
Abstract
This study aimed to evaluate the accuracy of disk diffusion and Etest methods, compared to that of the broth dilution reference method for identifying beta-lactam susceptibilities of Penicillin-Resistant, Ampicillin-Susceptible Enterococcus faecalis (PRASEF) isolates. Fifty-nine PRASEF and 15 Penicillin-Susceptible, Ampicillin-Susceptible E. faecalis (PSASEF) clinical nonrepetitive isolates were evaluated. The effectiveness of five beta-lactams (ampicillin, amoxicillin, imipenem, penicillin, and piperacillin) was tested. All antimicrobial susceptibility tests were performed and interpreted according to the Clinical and Laboratory Standards Institute guidelines. Interpretative discrepancies, such as essential agreement, categorical agreement, and errors, were assessed. The acceptability was ≥ 90% for both categorical agreement and essential agreement. Etest proved to be an accurate method for testing beta-lactam susceptibilities of the emerging PRASEF isolates, disk diffusion presented poor performance, particularly for imipenem and piperacillin.
Similar content being viewed by others


Background
Although enterococci are widely distributed in the environment and are considered as normal intestinal microbes of humans and animals, during the past few decades, they have caused various infections in humans, primarily observed in hospitalized patients [1]. E. faecalis, an enterococci species, is most frequently isolated from clinical specimens [2]. These microorganisms are intrinsically resistant to several antimicrobial agents and have a great ability to acquire and express new resistance determinants. Notably, in recent years, enterococci have acquired high-level antibiotic resistance to aminoglycosides, glycopeptides, and beta-lactams [1, 3].
Enterococci usually present cross-susceptibility to β-lactamase-susceptible penicillin; however, the emergence of clinical penicillin-resistant, ampicillin-susceptible Enterococcus faecalis (PRASEF) isolates, exhibiting an unusual resistance phenotype, have been reported in various countries [4,5,6,7,8]. Moreover, although the current Clinical and Laboratory Standards Institute (CLSI) [9] and European Committee on Antimicrobial Susceptibility Testing (EUCAST) [10] guidelines state that the susceptibility to ampicillin may predict susceptibility to amoxicillin, piperacillin, and imipenem for E. faecalis, studies have demonstrated that this rule may not be applicable to the penicillin resistant isolates [3, 4, 6, 8].
Various methods are applied for the in vitro evaluation of enterococci susceptibility to beta-lactams; however, disk diffusion and Etest are routinely used in most clinical microbiology laboratories in the developing countries [11, 12]. Thus, this study aimed to assess the performance of Etest and disk diffusion methods to determine the susceptibilities of PRASEF isolates for beta-lactam antimicrobials in comparison with broth dilution using the reference method.
Methods
Bacterial isolates and species identification
In total, 59 PRASEF nonrepetitive isolates recovered from patients admitted at a Brazilian tertiary hospital during the period 2006–2014 were included in this study. A few isolates evaluated herein belonged to a previous publication [6, 13]. Moreover, 15 penicillin-susceptible, ampicillin-susceptible E. faecalis (PSASEF) isolates were evaluated for comparative testing. The species identification of isolates was based on the phenotypic tests [2] and was confirmed by PCR using specific primers [14]. No isolate produced beta-lactamase according to the results of the nitrocefin disk test (Becton Dickinson and Company).
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing methods (broth dilution, disk diffusion, and Etest) were run simultaneously, and the standardized inoculum was prepared from the same bacterial suspension. The direct colony suspension method was used for preparing inoculum from colonies grown within 18–24 h at 35 ± 2 °C. Five beta-lactams were tested (penicillin, ampicillin, amoxicillin, imipenem, and piperacillin). Broth dilution and disk diffusion were performed and interpreted according to CLSI guidelines [9]. Etest (bioMérieux, Sweden) was performed according to the manufacturer’s instructions.
The broth dilution method was carried out using cation-adjusted Mueller–Hinton broth (Difco, France) and antimicrobial solutions were prepared from powders of known potencies (Sigma-Aldrich, Denmark). The beta-lactam dilutions tested ranged from 0.5 to 256 µg/mL. E. faecalis ATTC 29212 was used as a susceptible control. The same strain was used as a control for Etest assays. A minimum inhibitory concentration (MIC) ≥ 16 µg/mL indicated resistance to all beta-lactams evaluated [9].
Beta-lactam disks (Oxoid, United Kingdom) and Mueller–Hinton agar (Difco, France) were used for disk diffusion testing. Staphylococcus aureus ATCC 25923 and Escherichia coli ATCC 25922 were included as susceptible controls. An inhibition zone diameter ≥ 15 mm indicated penicillin susceptibility and ≥ 17 mm indicated susceptibility to other beta-lactams [9].
Data interpretation and analysis
Disk diffusion and Etest results were compared with those obtained by the broth dilution method, which is considered the gold standard. Interpretative discrepancies such as essential agreement (EA; MIC ± 1 log2), categorical agreement (CA; same category result), very major error (VME; false susceptible), and major error (ME; false resistant) were assessed as described elsewhere [11]. The acceptability was ≥ 90% for both CA and EA.
Results and discussion
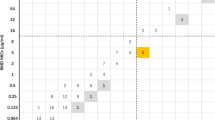
Table 1 summarizes the results of beta-lactam antimicrobial susceptibility testing of E. faecalis isolates and the interpretative discrepancies for each method, whereas Fig. 1 illustrates the relationship of beta-lactam MICs by the reference method and the zone diameters by disk diffusion for PRASEF and PSASEF isolates.

Scattergram of beta-lactam zone diameters of the disk diffusion and minimum inhibitory concentration (MIC) from the reference method of the penicillin-susceptible, ampicillin-susceptible E. faecalis (PSASEF; n = 15) and penicillin-resistant, ampicillin-susceptible E. faecalis (PRASEF; n = 59) isolates. Current CLSI breakpoints are represented as dotted lines. Numbers represent the number of isolates at each MIC/zone diameter pair
Among the 59 PRASEF isolates evaluated, 16 (27.1%) were resistant to imipenem and 58 (98.3%) to piperacillin, according to the results of the broth dilution reference method; however, no isolate was resistant to ampicillin or amoxicillin using the same reference method, indicating that ampicillin susceptibility should not be used to predict susceptibility of imipenem and piperacillin for E. faecalis with penicillin resistance phenotype.
As demonstrated in Table 1, the Etest revealed good accuracy (CA > 90%) for all beta-lactams, except for imipenem (CA of 85.1%), although no VME (false susceptibility) was observed for the latter drug. Notably, most imipenem false-resistant isolates (7 of 11) exhibited MIC values around the CLSI breakpoint. All beta-lactams presented good EA rates, except for piperacillin, which revealed a great variability in MIC values, particularly in the PRASEF isolates.
In contrast to Etest, the disk diffusion method presented good accuracy (CA > 90%) only for penicillin and amoxicillin. As illustrated in Fig. 1, the two PRASEF isolates erroneously detected as penicillin susceptible by the diffusion disk exhibited an MIC of 16 μg/mL (cutoff point), and one of them presented an inhibition halo of 15 mm (cutoff point). Notably, all E. faecalis isolates erroneously categorized as resistant to ampicillin (n = 13; 17.6%) and amoxicillin (n = 4; 5.4%) by disk diffusion were PRASEF isolates (Fig. 1). They exhibited MIC values ranging from 2 to 4 µg/mL for amoxicillin or from 2 to 8 µg/mL for ampicillin and inhibition halos of 15–16 mm, which are close to the cutoff point of 17 mm.
Imipenem presented poor performance in the disk diffusion method (CA, 55.4%). High rates of both VME (37.5%) and ME (46.5%) were found for this beta-lactam; however, notably, these false susceptible and false resistant isolates were PRASEF isolates (Fig. 1). A high rate of VME (24.15%) but low ME (6.3%) was observed for piperacillin, and the CA rate was unacceptable (79.7%).
As illustrated in Fig. 1, the MIC values for the beta-lactams evaluated tended to be higher among the PRASEF isolates in comparison to those of PSASEF. Moreover, PSASEF isolates usually displayed larger disk zone diameters than PRASEF. Presumably, the inhibition zones of most of the PRASEF isolates correspond exactly or are extremely close to the CLSI breakpoint values. This could lead to higher misinterpretation in the isolates observed from this group using the disk diffusion method, particularly for imipenem and piperacillin.
Only 16 of the 74 E. faecalis isolates susceptible to ampicillin were susceptible to piperacillin using the broth dilution method in this study. In another study, it was reported that ampicillin results could be extrapolated to piperacillin in 98.2% of E. faecalis analyzed using the same method; however, as the penicillin susceptibility was not determined in that study, presumably, the isolates evaluated were mainly PSASEF [15].
Interestingly, a fuzzy zone edge with a double halo of growth inhibition was observed in all beta-lactams tested by disk diffusion and Etest only for the PRASEF isolates. This needs to be further assessed because it could influence the reading and the interpretative criteria of beta-lactam susceptibility testing. As generally recommended by CLSI, the inner zone of complete growth inhibition, observed by the naked eye, was interpreted in the present study.
Although the present study provides valuable insights into the population of penicillin-resistant E. faecalis and the methods for testing beta-lactam susceptibilities, it has certain limitations. First, we did not truly test for ampicillin- or amoxicillin-resistant isolates as determined by the reference method; however, it should be emphasized that these isolates are rarely found worldwide, which precluded the assessment of VME rates for both beta-lactams. Second, only isolates from one tertiary care hospital were included, which might have resulted in a bias due to in-hospital clonal expansion of a few lineages. In contrast, we estimated that the clonal bias must be limited since our collection covers eight years and derives from different wards.
In conclusion, Etest is efficient in testing beta-lactam susceptibilities of PRASEF isolates, whereas the disk diffusion method revealed poor performance, mainly for imipenem and piperacillin. Therefore, a careful analysis of antimicrobial susceptibility tests for the emerging population of penicillin-resistant E. faecalis is warranted, particularly for predicting piperacillin or imipenem susceptibility using the ampicillin results. Thus, further studies are needed to explore different disk brands and PRASEF isolates from other institutions.
Availability of data and materials
The datasets used and analyzed during the present study are available from the corresponding author upon reasonable request.
Abbreviations
- CA:
-
Categorical agreement
- CLSI:
-
Clinical and Laboratory Standards Institute
- EA:
-
Essential agreement
- EUCAST:
-
European Committee on Antimicrobial Susceptibility Testing
- E. faecalis:
-
Enterococcus faecalis
- ME:
-
Major error
- MIC:
-
Minimum inhibitory concentration
- PRASEF:
-
Penicillin-resistant, ampicillin-susceptible Enterococcus faecalis
- PSASEF:
-
Penicillin-susceptible, ampicillin-susceptible E. faecalis
- VME:
-
Very major error
References
Arias CA, Murray BE. The rise of the Enterococcus: beyond vancomycin resistance. Nat Rev Microbiol. 2012;10:266–78.
Teixeira LM, Carvalho MG, Shewmaker PL, Facklam RR. Enterococcus. In: Versalovic J, Carroll KC, Funke G, Jorgensen JH, Landry ML, Warnock DW, editors. Manual of clinical microbiology. 10th ed. Washington: ASM Press; 2011. p. 350–364.
Gagetti P, Bonofiglio L, García Gabarrot G, Kaufman S, Mollerach M, Vigliarolo L, von Specht M, Toresani I, Lopardo HA. Resistance to β-lactams in enterococci. Rev Argent Microbiol. 2019;51(2):179–83.
Infante VHP, Conceição N, Oliveira AG, Darini ALC. Evaluation of polymorphisms in pbp4 gene and genetic diversity in penicillin-resistant, ampicillin-susceptible Enterococcus faecalis from hospitals in different states in Brazil. FEMS Microb Let. 2016;363(7):1–5.
Tan YE, Ng LS, Tan TY. Evaluation of Enterococcus faecalis clinical isolates with ‘penicillin-resistant, ampicillin-susceptible’ phenotype as reported by Vitek-2 Compact system. Pathology. 2014;46(6):544–50.
Conceição N, de Oliveira CCHB, da Silva LE, de Souza LR, de Oliveira AG. Ampicillin susceptibility can predict in vitro susceptibility of penicillin-resistant, ampicillin-susceptible Enterococcus faecalis isolates to amoxicillin but not to imipenem and piperacillin. J Clin Microbiol. 2012;50(11):3729–31.
Guardabassi L, Larsen J, Skov R, Schonheyder HC. Gentamicin-resistant Enterococcus faecalis sequence type 6 with reduced penicillin susceptibility: diagnostic and therapeutic implications. J Clin Microbiol. 2010;48:3820–1.
Metzidie E, Manolis EM, Pournaras S, Sofianou D, Tsakris A. Spread of anunusual penicillin and imipenem resistant but ampicillin-susceptible phenotype among Enterococcus faecalis clinical isolates. J Antimicrob Chemother. 2005;57:158–60.
CLSI. Performance standards for antimicrobial susceptibility testing: 28th ed. CLSI supplement, M100. Wayne: Clinical and Laboratory Standards Institute; 2018.
European Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint tables for interpretation of MICs and zone diameters. Version 6.0, 2016. https://www.eucast.org. Accessed 17 Feb 2020.
Humphries RM, Ambler J, Mitchell SL, Castanheira M, Dingle T, Hindler JA, et al. CLSI methods development and standardization working group best practices for evaluation of antimicrobial susceptibility tests. J Clin Microb. 2018;56(4):e01934–e2017.
Croxatto A. Laboratory automation in clinical bacteriology. In: Tang Y-W, Stratton CW, editors. Advanced techniques in diagnostic microbiology. Cham: Springer; 2018. p. 15–32.
Conceição N, da Silva LE, Darini AL, Pitondo-Silva A, de Oliveira AG. Penicillin-resistant, ampicillin-susceptible Enterococcus faecalis of hospital origin: pbp4 gene polymorphism and genetic diversity. Infect Genet Evol. 2014;28:289–95.
Dutka-Malen S, Evers S, Courvalin P. Detection of glycopeptide resistance genotypes and identification to the species level of clinically relevant enterococci by PCR [published correction appears in J Clin Microbiol 1995 May;33(5):1434] [published correction appears in J Clin Microbiol. 1995 May;33(5):1434]. J Clin Microbiol. 1995;33(1):24–7.
Jones RN, Sutton LD, Cantrell HF, Lankford RB. Prediction of piperacillin-tazobactam susceptibility among Enterobacteriaceae, Pseudomonas aeruginosa, and other bacteria using ticarcillin-clavulanic acid, ceftazidime, and other broad-spectrum antimicrobial in vitro test results. Diagn Microbiol Infect Dis. 1994;20(3):143–9.
Acknowledgements
Not applicable.
Funding
Data collection and database construction were supported by Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG), Grant CBB APQ 1594/09. Data analysis was granted by Fundação de Ensino e Pesquisa de Uberaba (FUNEPU), Grant Number 2007/1107.
Author information
Authors and Affiliations
Contributions
NC, KLPO, LEPS, and LRCS carried out the study and helped to draft the manuscript. WFR and CCHBO participated in the design of the study and helped to draft the manuscript. AGO conceived the study, analyzed the data, and drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Conceição, N., Rodrigues, W.F., de Oliveira, K.L.P. et al. Beta-lactams susceptibility testing of penicillin-resistant, ampicillin-susceptible Enterococcus faecalis isolates: a comparative assessment of Etest and disk diffusion methods against broth dilution. Ann Clin Microbiol Antimicrob 19, 43 (2020). https://doi.org/10.1186/s12941-020-00386-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12941-020-00386-8