivity in diagnosing MTC from 98 to 99% [14, 15]. Serum CEA is another useful biomarker for MTC, especially in patients with poorly differentiated or metastatic MTC who may not have elevated serum calcitonin level [14]. Nevertheless, CEA level does not have the specificity of calcitonin for MTC. Calcitonin is a hormone produced and secreted by thyroid C cells specifically. Therefore, serum calcitonin levels can be determined as a highly specific biomarker for the early diagnosis of MTC [16]. Overall, FDG-PET/CT is less sensitive in MTC patients with de-differentiated tumors, whereas it is more sensitive in patients with high serum calcitonin (> 1000 ng/L) and short calcitonin doubling times (< 24 months) [17].
The patient’s history of resected CRC with high-serum CEA levels made us focus on searching recurrence or metastasis of CRC and overlook other disease causing elevated CEA level. If we checked his serum calcitonin while FDG-PET revealing hypermetabolic thyroid nodule or performed repeat FNAC in the next 3 months after initial negative cytology result, the delay in MTC diagnosis and treatment would have been avoided, and the disease might not spread to the cervical lymph nodes.
Conclusion
FDG-PET/CT has emerged as a powerful imaging tool for the detection of the recurrence of colorectal cancers with rising serum CEA levels. The full-body scan of PET/CT may detect occult tumors that result in CEA elevation, such as MTC. This case reminds us that focal FDG uptake in the thyroid gland with elevated CEA level can be associated with MTC. Moreover, FNA has a higher false negative rate in detecting MTC than other forms of thyroid cancer. In this case, repeat FNA and measure of serum calcitonin could be most helpful in early detection of MTC.
Abbreviations
- CEA:
-
Carcinoembryonic antigen
- CRC:
-
Colorectal cancer
- CT:
-
Computed tomography
- FDG-PET:
-
Fluorodeoxyglucose-positron emission tomography
- FNA:
-
Fine needle aspiration
- maxSUV:
-
Maximum standardized uptake value
- MTC:
-
Medullary thyroid cancer
References
Fakih MG, Padmanabhan A. CEA monitoring in colorectal cancer. What you should know. Oncology (Williston Park). 2006;20:579–87.
Sturgeon CM, Lai LC, Duffy MJ. Serum tumour markers: how to order and interpret them. BMJ. 2009;339:b3527.
Petersen RK, Hess S, Alavi A, Høilund-Carlsen PF. Clinical impact of FDG-PET/CT on colorectal cancer staging and treatment strategy. Am J Nucl Med Mol Imaging. 2014;4:471–82.
de Geus-Oei LF, Ruers TJ, Punt CJ, et al. FDG-PET in colorectal cancer. Cancer Imaging. 2006;6:S71–81.
Sørensen CG, Karlsson WK, Pommergaard HC, et al. The diagnostic accuracy of carcinoembryonic antigen to detect colorectal cancer recurrence—a systematic review. Int J Surg. 2016;25:134–44.
Zervos EE, Badgwell BD, Burak WE Jr, et al. Fluorodeoxyglucose positron emission tomography as an adjunct to carcinoembryonic antigen in the management of patients with presumed recurrent colorectal cancer and nondiagnostic radiologic workup. Surgery. 2001;130:636–43.
Flamen P, Hoekstra OS, Homans F, et al. Unexplained rising carcinoembryonic antigen (CEA) in the postoperative surveillance of colorectal cancer: the utility of positron emission tomography (PET). Eur J Cancer. 2001;37:862–9.
Flanagan FL, Dehdashti F, Ogunbiyi OA, et al. Utility of FDG-PET for investigating unexplained plasma CEA elevation in patients with colorectal cancer. Ann Surg. 1998;227:319–23.
Marcus C, Whitworth PW, Surasi DS, et al. PET/CT in the management of thyroid cancers. AJR Am J Roentgenol. 2014;202:1316–29.
Chen YK, Ding HJ, Chen KT, et al. Prevalence and risk of cancer of focal thyroid incidentaloma identified by 18F-fluorodeoxyglucose positron emission tomography for cancer screening in healthy subjects. Anticancer Res. 2005;25:1421–6.
Gharib H, Goellner JR. Fine-needle aspiration biopsy of the thyroid: an appraisal. Ann Int Med. 1993;118:282–9.
Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133.
Hundahl SA, Fleming ID, Fremgen AM, Menck HRA. National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985-1995. Cancer. 1998;83:2638–48.
Ganeshan D, Paulson E, Duran C, et al. Current update on medullary thyroid carcinoma. AJR Am J Roentgenol. 2013;201:W867–76.
Simões-Pereira J, Bugalho MJ, Limbert E, Leite V. Retrospective analysis of 140 cases of medullary thyroid carcinoma followed-up in a single institution. Oncol Lett. 2016;11:3870–4.
van Veelen W, de Groot JW, Acton DS, et al. Medullary thyroid carcinoma and biomarkers: past, present and future. Intern Med. 2009;266(1):126–40.
Ong SC, Schöder H, Patel SG, et al. Diagnostic accuracy of 18F-FDG PET in restaging patients with medullary thyroid carcinoma and elevated calcitonin levels. J Nucl Med. 2007;48:501–7.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Author information
Authors and Affiliations
Contributions
SWC contributed to the acquisition and analysis of the data and images of the patient and was a major contributor in writing the manuscript. YKC revised the manuscript critically for important intellectual content. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chen, SW., Chen, YK. High CEA levels in a case of resected colorectal cancer: delayed diagnosis of metachronous medullary thyroid cancer. World J Surg Onc 15, 230 (2017). https://doi.org/10.1186/s12957-017-1303-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-017-1303-4