
Abstract
Background
Dyslipidemia, an increased level of total cholesterol (TC), triglycerides (TG), low-density-lipoprotein cholesterol (LDL-C) and decreased level of high-density-lipoprotein cholesterol (HDL-C), is one of the most important risk factors for cardiovascular disease. We examined the six-year trend of dyslipidemia in Newfoundland and Labrador (NL), a Canadian province with a historically high prevalence of dyslipidemia.
Methods
A serial cross-sectional study on all of the laboratory lipid tests available from 2009 to 2014 was performed. Dyslipidemia for every lipid component was defined using the Canadian Guidelines for the Diagnosis and Treatment of Dyslipidemia. The annual dyslipidemia rates for each component of serum lipid was examined. A fixed and random effect model was applied to adjust for confounding variables (sex and age) and random effects (residual variation in dyslipidemia over the years and redundancies caused by individuals being tested multiple times during the study period).
Results
Between 2009 and 2014, a total of 875,208 records (mean age: 56.9 ± 14.1, 47.6% males) containing a lipid profile were identified. The prevalence of HDL-C and LDL-C dyslipidemia significantly decreased during this period (HDL-C: 35.8% in 2009 [95% CI 35.5-36.1], to 29.0% in 2014 [95% CI: 28.8-29.2], P = 0.03, and LDL-C: 35.2% in 2009 [95% CI: 34.9-35.4] to 32.1% in 2014 [95% CI: 31.9-32.3], P = 0.02). A stratification by sex, revealed no significant trend for any lipid element in females; however, in men, the previously observed trends were intensified and a new decreasing trend in dyslipidemia of TC was appeared (TC: 34.1% [95% CI 33.7-34.5] to 32.3% [95%CI: 32.0-32.6], p < 0.02, HDL-C: 33.8% (95%CI: 33.3-34.2) to 24.0% (95% CI: 23.7-24.3)], P < 0.01, LDL-C: 32.9% (95%CI:32.5-33.3) to 28.6 (95%CI: 28.3-28.9), P < 0.001). Adjustment for confounding factors and removing the residual noise by modeling the random effects did not change the significance.
Conclusion
This study demonstrates a significant downward trend in the prevalence of LDL-C, HDL-C, and TC dyslipidemia, exclusively in men. These trends could be the result of males being the primary target for cardiovascular risk management.
Similar content being viewed by others


Background
Cardiovascular disease (CVD), remains to be the first cause of death globally, with 17.7 million deaths each year [1]. In Canada, over 1.3 million people have a diagnosis of heart disease [2], and CVD is the leading cause of death (one-third of the total deaths) [3], imposing the highest economic burden of disease after musculoskeletal conditions [2]. In the past decades, significant improvements have been reported in the rates of CVD and its associated risk factors in the developed world. Over the past 50 years, there has been a 70% decline in the incidence of CVD in Canada [2]. Compared to the other Canadian provinces, however, Newfoundland and Labrador (NL) has the highest rates of CVD morbidity and mortality in adults [4]. In 2007, Statistics Canada reported that NL had the highest age-standardized mortality rate for major CVD events (218.5 per 100,000 population) among all Canadian provinces (national average mortality rate: 151.9/100,000) [5]. This rate is comparable to those of low- or middle-income nations which tend to have higher CVD-related death rates compared to the developed world [6, 7], and do not show a declining trend in CVD incidence [8].
The declining global trends in CVD incidence has been mainly attributed to decreasing rates of preventable CVD risk factors such as tobacco use [9], uncontrolled hypertension [10], and abnormal lipid levels [11]. Dyslipidemia, defined as abnormally elevated levels of total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG), as well as decreased levels of high-density lipoprotein cholesterol (HDL-C), is one of the strongest and most modifiable risk factors for CVD [12]. Like other CVD risk factors, there has been an improvement in the abnormal cholesterol levels among Canadians in the past decade, and this trend is projected to continue over the next few years [11]. However, it is not known whether the declining trend in the prevalence of dyslipidemia has reached the NL population. Our previous study demonstrated that the prevalence of dyslipidemia, as represented by abnormal levels of total cholesterol (40 vs. 37%), LDL-C (29 vs. 25%), triglyceride (29 vs. 26%) and HDL-C (38 vs. 27%), is significantly higher in NL compared to the rest of Canada [13]. Although the cultural and genetic isolation of the NL population [14] might partially explain the differences in the lipid profiles, our study on high-cardiac risk patients has shown that primary care management, particularly medication therapy, is the most contributing factor to suboptimal lipid levels in Canada, and particularly, in NL [15]. Therefore, any change in the pattern of dyslipidemia could well reflect the quality of healthcare in the province, and thus, the higher rates of CVD and dyslipidemia prevalence in NL necessitates the investigation of the trend of the change in dyslipidemia.
The availability of Laboratory Information System (LIS) in NL, which enables access to all of the laboratory test results conducted in the province, provides an excellent opportunity to investigate the rates of dyslipidemia and its patterns over the past years. Discovery of this trend in NL is essential since it can be helpful for the estimation of future prevalence of dyslipidemia and its consequential burden on the health care system. Also, these data are necessary for evaluation and monitoring of the effectiveness of population- and community-wide interventions in reducing the prevalence of dyslipidemia and its adverse consequences in NL, and accordingly, in Canada. The present study examines the trend and pattern of dyslipidemia among the adult population living in NL over a six-year period between 2009 and 2014.
Methods
Source of data
Individuals with a registered permanent address in NL are provided with a lifetime medical care plan number. For each laboratory service, the patient’s identification (ID), date of service, and laboratory test results are entered into the LIS. The system is administered through four health region authorities in the province (Eastern, Central, Western, and Labrador-Grenfell). The study extracted all available records included in the LIS between January 2009 and December 2014. Every record contained individual de-identified ID, age, sex, date of testing, and lipid test results. Only records for individuals who were 20 years and older at the time of lipid testing, were used in this study.
Identification of trends of change in dyslipidemia
We defined dyslipidemia based on lipid levels, according to the Canadian Guidelines for the Diagnosis and Treatment of Dyslipidemia (Table 1), in effect during the time of the study [16, 17]. The prevalence of dyslipidemia in each year was calculated as the ratio of records with abnormal levels of lipid to the total number of records available in that year. Descriptive statistics, including mean and 95% confidence intervals (CI), were used to describe and visualize the changes in the prevalence of dyslipidemia over the 6-year period. A non-parametric trend test was performed to examine the existence of a changing trend in dyslipidemia during this time.
Adjustment for confounding factors and control for repeated individual tests and random yearly variations
Assessment of the variability in the lipid profiles as reported by the four different regional health authorities was determined by measuring an intra-class correlation which did not reveal a significant clustering by health region (not shown). Therefore this variable was not used in this analysis. A multivariable logistic mixed effect model was utilized to adjust for the confounding variables including age and sex, as well as to account for variations caused by the same individuals repeating the tests over the 6-year period or the normal yearly changes. In this model, dyslipidemia status was considered as the response variable, the year was considered a categorical predictor, and age and sex were incorporated as confounding factors. The first year (2009) was considered as the base, to which all of the upcoming years were compared. Given an individual could be tested for lipid profile multiple times across the 6-year period, we incorporated the individual ID as a random effect in the model to account for this redundancy. As well, we incorporated the year variable as the second random effect to reduce the residual variation that typically occurs on a yearly basis in dyslipidemia rates. The analysis was conducted using the lme4 package [18].
All of the statistical analyses were performed using R.3.3.0. P-values less than 0.05 were considered significant.
Results
Characteristics of the study population
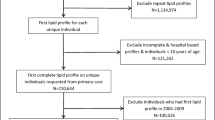
After quality assessment and removal of missing information, a total of 875,208 records with lipid tests were identified in LIS, representing the total number of tests performed in the province between 2009 and 2014. A considerable gradual increase in the number of tests was noted from the first year (2009, ~ 115,000) to the last year of the study (2014, ~ 184,000). The population was almost equally composed of males and females with slightly more records identified for women (52 - 53% females). The mean age ranged from 56 to 58 during the 6-year period. Table 2 represents the characteristics of the study population as stratified by each year included in our study.
Changes in the pattern of dyslipidemia between 2009 and 2014
Examination of the rates of dyslipidemia over the 6-year period revealed a declining trend for HDL-C (35.8% [95% confidence interval: 28.8 - 29.2] to 29.0% [95% confidence interval: 28.8 - 29.2], p = 0.03) and LDL-C (35.2% [95% confidence interval: 34.9 - 35.4] to 32.1% [95% confidence interval: 31.9 - 32.3], p = 0.02). Other lipid components fluctuated during the same period without overall significant changes. Total cholesterol dyslipidemia, for instance, showed a decreasing trend from 39% to 37% in 2013, but its rates increased to above 38% in 2014 (Fig. 1, Table 2). Re-examination of the trends following a split by sex, however, revealed that the declining pattern of change in HDL-C and LDL-C dyslipidemia is only significant in males. The split also resulted in the appearance of a significant decreasing trend in total cholesterol dyslipidemia in males (34.1% [95% confidence interval: 33.7 - 34.5] to 32.3% [95% confidence interval: 32.0 - 32.6], p = 0.02), but not in females (Table 2).

Rates of dyslipidemia by lipid components over six years: TC: Total cholesterol; HDL-C: High-density lipoprotein cholesterol, LDL-C: Low-density lipoprotein cholesterol, TG: Triglycerides
Trend of dyslipidemia after adjustment for confounding factors and random effects
Using a multivariable logistic mixed effect model, we examined the yearly pattern of change as adjusted for confounding factors (age and sex) and random effects (individuals repeating the test in the 6-year period, and regular annual variations in dyslipidemia). The analysis confirmed the previously observed declining rates of dyslipidemia over the 6-year period with the most prominent effect for HDL-C and LDL-C dyslipidemia. According to this analysis, the odds of finding an HDL-C or LDL-C dyslipidemia in the laboratory test reports in the last year of the study was significantly lower than those in the first year (ORHDL-C: 0.78, 95% confidence interval: 0.77 - 0.79, ORLDL-C: 0.87, 95% confidence interval: 0.85 - 0.88). Although a declining trend was observed for other lipid components, these findings were not as prominent as those found for LDL-C and HDL-C, with odds ratios ranging between 0.95 to 0.99. The most determinant variable of dyslipidemia in the population, however, was sex where males were significantly less likely to have dyslipidemia of HDL-C, LDL-C, and total cholesterol (OR: 0.60 – 0.78), but more likely to have a dyslipidemia of triglyceride (OR: 1.27, 95% confidence interval: 1.26 - 1.28). No effect was observed for age. The result of this analysis is presented in Table 3.
Discussion
The current study described the trend of dyslipidemia over a six-year period during 2009 to 2014 in NL using provincial medical laboratory information. The analyses identified a significant downward trend in the prevalence of dyslipidemia of LDL-C and HDL-C during this period. Further evaluations indicated that this declining pattern is mainly represented in males, whereas females do not show a significant change in the trend of dyslipidemia. Being male was also associated with a lower risk of having any form of dyslipidemia except for triglyceride.
Dyslipidemia is a highly manageable risk factor for CVD. The association between hyperlipidemia and the incidence, morbidity, and mortality of CVD has been reported in numerous studies [19, 20]. Every 1.0 mmol/L (38.6 mg/dl) reduction in LDL-C is found to be associated with a ~ 23% relative risk reduction in major vascular events over a five-year period [21]. Similarly, every 1.0 mg/dl increase in HDL-C has resulted in a 2-3% reduction in the occurrence of coronary heart disease [22]. Guidelines for the management of lipid levels as a means of CVD risk reduction have been in effect for decades, and these practices have resulted in a significant decrease in the rates of dyslipidemia, and subsequently CVD, in the developed world. Examination of a 30-year trend (1976-2006) in serum lipids among adults in the United States has shown decreases in age-adjusted mean TC (210 to 200 mg/dl) and LDL-C (134 to 119 mg/dl) as well as a significant increase in mean HDL-C (50 to 53 mg/dl) [23]. Similar patterns of change have been observed in Europe, as reported in a 10-year period by the Framingham Heart Study [24], and the northern Sweden MONICA study [25]. In Canada, projected rates of high cholesterol, based on the observed rates from the Canadian Health Measure Survey, indicates a gradual decrease in hypercholesterolemia between 2001 and 2021 [11].
In NL, however, no data is available on the time trend of change in dyslipidemia, besides the few recent reports of a higher rate of hypercholesterolemia compared to the rest of Canada. Our study is the first to examine such a trend over a six-year period in NL. Approximately ten years ago, a survey of waist circumference and body mass index in NL recommended that young NL adults are at an elevated risk of cardiovascular events due to the distribution of body fat [26]. Since then, multiple evaluations by our group and others recommended that the NL population may also suffer from a higher rate of dyslipidemia and other CVD risk factors [13]. These reports could have led to an increased awareness among the clinicians in NL. The findings in the present study recommend that NL is at the beginning of a movement toward improving cardiometabolic profiles. Our results support a declining trend in the rates of dyslipidemia of HDL-C, LDL-C, and TC. However, the level of change is not as significant as those found elsewhere, and any degree of improvement is restricted to men. These may be an indication of a recent movement towards the improvement of primary care management of dyslipidemia in the province.
An interesting finding in this study was that any declining trend in the rates of abnormal lipid profiles is restricted to men. Also, being male was significantly associated with a lower risk of having any dyslipidemia, except for TG. These might suggest that men have been targeted more intensively for CVD risk management. An alternative explanation might be related to the distribution of the age of our population. At the mean age of > 55, women are influenced by the physiological changes of menopause and are likely to show a higher rate of dyslipidemia [27]. It is possible that due to these physiological changes, women are not as responsive to CVD risk interventions as men [28, 29]. These hypotheses, however, will need to be further investigated.
Our study is limited by a few factors which need to be taken into consideration. The findings are built on the clinical laboratory tests conducted in the province and thus may not show a crude prevalence of dyslipidemia in NL. However, the results represent any individual who has ever performed a lipid test in the province during the six-year period, and thus, they can be used as a reliable indicator of population health as related to CVD and dyslipidemia. The other limitation of this study is the lack of information on the confounding factors that might influence dyslipidemia (e.g., body mass index, diabetes, menopause status and smoking). Also, the information related to lipid modifying agent consumption was not available. Lifestyle-related factors related to hypercholesterolemia such as nutritional behaviors, physical activity and awareness towards primary prevention were not included in this study since we did not have access to datasets where these variables were included.
Conclusion
The findings of this study reveal that NL has started to follow the declining trend in the rates of dyslipidemia. This is mainly represented as a significant downward trend in the rates of LDL-C, HDL-C, and TC dyslipidemia in men. These trends could be the result of males being the primary target for cardiovascular risk management guidelines; however, further research is required to verify this hypothesis. The province of Newfoundland and Labrador could see a reduction in cardiovascular disease incidence along with their associated mortality rates following an improvement in lipid profiles within the next few years. Our study’s findings indicate the urgency for further investigation into this matter which can be considered essential for the proper surveillance of chronic disease outcomes in the province.
Abbreviations
- CVD:
-
Cardiovascular disease
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- LIS:
-
Laboratory information system
- NL:
-
Newfoundland and Labrador
- OR:
-
Odds ratio
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
References
World Health Organization. Cardiovascular diseases (CVDs). In: Fact sheets. World Health Organization – Media center. 2017. http://www.who.int/mediacentre/factsheets/fs317/en/. Accessed 25 Apr 2018.
Public Health Agency of Canada. Many Canadians have CVD. In: Tracking Heart Disease and Stroke in Canada. 2009. http://www.phac-aspc.gc.ca/publicat/2009/cvd-avc/pdf/cvd-avs-2009-eng.pdf. Accessed 25 Apr 2018.
Genest J, McPherson R, Frohlich J, Anderson T, Campbell N, Carpentier A, et al. 2009 Canadian cardiovascular society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult–2009 recommendations. Can J Cardiol. 2009;25(10):567–79.
Filate WA, Johansen HL, Kennedy CC, Tu JV. Regional variations in cardiovascular mortality in Canada. Can J Cardiol. 2003;19(11):1241–8.
Statistics Canada. Mortality, summary list of causes 2007. In: Mortality, summary list of causes. 2010. http://www.statcan.gc.ca/pub/84f0209x/84f0209x2007000-eng.pdf. Accessed 25 Apr 2018.
World Health Organization. The global burden of disease: 2004 update. In: the global burden of disease: 2004 update. 2008. http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf. Accessed 25 Apr 2018.
Nichols M, Townsend N, Scarborough P, Rayner M. Cardiovascular disease in Europe 2014: epidemiological update. Eur Heart J. 2014;35(42):2950–9.
Gadd M, Johansson SE, Sundquist J, Wändell P. The trend of cardiovascular disease in immigrants in Sweden. Eur J Epidemiol. 2005;20(9):755–60.
Reid JL, Hammond D, Rynard VL, Madill CL, Burkhalter R. Tobacco Use in Canada: Patterns and Trends, 2017 Edition. Waterloo, ON: Propel Centre for Population Health Impact, University of Waterloo. Available: https://uwaterloo.ca/tobacco-use-canada/sites/ca.tobacco-use-canada/files/uploads/files/2017_tobaccouseincanada_final_0.pdf. Accessed 25 Apr 2018.
McAlister FA, Wilkins K, Joffres M, Leenen FH, Fodor G, Gee M, Tremblay MS, Walker R, Johansen H, Campbell N. Changes in the rates of awareness, treatment and control of hypertension in Canada over the past two decades. CMAJ. 2011;183(9):1007–13.
Manuel DG, Tuna M, Hennessy D, Bennett C, Okhmatovskaia A, Finès P, Tanuseputro P, Tu JV, Flanagan W, Simulation Technology for Applied Research Team, Canadian Cardiovascular Outcome Research Team. Projections of preventable risks for cardiovascular disease in Canada to 2021: a microsimulation modelling approach. CMAJ open. 2014;2(2):E94.
Nelson RH. Hyperlipidemia as a risk factor for cardiovascular disease. Prim Care. 2013;40(1):195–211.
Asghari S, Aref-Eshghi E, Hurley O, Godwin M, Duke P, Williamson T, et al. Does the prevalence of dyslipidemias differ between Newfoundland and the rest of Canada? Findings from the electronic medical Records of the Canadian Primary Care Sentinel Surveillance Network. Front Cardiovasc Med. 2015;2
Rahman P, Jones A, Curtis J, Bartlett S, Peddle L, Fernandez BA, et al. The Newfoundland population: a unique resource for genetic investigation of complex diseases. Hum Mol Genet 15. 2003;12 Spec No 2:R167-72.
Aref-Eshghi E, Leung J, Godwin M, Duke P, Williamson T, Mahdavian M, Asghari S. Low density lipoprotein cholesterol control status among Canadians at risk for cardiovascular disease: findings from the Canadian primary care sentinel surveillance network database. Lipids Health Dis. 2015;14(1):60.
Oake J, Aref-Eshghi E, Godwin M, Collins K, Aubrey-Bassler K, Duke P, Mahdavian M, Asghari S. Using electronic medical record to identify patients with dyslipidemia in primary care settings: international classification of disease code matters from one region to a national database. Biomed Inform Insights. 2017;9:1178222616685880.
Aref-Eshghi E, Oake J, Godwin M, Aubrey-Bassler K, Duke P, Mahdavian M, Asghari S. Identification of Dyslipidemic patients attending primary care clinics using electronic medical record (EMR) data from the Canadian primary care sentinel surveillance network (CPCSSN) database. J Med Syst. 2017;41(3):45.
Bates D, Maechler M, Bolker B, Walker S. lme4: linear mixed-effects models using Eigen and S4. R package version. 2014;1(7):1–23.
Castelli WP. Cholesterol and lipids in the risk of coronary artery disease--the Framingham heart study. Can J Cardiol. 1988;4:5A–10A.
Cooney MT, Dudina A, De Bacquer D, Wilhelmsen L, Sans S, Menotti A, De Backer G, Jousilahti P, Keil U, Thomsen T, Whincup P. HDL cholesterol protects against cardiovascular disease in both genders, at all ages and at all levels of risk. Atherosclerosis. 2009;206(2):611–6.
Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366(9493):1267–78.
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Summary of the second report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel II). JAMA. 1993;269:3015–23.
Cohen JD, Cziraky MJ, Cai Q, Wallace A, Wasser T, Crouse JR, Jacobson TA. 30-year trends in serum lipids among United States adults: results from the National Health and nutrition examination surveys II, III, and 1999–2006. Am J Cardiol. 2010;106(7):969–75.
Ingelsson E, Massaro JM, Sutherland P, Jacques PF, Levy D, D’Agostino RB, Vasan RS, Robins SJ. Contemporary trends in dyslipidemia in the Framingham heart study. Arch Intern Med. 2009;169(3):279–86.
Eliasson M, Janlert U, JANSSON JH, Stegmayr B. Time trends in population cholesterol levels 1986–2004: influence of lipid-lowering drugs, obesity, smoking and educational level. The northern Sweden MONICA study. J Intern Med. 2006;260(6):551–9.
Kettle SM, Roebothan BV, West R. Prevalence of specific cardiovascular disease risk factors in young Newfoundland and Labrador adults living in urban and rural communities. Can J Rural Med. 2005;10(2):81–5.
Gold EB. The timing of the age at which natural menopause occurs. Obstet Gynecol Clin North Am. 2011;38(3):425.
Sultan N, Nawaz M, Sultan A, Fayaz M, Baseer A. Effect of menopause on serum HDL-cholesterol level. J Ayub Med Coll Abbottabad. 2002;15(3):24–6.
Kim CJ, Kim TH, Ryu WS, Ryoo UH. Influence of menopause on high density lipoprotein-cholesterol and lipids. J Korean Med Sci. 2000;15(4):380–6.
Funding
This study was supported by a project grant from the Newfoundland and Labrador Centre for Applied Health Research.
Availability of data and materials
Due to the HREA conditions and to protect the identity of the subjects, the data used in this study is not publically available.
Author information
Authors and Affiliations
Contributions
PP and EAE: data analysis and manuscript writing; HHM: data analysis; OH, SA, MG, PD, MM: interpretation of the results and revisions; SA: study design and supervision of the study team. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study has been approved by the Health Research Ethics Authority, Memorial University of Newfoundland, Canada. All of the data were anonymized prior to analysis.
Consent for publication
All of the authors have read and approved this manuscript for publication.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Pedram, P., Aref-Eshghi, E., Mariathas, H.H. et al. Six-year time-trend analysis of dyslipidemia among adults in Newfoundland and Labrador: findings from the laboratory information system between 2009 and 2014. Lipids Health Dis 17, 99 (2018). https://doi.org/10.1186/s12944-018-0752-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-018-0752-2