
Abstract
Background
Previous studies suggested that baseline white blood cell count and apolipoprotein A1 levels were associated with clinical outcomes in patients with coronary heart disease (CAD) who underwent percutaneous coronary intervention (PCI). However, the ratio of baseline white blood cell count-to-apolipoprotein A1 level (WAR) and CAD after PCI have not been investigated. The present study investigated the effects of baseline WAR on long-term outcomes after PCI in patients with CAD.
Methods
A total of 6050 patients with CAD who underwent PCI were included in the study. Of these, 372 patients were excluded because no baseline white blood cell counts or apolipoprotein A1 (ApoA1) data was available or because of malignancies or other diseases. Finally, 5678 patients were enrolled in the present study and were divided into 3 groups according to WAR value: lower group - WAR< 5.25 (n = 1889); median group - 5.25 ≤ WAR≤7.15 (n = 1892); and higher group - WAR≥7.15 (n = 1897). The primary endpoint was long-term mortality, including all-cause mortality (ACM) and cardiac mortality (CM), after PCI. The average follow-up time was 35.9 ± 22.6 months.
Results
A total of 293 patients developed ACM, including 85 (4.5%) patients in the lower group, 90 (4.8%) patients in the median group, and 118 (6.2%) patients in the higher group. The risk of ACM, cardiac mortality (CM), major adverse cardiovascular and cerebrovascular events (MACCEs), and major adverse cardiovascular events (MACEs) increased 62.6% (hazard risk [HR] =1.626, 95%CI: 1.214–2.179, P = 0.001), 45.5% (HR = 1.455, 95%CI: 1.051–2.014, P = 0.024), 21.2% (HR = 1.212, 95%CI: 1.011–1.454, P = 0.038), and 23.8% (HR = 1.238, 95%CI: 1.025–1.495, P = 0.027), respectively, as determined by multivariate Cox regression analyses comparing the patients in the higher group to patients in the lower group. Patients with a WAR≥4.635 had 92.3, 81.3, 58.1 and 58.2% increased risks of ACM, CM, MACCEs and MACEs, respectively, compared to the patients with WAR< 4.635. Every 1 unit increase in WAR was associated with 3.4, 3.2, 2.0 and 2.2% increased risks of ACM, CM, MACCEs and MACEs, respectively, at the 10-year follow-up.
Conclusion
The present study indicated that baseline WAR is a novel and an independent predictor of adverse long-term outcomes in CAD patients who underwent PCI.
Similar content being viewed by others

Introduction
A large number of epidemiological and clinical studies have shown that the inflammatory response is closely related to the occurrence and development of coronary artery disease (CAD) [1,2,3,4]. Inflammation plays an increasingly important role in major cardiac adverse events (MACE). White blood cell (WBC) count is an inflammatory marker in routine blood tests, and it has a negligible effect on the clinical outcomes of patients with CAD. As early as the 1980s, Schlant et al. observed an increase in WBC count as an indicator of mortality in patients with myocardial infarction [5]. Lao D et al. further demonstrated that leukocytosis is an independent predictor in CAD patients after PCI [6]. A large number of recent studies confirmed that the increase in baseline WBC count is associated with the occurrence of adverse clinical outcomes after PCI in patients with CAD [7,8,9].
Epidemiological study demonstrated a strong negative correlation between high-density lipoprotein (HDL) levels and atherosclerosis [10]. ApoA-1 is a main protein component of HDL, and it showed a similar negative correlation. A large number of preclinical studies support epidemiological data from animal models of atherosclerosis, which suggest that HDL/apoA-1 intervention reduces plaque size and inflammation [11,12,13,14,15]. Lower HDL levels (< 0.91 mmol/l) doubled patient mortality in patients with PCI compared to patients with higher HDL levels (1.24 to 3.1 mmol/l) [16, 17]. ApoA-1 perfusion reduces endometrial formation and vein grafting after carotid artery injury in mice [18] and enhances the re-endothelialization of endothelial injury sites [19]. Studies directly evaluated the effect of apoA-1 systemic perfusion on stent biocompatibility and found that ApoA-1 was associated with a reduction in-stent restenosis and platelet activation and an increase in endothelialization [20].
Previous study has indicated that elevated serum apoA-1 levels may be associated with decreased levels of high-sensitivity C-reactive protein and decreased WBC counts, which may be inflammatory biomarkers for the onset of CAD [21]. Elevated levels of WBC and decreased levels of apoA-1 may be useful markers of CAD risk. However, there are few reports on the correlation between baseline WBC-to-ApoA1 ratios (WAR) and the occurrence and prognosis of CAD. The present study assessed the predictive effect of baseline WAR on long-term outcomes of CAD patients who underwent PCI.
Patients and methods
Study population
This study was a single-center retrospective cohort study that investigated the clinical outcomes and risk factors for patients with CAD after PCI (CORFCHD-PCI). In the CORFCHD-PCI study, we collected clinical, angiographic, short-term and long-term outcome data of CAD patients who underwent PCI in the First Affiliated Hospital of Xinjiang Medical University from January 2008 to December 2016. The details of the design are registered at http://www.chictr.org.cn (ChiCTR-ORC-16010153). In the CORFCHD-PCI study, 6050 CAD patients were recruited. The average follow-up period was 35.9 months, and 102 patients were lost during follow-up. The selected criterion for CAD was at least one coronary artery diameter stenosis ≥70%, as confirmed on coronary angiography. An experienced cardiologist performed PCI. The following exclusion criteria for the study were used: 1) preoperative baseline WBC count or ApoA1 data were not be acquired; 2) systemic disease, malignant tumor, inflammatory disease, acute infectious disease, or severe kidney disease; and 3) taking drugs that affect leukocytes before admission. The present study excluded 372 patients for unavailable WBC or apoA1, acute infections, malignancies, or hepatobiliary disease. Finally, 5678 patients were included the present study. In these 5678 patients, 256 patients have previous CAD history and none of these interventions has coronary artery bypass grafting (CABG) vessel. We divided these patients into 3 groups according to WAR values: lower group - WAR< 5.25 (n = 1889); median group - 5.25 ≤ WAR< 7.15 (n = 1892); and higher group - WAR≥7.15 (n = 1897). WAR was calculated as the ratio of baseline WBC count to ApoA1 from the same blood sample.
Data collection
We collected general demographic data for patients, including smoking, drinking, past medical history, cardiovascular risk factors, and laboratory-related tests. All laboratory-related tests were performed on the second day after admission after fasting for at least 12 h. Serum concentration of blood urea nitrogen (BUN), creatinine (Cr), uric acid (UA), total cholesterol (TC), triglyceride (TG), glucose (GLU), high-density lipoprotein-C (HDL-C), low-density lipoprotein-C (LDL-C), apolipoprotein A1 (apo-AI), lipid-loading protein B (apo-B) and lipoprotein A (Lp (a)) were measured using equipment for chemical analysis (Dimension AR/AVL Clinical Chemistry System, Newark, NJ, USA) employed by the Clinical Laboratory Department of the First Affiliated Hospital of Xinjiang Medical University.
Clinical diagnosis
Hypertension was defined as blood pressure ≥ 140/90 mmHg at three different times on the same day or treatment with antihypertensive drugs. The diagnostic criteria for hyperlipidemia were defined according to the “Guidelines for the Prevention and Treatment of Dyslipidemia in Chinese Adults” [22]. The diagnostic criteria for diabetes was a clear history of diabetes, the use of hypoglycemic agents, fasting blood glucose ≥7.1 mmol/L, or two-hour postload glucose ≥11.1 mmol/L.
Coronary angiography, interventional therapy, and postoperative reports were performed by experienced coronary intervention specialists. Patients with CAD who underwent PCI received a loading dose of aspirin and clopidogrel preoperatively, and intravenous heparin anticoagulation was routinely used at the start of PCI.
Endpoints
The primary endpoint of the study was long-term mortality, including all-cause mortality (ACM) and cardiac mortality (death due to coronary heart disease, cardiogenic shock, or sudden death). Secondary endpoints were major adverse cardiac events (MACEs), which were defined as a combination of cardiac death, recurrent myocardial infarction, and target vessel reconstruction, and major adverse cardiac and cerebrovascular events (MACCEs), which were defined as MACE plus stroke, as described previously [23].
Follow-up
Specially trained professional staff performed the follow-up. All patients were followed via outpatient, inpatient, and telephone follow-up and with questionnaire surveys. The longest follow-up time was 10 years.
Statistical analysis
All analyses were performed using SPSS 22.0 for Windows statistical software (SPSS Inc., Chicago, IL, USA). For the subsequent analyses, we divided patients into three groups according to WAR value. Continuous variables are expressed as the means ± standard deviation or medians (25 to 75%), and categorical variables are expressed as a percentage. One-way ANOVA was used to evaluate differences between normally distributed numerical variables, and nonnormally distributed numerical variables were analyzed using the Mann-Whitney U test. The chi-squared test was used to compare categorical variables, and the cumulative incidence of long-term prognosis was analyzed by using Kaplan-Meier analysis. The log-rank test was used to compare groups. To establish the COX model, a univariate model analysis was performed for all predictors, and a significant (P < 0.05) variable in the univariate analysis was included in the multivariate Cox model. P < 0.05 was considered statistically significant.
Results
Baseline data and procedural characteristics
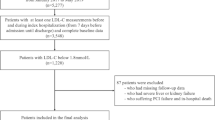
As shown in Fig. 1, 6050 patients with CAD who underwent PCI were included in the study. Of these, 372 patients were excluded because of no available baseline white blood cell counts and ApoA1 data, malignancies, and other diseases. Finally, 5678 patients were enrolled in the present study and divided into 3 groups according to WAR: lower group - WAR< 5.25 (n = 1889); median group - 5.25 ≤ WAR< 7.15 (n = 1892); and higher group - WAR≥7.15 (n = 1897). There were significant differences between groups in gender, smoking, alcohol consumption, age, total cholesterol, high-density lipoprotein-C, low-density lipoprotein-C, diastolic blood pressure, creatinine, and uric acid (all Ps < 0.05). However, clopidogrel and aspirin treatment, the incidence of diabetes, hypertension, systolic blood pressure, triglycerides, blood urea nitrogen and the procedural characteristics between groups were not significantly different (all Ps ≥ 0.05) (Table 1).

The flow chart of participant inclusion. A total of 6050 CAD patients after PCI were evaluated initially, and 5678 patients were included the present study
Clinical outcomes
As shown in Table 2 and Fig. 2, 293 patients developed all-cause mortality (ACM), including 85 (4.5%) patients in the lower group, 90 (4.8%) patients in the median group, and 118 (6.2%) patients in the higher group. The incidence of ACM increased gradually with the increase in WAR value, and the ACM incidence of the higher group was significantly increased than the lower group (HR = 1.484, 95%CI: 1.123–1.962, P = 0.007). We also found that the incidence of MACE (HR = 1.267, 95%CI:1.059–1.516, P = 0.010) or MACCEs (HR = 1.261, 95%CI: 1.062–1.499, P = 0.008) in the higher group was significantly greater compared to the lower group. These differences remained significant after multivariable COX regression analysis (ACM [HR = 1.626, 95%CI: 1.214–2.179, P = 0.001], MACCE [HR = 1.212, 95%CI: 1.011–1.454, P = 0.038], MACE [HR = 1.238, 95%CI: 1.025–1.495, P = 0.027). However, the incidence of CM was not significantly different between groups in univariate analysis (HR = 1.347, 95%CI: 0.989–1.835, P = 0.059) but showed significant differences in multivariable analysis (HR = 1.455, 95%CI: 1.051–2.014, P = 0.024). The neutrophil-to-lymphocyte ratio (NLR) and monocyte-to-HDL-C ratio (MHR) are independent predictors for outcomes. Therefore, we included these two variables in the multivariable Cox regression analysis. As shown in Tables S1, S2, S3 and S4, WAR remained a strong independent predictor for ACM, CM, MACCEs and MACEs.

Cumulative Kaplan-Meier estimates of the time to the first adjudicated occurrence of primary endpoints (ACM and CM) and secondary endpoints (MACCEs and MACEs). Left: Univariate analysis; Right: Multivariate. Upper: Primary endpoints; Lower: Secondary endpoints
As shown in Table 3, analyses with WAR as a continuous variable showed that every increase of 1 resulted in 3.4, 3.2, 2.0 and 2.2% increased risks of ACM, CM, MACCEs and MACEs at 10-year follow-up, respectively.
As shown in Fig. 3, the receiver operating characteristic (ROC) curve showed that the area under the curve (AUC) of WAR was the largest (AUC = 0.622) compared to WBC and ApoA1, which suggests that WAR is a stronger predictor for adverse outcomes in CAD patients who underwent PCI than WBC or ApoA1 alone. The ROC curve revealed 4.636 as the optimal cut-off value for WAR. Patients with a WAR ≥4.635 had 92.3, 81.3, 58.1 and 58.2% increased risks of ACM, CM, MACCEs and MACEs, respectively, compared to patients with WAR< 4.635 (Table 3).

Comparison of areas under the curves between WBC, ApoA1, and WAR
Discussion
The present study suggests that high WAR is significantly associated with long-term prognosis in patients with CAD who underwent PCI. The inclusion of WAR in clinical predictive models may significantly improve the power of prediction in CAD patients after PCI.
Recent studies demonstrated that elevated WBC counts were associated with an increased risk of CAD [22]. Leukocytes are associated with the destruction of arterial plaque stability, and an increased WBC count is an independent risk factor for CAD [24]. A recent study reported that infusion of apoA-1 reduced the neointimal area in the stent in a unique stent-implanted mouse model [20, 25]. Leukocytes are associated with neointimal hyperplasia (NIH) because these cells release inflammatory proteins and growth factors that stimulate smooth muscle cell proliferation [26]. These studies indicate that apoA-1 inhibits smooth muscle cell proliferation, inflammation, and leukocyte recruitment. Therefore, joint analyses of leukocytes and ApoA-1 provide more useful information for the predicting of cardiovascular events in patients with CAD.
The protective effect of ApoA1 on the formation of atherosclerotic lesions was extensively studied in animal models and humans [27, 28]. Yvan-Charvet et al. found that ApoA1 inhibited the degree of leukocytosis to a certain extent, which inhibited the progression of atherosclerosis [29]. The combination of leukocyte subtypes or the combination of leukocyte subtypes with other indicators may be used as a predictor of prognosis in patients with CAD [30]. For example, the neutrophil-to-lymphocyte ratio (NLR) is an independent predictor of long-term cardiovascular outcome after elective PCI [30]. Arisoy A et al. also found that the ratio of monocytes-to-high-density lipoprotein (MHR) was an independent predictor of increased thrombus burden after PCI in patients with STEMI [31]. These studies and findings provide strong evidence to support our current research. Furthermore, previous studies suggested that ApoA1 was associated with cardiovascular events in rheumatoid arthritis patients [32] and CAD patients who underwent PCI [33, 34]. These studies were in line with our result.
Numerous biomarkers and scoring systems are used for prognostic evaluations of patients with CAD. However, some systems are relatively expensive or difficult to apply in clinical practice. The present study is the first to demonstrate the association of elevated WAR with an increased risk of adverse outcomes in CAD patients.
The present study has several limitations. First, as a single-center observational study, unknown confounding factors may have affected the outcome. Second, this study only performed assessments of WAR, and it did not assess the effect of WAR changes. Third, there were 102 patients were loss of follow-up in the study, which might impact on the reality of the result. Forth, we did not compare WAR and well known inflammatory markers in CAD. Finally, the mechanism of action between Apo-A1 and WBC requires further study.
Conclusion
The present study demonstrated that WAR is independently associated with long-term mortality and may be used as an independent predictor of long-term outcomes in patients with CAD after PCI.
Availability of data and materials
Due to confidentiality policies, data will not be shared.
Abbreviations
- ACM:
-
All-cause mortality
- CAD:
-
Coronary artery disease
- CM:
-
Cardiac mortality
- MACCEs:
-
Major adverse cardiovascular and cerebrovascular events
- MACE:
-
Major adverse cardiovascular events
- PCI:
-
Percutaneous coronary intervention
- WAR:
-
White blood cell count-to-apolipoprotein A1 ratio
- WBC:
-
White blood cell
References
Wang D. Mechanisms of disease: inflammation, atherosclerosis, and coronary artery disease. Nature. 2005;306:5.
Tuttolomondo A, Di Raimondo D, Pecoraro R, Arnao V, Pinto A, Licata G. Atherosclerosis as an inflammatory disease. Curr Pharm Des. 2012;18:4266–88.
Anogeianaki A, Angelucci D, Cianchetti E, D'Alessandro M, Maccauro G, Saggini A, Salini V, Caraffa A, Tete S, Conti F, Tripodi D, Shaik-Dasthagirisaheb YB. Atherosclerosis: a classic inflammatory disease. Int J Immunopathol Pharmacol. 2011;24:817–25.
Vaccarezza M, Balla C, Rizzo P. Atherosclerosis as an inflammatory disease: doubts? No more. Int J Cardiol Heart Vasc. 2018;19:1–2.
Schlant RC, Forman S, Stamler J, Canner PL. Circulation. The natural history of coronary heart disease: prognostic factors after recovery from myocardial infarction in 2789 men. The 5-year findings of the coronary drug project. Circulation. 1982;66:401–14.
Lao D, Yeghiazarians Y. Pre-PCI white blood cell count: should we care? J Invasive Cardiol. 2009;21:207–8.
Danesh Sani SH, Eshraghi A, Shahri B, Vejdanparast M. No-reflow phenomenon in patients with ST-elevation acute myocardial infarction, treated with primary percutaneous coronary intervention: a study of predictive factors. J Cardiothorac Med. 2014;2:221–6.
Matić DM, Ašanin MR, SDj S, Mrdović IB, Marinković JM, Kočev NI, Antonijević NM, Marjanović MM, Nešić ZI, Prostran MS, Stanković GR. Incidence, predictors and prognostic implications of bleeding complicating primary percutaneous coronary intervention. Vojnosanit Pregl. 2015;72:589–95.
Abdi S, Rafizadeh O, Peighambari M, Basiri H, Bakhshandeh H. Evaluation of the clinical and procedural predictive factors of no-reflow phenomenon following primary percutaneous coronary intervention. Res Cardiovasc Med. 2015;4:e25414.
Gordon DJ, Probstfield JL, Garrison RJ, Neaton JD, Castelli WP, Knoke JD, Jacobs DR Jr, Bangdiwala S, Tyroler HA. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation. 1989;79(1):8–15.
Miyazaki A, Sakuma S, Morikawa W, Takiue T, Miake F, Terano T, Sakai M, Hakamata H, Sakamoto Y, Natio M, et al. Author information intravenous injection of rabbit apolipoprotein A-I inhibits the progression of atherosclerosis in cholesterol-fed rabbits. Arterioscler Thromb Vasc Biol. 1995;15:1882–8.
Tangirala RK, Tsukamoto K, Chun SH, Usher D, Pure E, Rader DJ. Regression of atherosclerosis induced by liver-directed gene transfer of apolipoprotein A-I in mice. Circulation. 1999;100:1816–22.
Shah PK, Yano J, Reyes O, Chyu KY, Kaul S, Bisgaier CL, Drake S, Cercek B. High-dose recombinant apolipoprotein A-I (Milano) mobilizes tissue cholesterol and rapidly reduces plaque lipid and macrophage content in apolipoprotein e-deficient mice. Potential implications for acute plaque stabilization. Circulation. 2001;103:3047–50.
Rong JX, Li J, Reis ED, Choudhury RP, Dansky HM, Elmalem VI, Fallon JT, Breslow JL, Fisher EA. Elevating high-density lipoprotein cholesterol in apolipoprotein E-deficient mice remodels advanced atherosclerotic lesions by decreasing macrophage and increasing smooth muscle cell content. Circulation. 2001;104:2447–52.
Feig JE, Rong JX, Shamir R, Sanson M, Vengrenyuk Y, Liu J, Rayner K, Moore K, Garabedian M, Fisher EA. HDL promotes rapid atherosclerosis regression in mice and alters inflammatory properties of plaque monocyte-derived cells. Proc Natl Acad Sci U S A. 2011;108:7166–71.
Shah PK, Amin J. Low high density lipoproteinlevel is associated with increased restenosis rate after coronary angioplasty. Circulation. 1992;85:1279–85.
Ghazzal ZB, Dhawan SS, Sheikh A, Douglas JS, Veledar E, Mavromatis K, Pohlel FK, Vaccarino V. Usefulness of serum high-density lipoprotein cholesterol level as an independent predictor of one-year mortality after percutaneous coronary interventions. Am J Cardiol. 2009;103:902–6.
De Geest B, Zhao Z, Collen D, Holvoet P. Effects of adenovirus-mediated human apo A-I gene transfer on neointima formation after endothelial denudation in apo E-deficient mice. Circulation. 1997;96:4349–56.
Feng Y, Gordts SC, Chen F, Hu Y, Van Craeyveld E, Jacobs F, Carlier V, Feng Y, Zhang Z, Xu Q, Ni Y, De Geest B. Topical HDL administration reduces vein graft atherosclerosis in apo E deficient mice. Atherosclerosis. 2011;214:271–8.
Vanags LZ, Tan JTM, Galougahi KK, Schaefer A, Wise SG, Murphy A, Ali ZA, Bursill CA. Apolipoprotein A-I reduces in-stent restenosis and platelet activation and alters Neointimal cellular phenotype. JACC Basic Transl Sci. 2018;3:200–9.
Tani S, Nagao K, Hirayama A. Association of systemic inflammation with the serum apolipoprotein A-1 level: a cross-sectional pilot study. J Cardiol. 2016;68:168–77.
Twig G, Afek A, Shamiss A, Derazne E, Tzur D, Gordon B, Tirosh A. White blood cell count and the risk for coronary artery disease in young adults. PLoS One. 2012;7:e47183.
Zheng YY, Wu TT, Chen Y, Hou XG, Yang Y, Ma X, Ma YT, Zhang JY, Xie X. Gamma-Glutamyl Transferase-to-platelet ratio as a novel predictor of long-term adverse outcomes in patients after undergoing percutaneous coronary intervention: a retrospective cohort study. Thromb Haemost. 2019;119(6):1021–30.
Takeda Y, Suzuki S, Fukutomi T, Kondo H, Sugiura M, Suzumura H, Murasaki G, Okutani H, Itoh M. Elevated white blood cell count as a risk factor of coronary artery disease: inconsistency between forms of the disease. Jpn Heart J. 2003;44:201–11.
Ali ZA, Alp NJ, Lupton H, Arnold N, Bannister T, Hu Y, Mussa S, Wheatcroft M, Greaves DR, Gunn J, Channon KM. Increased in-stent stenosis in ApoE knockout mice: insights from a novel mouse model of balloon angioplasty and stenting. Arterioscler Thromb Vasc Biol. 2007;27:833–40.
Welt FG, Tso C, Edelman ER, Kjelsberg MA, Paolini JF, Seifert P, Rogers C. Leukocyte recruitment and expression of chemokines following different forms of vascular injury. Vasc Med. 2003;8:1–7.
Nissen SE, Tsunoda T, Tuzcu EM, Schoenhagen P, Cooper CJ, Yasin M, Eaton GM, Lauer MA, Sheldon WS, Grines CL, Halpern S, Crowe T, Blankenship JC, Kerensky R. Effect of recombinant ApoA-I Milano on coronary atherosclerosis in patients with acute coronary syndromes: a randomized controlled trial. JAMA. 2003;290:2292–300.
Moore RE, Navab M, Millar JS, Zimetti F, Hama S, Rothblat GH, Rader DJ. Increased atherosclerosis in mice lacking apolipoprotein A-I attributable to both impaired reverse cholesterol transport and increased inflammation. Circ Res. 2005;97(8):763–71.
Yvan-Charvet L, Pagler T, Gautier EL, Avagyan S, Siry RL, Han S, Welch CL, Wang N, Randolph GJ, Snoeck HW, Tall AR. ATP-binding cassette transporters and HDL suppress hematopoietic stem cell proliferation. Science. 2010;328(5986):1689–93.
Wada H, Dohi T, Miyauchi K, Shitara J, Endo H, Doi S, Konishi H, Naito R, Tsuboi S, Ogita M, Kasai T, Hassan A, Okazaki S, Isoda K, Suwa S, Daida H. Pre-procedural neutrophil-to-lymphocyte ratio and long-term cardiac outcomes after percutaneous coronary intervention for stable coronary artery disease. Atherosclerosis. 2017;265:35–40.
Arısoy A, Altunkaş F, Karaman K, Karayakalı M, Çelik A, Ceyhan K, Zorlu Ç. Association of the Monocyte to HDL cholesterol ratio with Thrombus burden in patients with ST-segment elevation myocardial infarction. Clin Appl Thromb Hemost. 2017;23:992–7.
Zegarra-Mondragón S, López-González R, Martín-Martínez MA, García-Gómez C, Sánchez-Alonso F, González-Juanatey C, Manrique Arija S, Bonilla Hernán G, Martínez Pardo S, Ruibal Escribano A, Pagán García E, Delgado Frías E, Rivera Redondo J, Delgado Sánchez M, Rodriguez Cambrón AB, Moreno Ramos MJ, Rodríguez Montero SA, Navío Marco MT, Morcillo Valle M, García González J, Bachiller Corral J, Llorca J, Castañeda S, González-Gay MÁ; CARMA Project Collaborative Group. Association of apolipoprotein B/apolipoprotein A1 ratio and cardiovascular events in rheumatoid arthritis: results of the CARMA study. Clin Exp Rheumatol; 2019. [Epub ahead of print] PMID: 31694752.
Chen BD, Chen XC, Yang YN, Gao XM, Ma X, Huang Y, Li XM, Gai MT, Liu F, Pan S, Ma YT. Apolipoprotein A1 is associated with SYNTAX score in patients with a non-ST segment elevation myocardial infarction. Lipids Health Dis. 2019;18(1):159. https://doi.org/10.1186/s12944-019-1101-9.
Tian M, Li R, Shan Z, Wang DW, Jiang J, Cui G. Comparison of Apolipoprotein B/A1 ratio, Framingham risk score and TC/HDL-c for predicting clinical outcomes in patients undergoing percutaneous coronary intervention. Lipids Health Dis. 2019;18(1):202. https://doi.org/10.1186/s12944-019-1144-y.
Acknowledgments
The authors are grateful to the Department of Cardiology at the First Affiliated Hospital of Xinjiang Medical University for their help and expertise in conducting this study.
Funding
This research was funded by the National Natural Science Foundation of China (U1603381, 81760043 and 81560070).
Author information
Authors and Affiliations
Contributions
YP, TTW and JZ made substantial contributions to the study conception and design and to the drafting and critical revision of the manuscript for important intellectual content. XGH, YY, XM, and YTM made substantial contributions to the study conception and design and to the critical revision of the manuscript for important intellectual content. XX and YYZ made substantial contributions to the study conception and design and to the drafting and critical revision of the manuscript for important intellectual content, including study supervision. The authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The ethics committee or review committee of the First Affiliated Hospital of Xinjiang Medical University approved the research protocol. Because the study was a retrospective cohort study based on real-world situations, there was no need to obtain informed consent from patients.
Consent for publication
All authors agree to the publication of this work.
Competing interests
No potential conflicts of interest relevant to this article were reported by any of the authors. None of the funding sources played a role in the design, collection, analysis or interpretation of the data or in the decision to submit the manuscript for publication. The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Table S1.
Multivariable analysis for CM. Table S2. Multivariable analysis for ACM. Table S3. Multivariable analysis for MACCE. Table S4. Multivariable analysis for MACE.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Pan, Y., Zhang, J., Wu, TT. et al. Baseline white blood cell count-to-apolipoprotein A1 ratio as a novel predictor of long-term adverse outcomes in patients who underwent percutaneous coronary intervention: a retrospective cohort study. Lipids Health Dis 19, 43 (2020). https://doi.org/10.1186/s12944-020-01206-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-020-01206-w