
Abstract
Background
Ionizing radiation is a well-known carcinogen. Chromosome aberrations, and in particular micronuclei represent an early biological predictor of cancer risk. There are well-documented associations of micronuclei with ionizing radiation dose in some radiation-exposed groups, although not all. That associations are not seen in all radiation-exposed groups may be because cells with micronuclei will not generally pass through mitosis, so that radiation-induced micronuclei decay, generally within a few years after exposure.
Methods
Buccal samples from a group of 111 male workers in Ukraine exposed to ionizing radiation during the cleanup activities at the Chornobyl nuclear power plant were studied. Samples were taken between 12 and 18 years after their last radiation exposure from the Chornobyl cleanup. The frequency of binucleated micronuclei was analyzed in relation to estimated bone marrow dose from the cleanup activities along with a number of environmental/occupational risk factors using Poisson regression adjusted for overdispersion.
Results
Among the 105 persons without a previous cancer diagnosis, the mean Chornobyl-related dose was 59.5 mSv (range 0–748.4 mSv). There was a borderline significant increase in micronuclei frequency among those reporting work as an industrial radiographer compared with all others, with a relative risk of 6.19 (95% CI 0.90, 31.08, 2-sided p = 0.0729), although this was based on a single person. There was a borderline significant positive radiation dose response for micronuclei frequency with increase in micronuclei per 1000 scored cells per Gy of 3.03 (95% CI -0.78, 7.65, 2-sided p = 0.1170), and a borderline significant reduction of excess relative MN prevalence with increasing time since last exposure (p = 0.0949). There was a significant (p = 0.0388) reduction in MN prevalence associated with bone X-ray exposure, but no significant trend (p = 0.3845) of MN prevalence with numbers of bone X-ray procedures.
Conclusions
There are indications of increasing trends of micronuclei prevalence with Chornobyl-cleanup-associated dose, and indications of reduction in radiation-associated excess prevalence of micronuclei with time after exposure. There are also indications of substantially increased micronuclei associated with work as an industrial radiographer. This analysis adds to the understanding of the long-term effects of low-dose radiation exposures on relevant cellular structures and methods appropriate for long-term radiation biodosimetry.
Similar content being viewed by others


Background
Ionizing radiation is a well-known carcinogen in humans, and a known clastogen leading to broken chromosomes. Chromosomal aberrations [1, 2] and more specifically formation of micronuclei (MN) in cell cytoplasm [3] could represent an early biological predictor of cancer risk. A cytological consequence of the induction of chromosome aberrations is the formation of MN that are observed in interphase cells as a result of a breakdown in repair of chromosomal breaks and general dysfunction of the chromosomal apparatus. MN originate from chromosome fragments or whole chromosomes that are not included in the main daughter nuclei during nuclear division [4,5,6]. MN rates in peripheral blood lymphocytes (PBL) are moderately rare, typically occurring at levels of 5–25 / 1000 cells [3] and at generally somewhat lower levels in the buccal mucosa, in the range 0.5–10 / 1000 cells [7, 8]. However, despite their moderate rarity, binucleated cells can be easily observed and studied [5, 8]. MN rates generally increase with age [9], although this is not universally observed [10]. MN can also be affected by cigarette smoking [9] and ionizing radiation dose [10], with a complex dependence on radiation dose, radiation energy and dose rate [11,12,13]. Because cells with MN will not generally pass through mitosis, radiation-induced MN generally decay fairly rapidly (over a period of years) after exposure [14].
It has been suggested that MN are suitable for biomonitoring genetic damage rates [5, 15, 16], in particular damage arising from ionizing radiation exposure, although this is rendered more difficult by the dependence of MN prevalence on age and cigarette smoking. Many studies have shown that the number of radiation-induced MN is strongly correlated with dose and quality of radiation [17,18,19,20,21]. The dose response for MN following a single acute low LET radiation exposure is known to be strongly curvilinear (upward curving), although a more linear relationship is known for high LET radiation exposure [22]. After whole-body exposure with low linear energy transfer (LET) radiation, doses down to 0.1 Gy can be detected [22].
Sari-Minodier et al. [4] evaluated the induction of MN in relation to occupational radiation exposure in a group of 132 exposed hospital workers and 69 controls, adjusting for the possible confounding effects of gender, age, smoking status, familial cancer history and medical irradiation. They demonstrated more frequent MN in the exposed group compared with controls despite the very low levels of exposure (generally <5 mSv / year) [4].
Several studies have been conducted in Chornobyl-exposed children in Belarus, demonstrating elevated rates of MN compared to those from the control areas with little or no radiation exposure [16, 23, 24]. A study of MN in intact cells exposed to serum samples from Chornobyl cleanup workers in Belarus 20 years after exposure observed a significant elevation in MN counts, suggestive of clastogenic factors in their exposed serum which could induce instability [25]. It has been suggested that radiation is one of a number of agents capable of inducing such MN-associated instability [15].
The present study is aimed at evaluating MN in buccal cells in a group of liquidators (cleanup workers) following the Chornobyl accident, collected 16–18 years after exposure. We assess the frequency of MN in relation to various environmental and occupational risk factors, with particular emphasis on assessing excess MN associated with radiation exposure from the Chornobyl accident, and possible modifications by age at exposure and the time between radiation exposure and buccal cell sampling.
Methods
Subjects
The study included 111 male members (mean age at first exposure 44.0 years; range 27.8–63.0 years) of the Ukrainian cohort of cleanup workers, who were exposed to different doses of ionizing radiation during the cleanup activities at the Chornobyl nuclear power plant. Subject recruitment and study methods of the previous case-control studies of leukemia nested in the cohort have been described previously [26, 27]. Briefly, all subjects underwent interview for dose reconstruction using the special questionnaire and doses were reconstructed using the Realistic Analytical Dose Reconstruction with Uncertainty Estimation (RADRUE) method [28]. RADRUE has been subject to extensive validation, which we shall consider further in the Discussion. Information about the influence of environmental factors other than Chornobyl radiation, habits, and therapeutic and diagnostic radiological procedures was collected via a special questionnaire [29]. During interview, study participants were asked to donate buccal cell samples. The majority of those who agreed were controls previously involved in case-control studies [26, 27], but a small number of cases (n = 3) also agreed to donate buccal cell samples. The National Research Center for Radiation Medicine (NRCRM) in Kyiv and University of California San Francisco (UCSF) Institutional Review Boards approved this study. Before enrollment, each patient gave written informed consent.
Collection of buccal cell samples for MN analysis.
Exfoliated buccal cells were obtained from the study subjects between November 2002 and March 2004, i.e., 16 to 18 years after the Chornobyl accident. After signing the consent form, commercial “Scope” mouthwash from a plastic container was vigorously swished by the subject in their mouth for 45 s. The throat was not cleared or gargled during the procedure. The mouthwash was then expectorated back into the container which was held close to the mouth. The containers were then tightly sealed and sent back to NRCRM within 24 h of the sample collection. The mouthwash samples were transferred to a 15 ml conical tube and centrifuged at 1500 x g for 15 min. The supernatant was decanted, and the cell pellet was resuspended in 3 ml of TE buffer solution [Tris-EDTA (100 x concentration; pH 8.0) in diethylpyrocarbonate (DEPC) treated water; 1:100 solution]. The 3 ml suspension of cells was distributed into cryovials and stored at -80C. The cells were re-suspended, dropped onto slides and dried at room temperature, and staining solution added, consisting of 10 ml of 0.5% propidium iodide in phosphate-buffered saline (PBS) containing 10% Glycerol. We assess the advantages of this method of buccal cell sampling in comparison with phlebotomy-derived PBL and cytobrush-exfoliated buccal cell samples in the Discussion.
Because of a priori doubts as to the effect of prior chemotherapy and radiotherapy, most analyses (Tables 1, 2 and 3, Fig. 1) exclude 6 persons recorded as having a previous tumor, the three persons reporting treatment for radiotherapy or chemotherapy for cancer (one person reporting both types of therapy), and the three leukemia cases known from a previous study [27]. Exclusion of these 6 case resulted in an analysis dataset of 105 persons. However, we also provide in Appendix 2 Tables 8 and 9 certain analyses with these 6 individuals included.

Microscopy
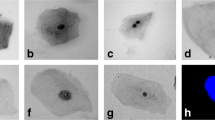
Slides each containing 1000 binucleated cells were scored for micronuclei via oil immersion light microscopy with 900× (40 × 15 × 1.5) magnification. Binucleated cells were scanned and the number of cells with micronuclei was counted. The slides were randomized and coded so that the scorer was not aware of subject ID or dose. The criteria for selecting binucleated cells to score are the following:
a) binucleated cells with main nuclei that are separate and of approximately equal size;
b) main nuclei that touch and even overlap as long as nuclear boundaries can be distinguished; and
c) main nuclei that are linked by nucleoplasmic bridges.
Not scored cells included: trinucleated, quadronucleated, or other multinucleated cells.
Dosimetry
A time-and-motion method of retrospective dose reconstruction in cleanup workers, known as RADRUE, was developed for the Leukemia Study and for a similar study conducted in Belarus, Russia, and Baltic countries [30] by an international group of scientists including experts from Belarus, France, Russia, the United States, and Ukraine [31, 32]. The method used combined data on work history from dosimetric questionnaires with field radioactivity measurements to estimate individual bone marrow doses for all study subjects. In-person interviews were conducted by trained interviewers and included questions concerning locations of work and residence while in the 30-km exclusion zone around the Chornobyl nuclear power plant, types of work, transportation routes, and corresponding dates. All study subjects were necessarily alive at the time of buccal cell sampling and the associated interview, so that there is not the complication of use of proxy subjects that previous analyses of the underlying case-control dataset have faced [26, 27]. Our analyses were based on the cumulative doses derived as the sums of the arithmetic means of the annual 1986–1990 bone marrow doses estimated by generating 10,000 realizations of dose predictions from RADRUE [31].
Statistical methods
To evaluate the relationship between cumulative estimated dose and MN, we fitted an additive model, linear-exponential in dose, in which the expected number of MN for individual i was given by:
where Scored i is the number of whole scored cells, \( {\left({Z}_{il}\right)}_{l=1}^N \)are various other variables (including a polynomial function of age at sampling, cigarette smoking, alcohol consumption, chemotherapy and radiotherapy exposure, diagnostic X-rays etc), and D i is the total buccal dose (in Gy), derived from questionnaire-assessed Chornobyl-related exposure (via RADRUE). The linear-exponential form of dose response used in model (1) is a standard one in analysis of radiobiological data [33], with the linear term αD i representing the MN induction effect, and the exponential term exp[βD i ] representing a sterilization effect. We also fitted a model for the relative MN rate, again linear-exponential in dose:
Exposure to various medical and occupational risk factors was qualitatively assessed, and taken into account in the regression model via the terms \( {\left({Z}_{il}\right)}_{l=1}^N \). In order to adequately fit MN prevalence taking account of all factors other than radiation, we considered variables taken from a candidate set of variables that included various occupational (including Chornobyl-related), medical and other terms, some derived from a previous study of these workers [27], and polynomial terms in the (centered) age at buccal sampling, (age i − 60.104)k, with integral k between 1 and 8, given in Appendix 1 Table 6. Age at buccal sampling, age i , was centered at its mean value, 60.104 years in the full sample, in order to improve the stability of parameter estimates. In order to avoid over-parameterized models, the Akaike Information Criterion (AIC) [34, 35] was employed to select the optimal subset of descriptive variables from this set. AIC penalizes against overfitting by adding 2 x [number of fitted parameters] to the model deviance. A mixed forward-backward stepwise algorithm was used to select the set of variables minimizing AIC, using R [36]. The indicated optimal models were augmented to make them polynomially complete in age at buccal sampling, so that if the optimal model included a variable (age i − 60.104)k for some index k, then all terms (age i − 60.104)m for indices 0 ≤ m ≤ k were also included in the model. The optimal set of variables are given in Appendix 1 Table 7.
Additional models analogous to models (1) and (2) were also fitted, in which adjustment was made for the modifying effects of age at first exposure, e i , or time between last exposure and buccal cell sampling, t i , on the radiation-associated absolute excess risk:
and the radiation-associated relative excess risk
The age at first exposure and time since last exposure variables were centered by subtracting their mean values, 43.593 years and 15.870 years among those without cancer, respectively, in order to stabilize parameter estimates. [It should be noted that without a modifying effect of age (or other variables) in the background term, \( \exp \left[\sum_{l=1}^N{\gamma}_l{Z}_{il}\right] \), precisely the same p-values and estimates of these coefficients (δ , ϕ) would be obtained in the relative risk model (4) as with the additive model (3), a consequence of the algebraic equivalence of these models in this special case.] Tables 2, 3, 4 and 5 detail the model fits to the MN frequency data, via Poisson maximum likelihood, and associated parameter estimates. Because of indications of marked over-dispersion, in the analyses (Tables 1, 2, 3, 4 and 5) all p-values (which are 2-sided) are computed using F-tests, derived from quasi-likelihood techniques [37], and the square roots of the associated variance inflation factors (defined by ϕ = deviance/df) are used to scale profile-likelihood confidence intervals in the standard way, i.e., by multiplying the distance of confidence limit to the best estimate by the square root of the inflation factor. Very similar estimates of the variance inflation factor derived in this way, which after adjustment for the background variables were about 1.4–1.5, were yielded by use of quasi-likelihood models in R [36], taking account of overdispersion [37]. Models were fitted using R [36] and Epicure [38]. Although all p-values are 2-sided, arguably 1-sided p-values (which would be about half the values given) are possibly more relevant for certain of the tests that we perform, given that one would expect MN prevalence only to increase with increasing dose. We emphasize in a few relevant places the two-sided nature of the relevant tests.
Results
Among the 105 persons without previous cancer the estimated mean Chornobyl-related bone marrow dose was 59.5 mSv (range 0–748.4 mSv) and the mean age at first exposure was 43.6 years (range 27.8–63.0 years). Among the same group with information on years since last exposure, the mean years since last exposure was 15.9 years (range 12.4–17.8 years). There are variations of MN prevalence with days of active work in the Chornobyl exclusion zone, being particularly high among those working 50–99 days, by type of work as a cleanup worker, and among those 25 persons in military occupations (Table 1). Minimizing AIC led to inclusion of 11 variables, providing a parsimonious model of underlying MN prevalence that includes a 5th order polynomial in age at buccal sample (Appendix 1 Table 7).
Table 2 demonstrates that there is a borderline significant increase in MN frequency among those reporting work as an industrial radiographer, with a relative risk of 6.19 (95% CI 0.90, 31.08, p = 0.0729). There are weak indications of increased MN frequency associated with radiation work apart from Chornobyl, or with radiation work in the nuclear industry, with relative risks of 1.68 (95% CI 0.68, 4.03, p = 0.2584), and 1.61 (95% CI 0.62, 3.98, p = 0.3195), respectively (Table 2), although there was a borderline significant reduction in MN prevalence among those reporting radiation work in the army, with a relative risk of 0.27 (95% CI 0.03, 1.14, p = 0.0721) (Table 2). There was a significant decrease in numbers of MN among those reporting bone X-rays, with a relative risk of 0.60 (95% CI 0.37, 0.96, p = 0.0388), although there were only weak indications of a (negative) trend with numbers of bone X-rays (p = 0.3845) (Table 2).
Table 3 demonstrates that after adjustment for some of these variables, there are borderline significant indications of a positive Chornobyl-related radiation dose response for the absolute risk of MN of 3.03 MN per 1000 scored cells per Gy (95% CI -0.78, 7.65, 2-sided p = 0.1170); there is somewhat weaker evidence of such trends using a relative risk model (2-sided p = 0.1902). There was some elevation of MN in a group exposed to intermediate levels of dose, 100–250 mGy, also at higher levels of dose, 500+ mGy (Fig. 1, Table 1). There is no evidence of a linear-exponential dose response, whether using absolute or relative risk models (p = 0.5710, p = 0.4205, respectively, Table 3).
Table 4 demonstrates that there was a borderline significant reduction of excess relative MN prevalence with increasing time since last exposure (p = 0.0949), and there are somewhat weaker indications (p = 0.2733) of a reducing trend in absolute excess MN prevalence with increasing time since last exposure. Variations of radiation-associated MN prevalence with age at first exposure are somewhat weaker, whether using relative risk or absolute risk models (p = 0.1368, p = 0.3215, respectively). The modifying effect of time since last exposure, whether on relative or absolute risk, is notably large, ϕ = − 0.753 year−1 or ϕ = − 0.464 year−1, respectively. Table 5 demonstrates that there are only weak indications of significant modifying effects on the MN Chornobyl-related dose response by number of days of work, or by number of active days of work, in the Chornobyl exclusion zone, whether in relation to absolute (p = 0.2808, p = 0.2590, respectively) or relative risk (p = 0.1671, p = 0.2156, respectively) models. There are no indications of modifications of MN prevalence by type of liquidator, cigarette smoking, or alcohol consumption, whether in relation to absolute (p = 0.6681, p = 0.8232, p = 0.7291, respectively) or relative risk (p = 0.7678, p = 0.6922, p = 0.7246, respectively) (Table 5).
Analyses including the 6 individuals with cancer were not markedly different (Appendix 2 Tables 8 and 9).
Discussion
We observed a large and borderline significant (2-sided p = 0.0729) increase in MN frequency among those reporting work as an industrial radiographer, although this finding was based on a single case. We also observed borderline-significant indications of a positive Chornobyl-related radiation dose response for MN (2-sided p = 0.1170). There is a substantial and borderline significant (p = 0.0949) reduction of Chornobyl-dose-related relative prevalence with increasing time since last exposure. We observed a significant decrease in numbers of MN among those reporting bone X-rays (2-sided p = 0.0388), but there was no significant trend in MN prevalence with numbers of bone X-rays.
The MN assay using buccal cells is a minimally invasive method for studying DNA damage, chromosomal instability, cell death and the regenerative potential of human buccal mucosal tissue. This method is increasingly used in molecular epidemiological studies for investigating the impact of nutrition, lifestyle factors, genotoxic exposure and genotype on DNA damage, chromosome mis-segregation and cell death. Although MN in buccal mucosa occur at a lower frequency than in PBL [3, 7, 8], there is no reason to exclude their use for this reason. Biologically one would expect the excess MN to persist to the same relative extent in various tissues of the body, so that it is not unreasonable to examine any radiation-exposed tissue in the body, in particular the buccal mucosa, for this marker of exposure. Although there are some very high skin doses due to low energy beta emitters [39], in the Chornobyl liquidators “photon energy spectra varied from one location to another and from one time period to another but were generally centered between 0.15 and 0.4 MeV” [32]. In the range of energy from 0.15 to 0.4 MeV, dose does not vary much with energy or from one organ/tissue to another [40]. Both blood and epithelial tissue are highly regenerative tissues with a continuous need for repopulation and a base of stem cells needed for lifetime renewal. Because of the long time between exposure and sampling, the damage measured here is primarily of the buccal stem cells. The biomarkers measured in this assay have been associated with increased risk of accelerated ageing, cancer and neurodegenerative diseases [41]. However, because cells with MN will not generally pass through mitosis, MN generally decay fairly rapidly, over a few years, after mutagenic exposure. In particular, there is human in vivo data demonstrating this. A study of a pregnant woman and her then in utero child, both heavily exposed (to several Gy) from an orphan 60Co source, demonstrated a progressive decline in MN in mother and daughter over the period from 41 days to 16 years after the accident [42]. This may also explain our generally null findings in relation to radiation exposure from the Chornobyl accident, last exposure from which occurred between 12 and 18 years prior to buccal cell sampling. Although not statistically significant, there is a pronounced negative modifying effect of time since exposure on the association of MN with radiation dose (Table 4).
The excess of MN that we observed among those reporting work as industrial radiographers, with a relative risk of 6.19 (95% CI 0.90, 31.08) (Table 2), should be compared with those in a study of Sari-Minodier et al. [43], who found a smaller, approximately two-fold, increase in a group of 29 radiographers compared with a group of 24 controls. The confidence intervals on our relative risks are wide, and so the relative risks in these two groups are statistically compatible despite these disparate point estimates.
Increases in MN frequency have been observed in some groups exposed to dental and other diagnostic X-rays procedures [7, 44], although not in many others [45,46,47,48,49]. In all these studies comparisons were made of MN within subjects before and shortly after (generally within a few days) of X-ray exposure. It is interesting that although negative for MN, the studies of Ribeiro et al. [45, 47], Angelieri et al. [46, 49] and Lorenzoni et al. [48] showed increases in the cytotoxic endpoints of karrhyorexis, pyknosis, and karyolysis after X-ray exposure, suggesting a substantial degree of induced cell death among buccal mucosa. This may explain the reduced MN frequency that we observed, presumably a much longer time after bone X-ray exposure than in these earlier studies. Unfortunately the cytotoxic endpoints considered in these earlier studies (karrhyorexis, pyknosis, and karyolysis) were not evaluated here. In addition to induced cell death of damaged mucosa, bone X-ray exposure may stimulate enhanced DNA repair as a hormetic effect [50].
A study of 132 radiation-exposed hospital workers and 69 controls matched for gender, age and smoking habits previously showed that chromosomal damage leading to micronucleated lymphocytes is more frequent after exposure to ionizing radiation than in controls, despite the very low dose levels recorded during a 10-year period [4]. The effect was significantly greater in females than in males, and a significant correlation between age and MN rates was observed in females but not in males. There was no significant effect of cigarette smoking. A large study of 1392 radiation workers and 143 controls in China demonstrated increased MN prevalence at relatively low occupational radiation doses (~50 mSv equivalent dose), and variation of MN prevalence also with exposure time [51]. A significant excess prevalence (p < 0.001) of MN in PBL was observed in a group of 25 exposed male workers compared with a group of 25 age-matched controls, with borderline significant indications (p = 0.079) of an increasing dose response [52]; exposure occurred 32–41 years previously. In PBL of patients receiving radiotherapy, MN yield increased with increasing equivalent dose and there was a general decline in MN yields with increasing length of follow-up, with considerable variation between individuals [53]. Whether this variation reflects inter-individual differences in susceptibility to radiation-induced DNA damage, or simply inter-individual differences in ability to clear MN, is unknown. However, in the period from 19 to 75 months after treatment, seven of thirteen patients showed higher MN yields than their respective levels before radiotherapy, indicating the persistence of radiation-induced residual cytogenetic damage in some subjects [53]. Such differences could be influenced by numerous subject characteristics, including germline genetics. However, the relatively short interval between radiation exposure and sampling should be noted. Because we performed analysis a long time after radiation exposure (e.g., at least 12.4 years after exposure from the Chornobyl accident) we used various methods to attempt to increase the MN assay sensitivity, although we did not use the cytokinesis-block micronucleus test (CB-MNT) [54]. The main analysis assessed counts of binucleated cells, commonly regarded as a type of cell with defective cytokinesis [8].
The method of alcohol-based mouthwash-expectorated buccal cell sampling that we employ is less commonly used than the cytobrush-exfoliated buccal cell collection method [9]. However, there have been a number of recent studies in the literature that use this method of mouthwash-mediated buccal cell collection, in particular those of Lum and Le Marchand [55], Garcia-Closas et al. [56], and Andrisin et al. [57]. As highlighted by Garcia-Closas et al. [56] and Lum and Le Marchand [55] the use of alcohol-based mouthwash has certain decisive advantages over cytobrush-exfoliated buccal cell collection in the proportion of high molecular weight DNA extracted and its stability, and the much lower proportion of non-human (bacterial) DNA content. As shown by Andrisin et al. [57] the method also produces samples with stable DNA content, that can be kept at room temperature for up to 90 days, unlike cytobrush-exfoliated buccal cell samples, that require processing within a matter of days; as shown by Walsh et al. [58] there is significant bacterial contamination on cytobrush-collected buccal samples within 4 days of sample collection. The method is also more acceptable to study subjects than PBL samples obtained via phlebotomy or cytobrush-exfoliated buccal cell collection, being less invasive; it is also preferable to saline-mouthwash collected buccal samples because of the more agreeable aftertaste. Admittedly not all of these advantages of the mouthwash method matter here, since all samples were processed within a few days of collection. Also, as discussed in the Introduction the baseline frequency of MN produced by this method is lower than for PBL.
A refinement of the assay, using a pan-centromeric DNA probe labeling the centromeric region, discriminates between centromere-negative MN (C-MN) and centromere-positive MN (C+MN). Significantly higher frequency of C-MN have been observed using this assay in a number of radiation-exposed groups exposed at relatively low levels of radiation dose (generally <100 mSv) [43, 59], also in an individual receiving a large (65 Gy) therapeutic dose [60]. The finding of significantly elevated MN prevalence in immortalized HPV-G cells exposed to serum samples from Chornobyl cleanup workers from Belarus some 20 years after exposure is of interest [25]. However, the study did not directly examine the rates of MN in the blood cells of the Belarus cleanup workers, but rather the effects of the soluble factors contained in sera from radiation-exposed subjects on human immortalized reporter cells treated with these sera, and as such is only tangentially relevant to the present study.
Set against that, there are a number of null studies of MN in buccal cells. A study of 15 heavy smokers and 17 non-smokers exposed to panoramic dental X-rays evaluated MN in exfoliated oral mucosa cells, and found no statistically significant differences in MN rates before versus after exposure either in smokers or non-smokers, although there were differences in measures of induced cell death (pyknosis, karyolysis, and karyorrhexis) [46]. A study of 31 healthy individuals evaluated MN before and 10 days after X-ray dental radiography and observed similar frequencies of MN, karyolysis and pyknosis over time (p > 0.90), although chromatin condensation and karyorrhexis increased significantly after exposure (p < 0.0001) [61]. These and other studies suggest an absence of MN induction after low dose radiation exposure, although there appear to be cytotoxic effects caused by increasing apoptosis [61, 62].
There has also been no demonstrated dose-related increase in MN frequency in the bone marrow cells of a small sample of Hiroshima atomic bomb survivors [63]. It is possible that the interval between exposure and sampling, about 5 years, may have contributed to this null finding. Interestingly, Oesterle and Finch observed internuclear bridges in the marrow smears in a large proportion of the heavily exposed (>3 Gy) survivors, and a substantial excess karyomere frequency in a group exposed to even larger doses (> 6 Gy) [63].
Bone marrow doses were estimated here by the RADRUE method [28]. RADRUE has been subject to extensive validation, in particular with thermoluminescent dosimetry (TLD) badges worn by certain reliably film-badged groups of workers (AC-605 liquidators), and various biological dosimeters, in particular electron paramagnetic resonance (EPR) in teeth and fluorescence in situ hybridization (FISH) in peripheral blood lymphocytes, as documented in the report of Kryuchkov et al. [32]. Although RADRUE dose estimates would not be biased, nevertheless there are considerable uncertainties in RADRUE doses, which have been estimated to have mean geometric standard deviation (GSD) about 1.9; the GSD was considerably higher, 4–6, when the subject was deceased and a proxy had to be used, but this is not relevant here, because all study subjects were alive at the time of interview [32]. These errors are of complex form, very likely a mixture of Berkson and classical type [64]. Classical dose errors would be expected to bias trends with dose towards the null; Berkson-type errors would not bias dose response trends, but would inflate the associated confidence intervals [64, 65].
Genome sequencing has uncovered a new mutational phenomenon called chromothripsis, characterized by extensive genomic rearrangements and an oscillating pattern of DNA copy number levels, all restricted to a few chromosomes. Using a combination of live-cell imaging and single-cell genome sequencing, Zhang et al. [66] demonstrated that MN formation can generate a spectrum of genomic rearrangements, some of which recapitulate known features of chromothripsis. These events are restricted to the mis-segregated chromosome and occur within one cell division. Zhang et al. [66] demonstrated that the mechanism for chromothripsis may involve the fragmentation and subsequent reassembly of a single chromatid from a MN. Chromothripsis has been linked with proton beam irradiation in vitro [67] and has also been shown to drive telomerase reactivation in CLL [68], the most common cancer experienced by Chornobyl cleanup workers.
In our study buccal cells rather than PBL have been used, but as above the only complication this is likely to introduce is the somewhat lower prevalence of MN. The study has some limitations. The dose from Chornobyl-related exposure was derived from questionnaire-based assessments, using RADRUE, and all other information relating to occupational and medical exposure was also questionnaire-derived. There was no assessment of radiation dose from radiotherapy or from other sources, nor was there any assessment made of the timing of the medical procedures and types of occupational exposure. The design of the questionnaire given to the study subjects made it impossible to determine the sequence of exposure of ionizing radiation and the possible confounding factors. That said, since we found no effect of any other occupational or medical factor, it is perhaps unlikely that there would be confounding due to these factors. Fourteen subjects had evidence of treatment for cancer, but exclusion of these made no difference to inference on dose response. This study gives no answer to the question of whether previous low-dose radiation exposure could change DNA susceptibility to chemo- or radiotherapy and elongate the time of damage persistence, that might be revealed by the MN assay.
As well as the long time interval between Chornobyl-related radiation exposure and buccal cell sampling, another factor that must be considered is the generally modest levels of radiation dose. The mean dose in the present study was 59.5 mSv, with a maximum dose of 748.4 mSv. Data from an experiment involving ex vivo 60Co-gamma irradiation of fibroblasts suggests that the minimal dose at which an elevated level of MN can be observed is about 200–250 mGy, minimally dependent on age [69]; only 10 of our cases had doses in excess of 250 mSv (Table 1, Appendix 1 Table 6). Set against that, a number of occupationally radiation-exposed groups observed increases in MN at levels of dose somewhat lower than the present study [4, 51]. A more detailed investigation of our results is still needed. Quantification of the precise dose-response relationship between MN levels and radiation dose in in vitro models could inform future studies in humans. However, to be most germane, such studies must also assess the effects of various time intervals between radiation exposure and cell sampling.
Conclusions
There are indications of increasing trends of MN prevalence with Chornobyl-cleanup-associated dose, and indications of reduction in radiation-associated excess prevalence of MN with time after radiation exposure. There are also indications of substantially increased MN prevalence associated with work as an industrial radiographer, although based on a single case. This analysis adds to the understanding of the long-term effects of low-dose radiation exposures on relevant cellular structures and methods appropriate for long-term radiation biodosimetry.
References
Norppa H, Bonassi S, Hansteen IL, Hagmar L, Stromberg U, Rossner P, et al. Chromosomal aberrations and SCEs as biomarkers of cancer risk. Mutat Res. 2006;600:37–45.
Boffetta P, van der Hel O, Norppa H, Fabianova E, Fucic A, Gundy S, et al. Chromosomal aberrations and cancer risk: results of a cohort study from Central Europe. Am J Epidemiol. 2007;165:36–43.
Bonassi S, El-Zein R, Bolognesi C, Fenech M. Micronuclei frequency in peripheral blood lymphocytes and cancer risk: evidence from human studies. Mutagenesis. 2011;26:93–100.
Sari-Minodier I, Orsière T, Auquier P, Martin F, Botta A. Cytogenetic monitoring by use of the micronucleus assay among hospital workers exposed to low doses of ionizing radiation. Mutat Res. 2007;629:111–21.
Fenech M, Bolognesi C, Kirsch-Volders M, Bonassi S, Zeiger E, Knasmüller S, Holland N: Harmonisation of the micronucleus assay in human buccal cells--a Human Micronucleus (HUMN) project (www.humn.org) initiative commencing in 2007. Mutagenesis 2007, 22:3-4.
Norppa H, Falck GC. What do human micronuclei contain? Mutagenesis. 2003;18:221–33.
Preethi N, Chikkanarasaiah N, Bethur SS. Genotoxic effects of X-rays in buccal mucosal cells in children subjected to dental radiographs. BDJOpen. 2016;2:16001.
Holland N, Bolognesi C, Kirsch-Volders M, Bonassi S, Zeiger E, Knasmueller S, et al. The micronucleus assay in human buccal cells as a tool for biomonitoring DNA damage: the HUMN project perspective on current status and knowledge gaps. Mutat Res. 2008;659:93–108.
Fenech M, Holland N, Zeiger E, Chang WP, Burgaz S, Thomas P, et al. The HUMN and HUMNxL international collaboration projects on human micronucleus assays in lymphocytes and buccal cells--past, present and future. Mutagenesis. 2011;26:239–45.
Prosser JS, Moquet JE, Lloyd DC, Edwards AA. Radiation induction of micronuclei in human lymphocytes. Mutat Res. 1988;199:37–45.
Vral A, Thierens H, De Ridder L. Study of dose-rate and split-dose effects on the in vitro micronucleus yield in human lymphocytes exposed to X-rays. Int J Radiat Biol. 1992;61:777–84.
Bhat NN, Rao BS. Dose rate effect on micronuclei induction in cytokinesis blocked human peripheral blood lymphocytes. Radiat Prot Dosimetry. 2003;106:45–52.
Noll M, Böck E, Schöner W, Egger P, Wolf C, Rüdiger H, et al. Correlation of the LET-dependent TL-response of LIF:Mg, Ti TL-dosemeters and gentoxic endpoints after proton irradiation. Appl Radiat Isot. 2000;52:1135–8.
Livingston GK, Falk RB, Schmid E. Effect of occupational radiation exposures on chromosome aberration rates in former plutonium workers. Radiat Res. 2006;166:89–97.
Fenech M. Cytokinesis-block micronucleus assay evolves into a "cytome" assay of chromosomal instability, mitotic dysfunction and cell death. Mutat Res. 2006;600:58–66.
Fenech M, Perepetskaya G, Mikhalevich L. A more comprehensive application of the micronucleus technique for biomonitoring of genetic damage rates in human populations--experiences from the Chernobyl catastrophe. Environ Mol Mutagen. 1997;30:112–8.
Verhaegen F, Vral A. Sensitivity of micronucleus induction in human lymphocytes to low-LET radiation qualities: RBE and correlation of RBE and LET. Radiat Res. 1994;139:208–13.
Vral A, Verhaegen F, Thierens H, De Ridder L. Micronuclei induced by fast neutrons versus 60Co γ-rays in human peripheral blood lymphocytes. Int J Radiat Biol. 1994;65:321–8.
Wuttke K, Müller W-U, Streffer C. The sensitivity of the in vitro cytokinesis-blocked micronucleus assay in lymphocytes for different and combined radiation qualities. Strahlenther Onkol. 1998;174:262–8.
Gersey B, Sodolak J, Hada M, Saganti P, Wilkins R, Cucinotta F, et al. Micronuclei induction in human fibroblasts exposed in vitro to Los Alamos high-energy neutrons. Adv Space Res. 2007;40:1754–7.
Willems P, August L, Slabbert J, Romm H, Oestreicher U, Thierens H, et al. Automated micronucleus (MN) scoring for population triage in case of large scale radiation events. Int J Radiat Biol. 2010;86:2–11.
Vral A, Fenech M, Thierens H. The micronucleus assay as a biological dosimeter of in vivo ionising radiation exposure. Mutagenesis. 2011;26:11–7.
Zotti-Martelli L, Migliore L, Panasiuk G, Barale R. Micronucleus frequency in Gomel (Belarus) children affected and not affected by thyroid cancer. Mutat Res. 1999;440:35–43.
Vorobtsova IE. Semenov AV: [Complex cytogenetic characteristic of people suffered from Chernobyl accident]. Radiats Biol Radioecol. 2006;46:140–51.
Marozik P, Mothersill C, Seymour CB, Mosse I, Melnov S. Bystander effects induced by serum from survivors of the Chernobyl accident. Exp Hematol. 2007;35:55–63.
Romanenko A, Bebeshko V, Hatch M, Bazyka D, Finch S, Dyagil I, et al. The Ukrainian-American study of leukemia and related disorders among Chornobyl cleanup workers from Ukraine: I. Study methods. Radiat Res. 2008;170:691–7.
Zablotska LB, Bazyka D, Lubin JH, Gudzenko N, Little MP, Hatch M, et al. Radiation and the risk of chronic lymphocytic and other leukemias among Chornobyl cleanup workers. Environ Health Perspect. 2013;121:59–65.
Chumak V, Drozdovitch V, Kryuchkov V, Bakhanova E, Babkina N, Bazyka D, et al. Dosimetry Support of the Ukrainian-American Case-control Study of Leukemia and Related Disorders Among Chornobyl Cleanup Workers. Health Phys. 2015;109:296–301.
Gudzenko N, Hatch M, Bazyka D, Dyagil I, Reiss RF, Brenner A, et al. Non-radiation risk factors for leukemia: A case-control study among Chornobyl cleanup workers in Ukraine. Environ Res. 2015;142:72–6.
Kesminiene A, Evrard AS, Ivanov VK, Malakhova IV, Kurtinaitis J, Stengrevics A, et al. Risk of hematological malignancies among Chernobyl liquidators. Radiat Res. 2008;170:721–35.
Chumak VV, Romanenko AY, Voilleque PG, Bakhanova EV, Gudzenko N, Hatch M, et al. The Ukrainian-American study of leukemia and related disorders among Chornobyl cleanup workers from Ukraine: II. Estimation of bone marrow doses. Radiat Res. 2008;170:698–710.
Kryuchkov V, Chumak V, Maceika E, Anspaugh LR, Cardis E, Bakhanova E, et al. RADRUE method for reconstruction of external photon doses for Chernobyl liquidators in epidemiological studies. Health Phys. 2009;97:275–98.
United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR): Sources and effects of ionizing radiation. UNSCEAR 1993 report to the General Assembly, with scientific annexes. vol. E.94.IX.2. pp. 1-922. New York: United Nations; 1993:1–922.
Akaike H: Information theory and an extension of the maximum likelihood principle. In 2nd International Symposium on Information Theory (Petrov BN, Czáki F eds.). pp. 267–281. Budapest: Akadémiai Kiadó; 1973:267-281.
Akaike H. Likelihood of a model and information criteria. J Econometrics. 1981;16:3–14.
R Project version 3.2.2: R version 3.2.2 https://www.r-project.org/. Comprehensive R Archive Network (CRAN); 2015.
McCullagh P, Nelder JA: Generalized linear models. 2nd edition. In Monographs on statistics and applied probability 37. pp. 1-526. Boca Raton, FL: Chapman and Hall/CRC; 1989:1–526.
Risk Sciences International. Epicure version 2.0.1.0. 55 Metcalfe, K1P 6L5, Canada: Risk Sciences International; 2015.
United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR): UNSCEAR 2008 Report to the General Assembly with Scientific Annexes. Volume II Annex D. Health effects due to radiation from the Chernobyl accident. pp. 1–173. New York; 2011:1-173.
International Commission on Radiological Protection (ICRP). Conversion coefficients for radiological protection quantities for external radiation exposures. ICRP Publication 116. Ann ICRP. 2010;40(2-5):1–257.
Thomas P, Holland N, Bolognesi C, Kirsch-Volders M, Bonassi S, Zeiger E, et al. Buccal micronucleus cytome assay. Nat Protoc. 2009;4:825–37.
Liu Q-J, Lu X, Zhao H, Chen S, Wang M-M, Bai Y, et al. Cytogenetic analysis in 16-year follow-up study of a mother and fetus exposed in a radiation accident in Xinzhou, China. Mutat Res. 2013;755:68–72.
Sari-Minodier I, Orsière T, Bellon L, Pompili J, Sapin C, Botta A. Cytogenetic monitoring of industrial radiographers using the micronucleus assay. Mutat Res. 2002;521:37–46.
Arora P, Devi P, Wazir SS. Evaluation of genotoxicity in patients subjected to panoramic radiography by micronucleus assay on epithelial cells of the oral mucosa. J Dent (Tehran). 2014;11:47–55.
Ribeiro DA, de Oliveira G, de Castro G, Angelieri F. Cytogenetic biomonitoring in patients exposed to dental X-rays: comparison between adults and children. Dentomaxillofac Radiol. 2008;37:404–7.
Angelieri F, de Cássia Gonçalves Moleirinho T, Carlin V, Oshima CTF, Ribeiro DA. Biomonitoring of oral epithelial cells in smokers and non-smokers submitted to panoramic X-ray: comparison between buccal mucosa and lateral border of the tongue. Clin Oral Investig. 2010;14:669–74.
Ribeiro DA, Sannomiya EK, Pozzi R, Miranda SR, Angelieri F. Cellular death but not genetic damage in oral mucosa cells after exposure to digital lateral radiography. Clin Oral Investig. 2011;15:357–60.
Lorenzoni DC, Cuzzuol Fracalossi AC, Carlin V, Ribeiro DA. Sant' Anna EF: Cytogenetic biomonitoring in children submitting to a complete set of radiographs for orthodontic planning. Angle Orthod. 2012;82:585–90.
Angelieri F, Carlin V, Saez DM, Pozzi R, Ribeiro DA. Mutagenicity and cytotoxicity assessment in patients undergoing orthodontic radiographs. Dentomaxillofac Radiol. 2010;39:437–40.
Calabrese EJ. Hormesis is central to toxicology, pharmacology and risk assessment. Hum Exp Toxicol. 2010;29:249–61.
Qian Q-Z, Cao X-K, Shen F-H, Wang Q. Effects of ionising radiation on micronucleus formation and chromosomal aberrations in Chinese radiation workers. Radiat Prot Dosimetry. 2016;168:197–203.
Han L, Zhao F-L, Sun Q-F, Wang P, Wang X-A, Guo F, et al. Cytogenetic analysis of peripheral blood lymphocytes, many years after exposure of workers to low-dose ionizing radiation. Mutat Res Genet Toxicol Environ Mutagen. 2014;771:1–5.
Lee T-K, Allison RR, O'Brien KF, Naves JL, Karlsson UL, Wiley AL Jr. Persistence of micronuclei in lymphocytes of cancer patients after radiotherapy. Radiat Res. 2002;157:678–84.
Cao J, Liu Y, Sun H, Cheng G, Pang X, Zhou Z. Chromosomal aberrations, DNA strand breaks and gene mutations in nasopharyngeal cancer patients undergoing radiation therapy. Mutat Res. 2002;504:85–90.
Lum A, Le Marchand L. A simple mouthwash method for obtaining genomic DNA in molecular epidemiological studies. Cancer Epidemiol Biomarkers Prev. 1998;7:719–24.
Garcia-Closas M, Egan KM, Abruzzo J, Newcomb PA, Titus-Ernstoff L, Franklin T, et al. Collection of genomic DNA from adults in epidemiological studies by buccal cytobrush and mouthwash. Cancer Epidemiol Biomarkers Prev. 2001;10:687–96.
Andrisin TE, Humma LM, Johnson JA. Collection of genomic DNA by the noninvasive mouthwash method for use in pharmacogenetic studies. Pharmacotherapy. 2002;22:954–60.
Walsh DJ, Corey AC, Cotton RW, Forman L, Herrin GL Jr, Word CJ, et al. Isolation of deoxyribonucleic acid (DNA) from saliva and forensic science samples containing saliva. J Forensic Sci. 1992;37:387–95.
Chang WP, Hsieh WA, Chen D-P, Lin Y-P, Hwang J-S, Hwang JJ, et al. Change in centromeric and acentromeric micronucleus frequencies in human populations after chronic radiation exposure. Mutagenesis. 1999;14:427–32.
Moore LE, Warner ML, Smith AH, Kalman D, Smith MT. Use of the fluorescent micronucleus assay to detect the genotoxic effects of radiation and arsenic exposure in exfoliated human epithelial cells. Environ Mol Mutagen. 1996;27:176–84.
Cerqueira EMM, Gomes-Filho IS, Trindade S, Lopes MA, Passos JS, Machado-Santelli GM. Genetic damage in exfoliated cells from oral mucosa of individuals exposed to X-rays during panoramic dental radiographies. Mutat Res. 2004;562:111–7.
Thomas P, Ramani P, Premkumar P, Natesan A, Sherlin HJ, Chandrasekar T. Micronuclei and other nuclear anomalies in buccal mucosa following exposure to X-ray radiation. Anal Quant Cytol Histol. 2012;34:161–9.
Oesterle SN, Finch SC: Bone marrow cytology in Hiroshima atomic bomb survivors 5 years following exposure. In RERF Technical Reports, vol. RERF TR 16–77. pp. 1-23. Hiroshima, Japan; 1978.
Carroll RJ, Ruppert D, Stefanski LA, Crainiceanu CM: Measurement error in nonlinear models. A modern perspective. pp. 1-488. Boca Raton, FL: Chapman and Hall/CRC; 2006:1–488.
Zhang Z, Preston DL, Sokolnikov M, Napier BA, Degteva M, Moroz B, et al. Correction of confidence intervals in excess relative risk models using Monte Carlo dosimetry systems with shared errors. PLoS One. 2017;12(4):e0174641.
Zhang C-Z, Spektor A, Cornils H, Francis JM, Jackson EK, Liu S, et al. Chromothripsis from DNA damage in micronuclei. Nature. 2015;522:179–84.
Morishita M, Muramatsu T, Suto Y, Hirai M, Konishi T, Hayashi S, et al. Chromothripsis-like chromosomal rearrangements induced by ionizing radiation using proton microbeam irradiation system. Oncotarget. 2016;7:10182-92.
Salaverria I, Martín-Garcia D, López C, Clot G, García-Aragonés M, Navarro A, et al. Detection of chromothripsis-like patterns with a custom array platform for chronic lymphocytic leukemia. Genes Chromosomes Cancer. 2015;54:668–80.
Tucker JD, Vadapalli M, Joiner MC, Ceppi M, Fenech M, Bonassi S. Estimating the lowest detectable dose of ionizing radiation by the cytokinesis-block micronucleus assay. Radiat Res. 2013;180:284–91.
Acknowledgements
Not applicable.
Ethical approval and consent to participate
The data were hosted at three collaborating institutions: National Research Center for Radiation Medicine, Kyiv, Ukraine, Columbia University/University of California San Francisco (UCSF), and the National Cancer Institute (NCI). All subjects signed an informed consent form, and the study was reviewed and approved by the institutional review boards of the participating institutions in both Ukraine and the United States. The data were de-identified before transfer to the United States participating institutions. The key to the data exists in Ukraine, but US researchers did not have access to it at any point.
Funding
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under contract NO1-CP-21178 and award number 5K07CA132918. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Additional support was provided by the Intramural Research Program of the National Institutes of Health, the National Cancer Institute, Division of Cancer Epidemiology and Genetics.
Availability of data and materials
The dataset and analysis files (including R [36] and Epicure [38] scripts) supporting the conclusions of this article is included within the article (and its additional file ‘Additional file 1.zip’).
Authors’ contributions
All authors of this research manuscript have directly participated in the planning, execution, or analysis of the study. The statistical analysis was conducted by MPL. Blood samples were collected and assayed, and associated interviews with the cleanup workers organized and conducted by DB, II, OL, ID, NT, NG. Dose estimates were made by VC. All authors participated in the writing of the manuscript.
Authors’ information
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
All authors of this manuscript agree to this submission to Environmental Health and agree with the content and presentation of the manuscript. It is not under consideration for publication elsewhere, its publication is approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and it will not be published elsewhere in the same form, in English or in any other language, including electronically without the written consent of the copyright-holder.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
Data files (Excel, text) and other R and Epicure files used in the analysis. (ZIP 3032 kb)
Appendices
Appendix 1
Appendix 2
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Bazyka, D., Finch, S.C., Ilienko, I.M. et al. Buccal mucosa micronuclei counts in relation to exposure to low dose-rate radiation from the Chornobyl nuclear accident and other medical and occupational radiation exposures. Environ Health 16, 70 (2017). https://doi.org/10.1186/s12940-017-0273-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12940-017-0273-x