
Abstract
Background
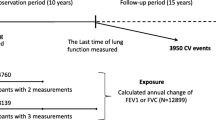
The potential effects of pulmonary dysfunction on cardiovascular diseases (CVD) are receiving attention. We aimed to investigate and quantify the cross-sectional and longitudinal associations between lung function and overall cardiovascular risk among Chinese general population.
Methods
We studied 4019 participants from the Wuhan-Zhuhai cohort, with a follow-up of 3 years. A multivariable risk algorithm generated from the Framingham study was used to calculate individuals’ overall cardiovascular risk i.e. 10-Year CVD Risk, which was further classified into 2 categories: low (< 10%) and high (≥10%) CVD risk. General linear model and logistic regression model were separately used to assess the associations of lung function with continuous and dichotomous 10-Year CVD Risk.
Results
Cross-sectionally, each 5% decrease in FEV1/FVC was associated with a 0.47% increase in 10-Year CVD Risk (P < 0.001). The adjusted odds ratio (OR) (95% confidence interval [CI]) for the prevalence of high CVD risk (10-Year CVD Risk≥10%) was 1.12 (1.07, 1.17) corresponding to each 5% decrease in FEV1/FVC. The OR (95% CI) for high CVD risk in the lowest group of FEV1/FVC (< 70% i.e. chronic obstructive pulmonary disease [COPD]) was 2.37 (1.43, 3.91) when compared with the highest group. Longitudinally, the adjusted risk ratio (RR) (95% CI) for the incidence of high CVD risk was 1.14 (1.03, 1.25) with each 5% decrease in baseline FEV1/FVC. Compared with the highest group of FEV1/FVC, the RR (95% CI) for high CVD risk in the lowest group (COPD) was 4.06 (1.46, 11.26). Analyses of 10-Year CVD Risk with FVC or FEV1 showed similar trends and significant associations (all P < 0.05).
Conclusion
Reduced lung function was cross-sectionally and longitudinally associated with increased cardiovascular risk in Chinese general population.
Similar content being viewed by others
Background
Cardiovascular diseases (CVD), including coronary disease, cerebrovascular disease, peripheral vascular disease and cardiac failure, are leading causes of morbidity and mortality in China and worldwide [1, 2]. To better prevent and control CVD, a global multivariable risk algorithm based on traditional CVD risk factors including sex, age, total and high density lipoprotein (HDL) cholesterol, systolic blood pressure and treatment for hypertension, smoking and diabetes status, was generated from the Framingham study [3]. The model has been demonstrated to have good discrimination power and be able to estimate overall CVD risk in the next ten years (10-Year CVD Risk) for individuals without CVD [3]. The 10-Year CVD Risk provides useful and elegant composite measures of the classical risk factors for CVD and reflects overall cardiovascular risk of individuals, thus it has been well recognized and widely used in fields of clinic and public health [3,4,5].
It is well known that cardiovascular and respiratory systems are closely linked with each other in physiology and pathophysiology. Cardiovascular dysfunction could affect lung function, in turn, pulmonary dysfunction may cause adverse cardiovascular outcomes [6, 7]. Pulmonary function, a noninvasive clinical diagnostic parameter, is often used to evaluate the conditions of the respiratory system and identify the severity of pulmonary impairments such as asthma and chronic obstructive pulmonary disease (COPD) [8]. Accumulating evidence suggested that pulmonary dysfunction was positively and independently associated with CVD morbidity [9,10,11,12,13,14,15] and mortality [16,17,18,19,20]. A cross-sectional study conducted among 9688 Korean general population without obstructive lung disease found that forced vital capacity (FVC) was inversely related to 10-Year CVD Risk [21]. However, it is still largely unknown whether the reduction of lung function parameters like forced expiratory volume in 1 s (FEV1) and the ratio of FEV1 to FVC (FEV1/FVC) are related to current and future CVD risk such as 10-Year CVD Risk. Further analysis on their associations in both cross-sectional and longitudinal ways will help better clarify and understand the potential effect of lung function decline on CVD.
Therefore, in present study, we investigated and quantified the cross-sectional and longitudinal associations between lung function (including parameters of FEV1, FVC and FEV1/FVC) and the 10-Year CVD Risk in a Chinese general population.
Methods
Study population
The study participants were from the Wuhan-Zhuhai cohort, a Chinese community-based prospective cohort, which has been described previously [22]. Briefly, the cohort was established between 2011 and 2012, comprising 4812 participants aged 18 to 80 years who lived in Wuhan or Zhuhai city in China for more than 5 years. Standardized questionnaires and extensive physical examinations were carried out at baseline and 3 years later. For cross-sectional analysis, participants less than 30 years old (n = 260) or previously diagnosed with CVD (n = 317) were excluded, as 10-Year CVD Risk estimation was inapplicable for this population [3]. We also excluded 216 subjects with missing data or outliers (>mean ± 3SD) on indexes of blood test, anthropometry, blood pressure or pulmonary function. Finally, a total of 4019 participants were included in our cross-sectional study. For longitudinal analysis, we further excluded 2196 individuals who did not attend physical examinations, or had missing data or outliers on indexes of blood test, anthropometry or blood pressure at 3-year follow-up. After further excluding 752 participants with 10-Year CVD Risk ≥10% at baseline, 1071 subjects were included in our longitudinal study. Individuals included and excluded in our study showed no differences with respect to basic demographic characteristics such as sex, body mass index, smoking status, drinking status, education levels, abdominal obesity, etc. (P > 0.05).
Lung function test
Lung function test was performed in accordance with the recommendation of American Thoracic Society [23]. In brief, spirometry was conducted by specialists using digital spirometers (Chestgraph HI-101, CHEST Ltd., Tokyo, Japan), which were calibrated each day before testing, according to the manufacturer’s instruction. All individuals were suggested not to smoke for at least 1 h and not to have a big meal for 2 h before the test. Each participant was informed to keep a sitting position, wear a nose clip, and then breathe through the mouth-piece after at least 5 min of normal breathing during the testing procedure. Three acceptable volume-time curves of pulmonary function parameters were obtained after three satisfactory blows of each participant performed. Lung function parameters including FVC, FEV1 and FEV1/FVC were mainly used in our study. COPD was defined as FEV1/FVC < 70%, which was further classified into four stages according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) [24]: GOLD 1 (mild: FEV1/FVC < 70% and FEV1 ≥ 80% predicted), GOLD 2 (moderate: FEV1/FVC < 70% and 50% ≤ FEV1 < 80% predicted), GOLD 3 (severe: FEV1/FVC < 70% and 30% ≤ FEV1 < 50% predicted) and GOLD 4 (very severe: FEV1/FVC < 70% and FEV1 < 30% predicted).
Ten-year CVD risk calculation and classification
Sex-specific 10-Year CVD Risk was calculated by a multivariable risk factor algorithm that incorporated age, total cholesterol, HDL cholesterol, systolic blood pressure and treatment for hypertension, current smoking, and diabetes status, as described previously [3]. According to the Framingham study [3] and Framingham database derived practice guideline [25], 10-Year CVD Risk was further classified into 2 categories: low (< 10%) and high (≥10%) CVD risk.
Ascertainment of covariates and CVD risk factors
Body mass index (BMI) was calculated by dividing weight (kg) by the squared value of height (m). Active physical activity was defined as regular exercise ≥2 times per week and each time ≥ 20 min within the last 6 months. Education degree was classified into 3 levels: middle school or below, high school, and university or above. Smokers comprised both current and former smokers, and smoking amount (pack-years) for each smoker was computed as packs of cigarettes per day multiplied by years of smoking. Participants were divided into drinkers (including current and former drinkers) and nondrinkers. Abdominal obesity was defined as waist circumference ≥ 90 cm for men or ≥ 80 cm for women. Blood lipids and fasting glucose levels were determined in the clinical laboratory of hospitals. Blood pressure was measured on the right arm of the seated participant with a validated automatic oscillometric device. Diabetes was defined as fasting plasma glucose ≥7.0 mmol/L, or taking oral hypoglycemic medication or insulin, or self-reported physician-diagnosed diabetes.
Statistical analyses
Subjects were divided into four groups based on quartiles (Q) of FVC or FEV1 or clinical thresholds of FEV1/FVC level (L1 < 70%; L2 70% ~ < 80%; L3 80% ~ < 90%; L4 ≥ 90%), for which 70% is a clinical threshold of COPD diagnosis and 80% is a critical value of normal lung function. Baseline characteristics across groups of FEV1/FVC were compared by variance analysis for continuous variables and Cochran-Armitage trend test for dichotomous variables. Analysis of covariance was used to compare 10-Year CVD Risk by groups of lung function parameters, with adjusting for gender, height, weight, abdominal obesity, smoking amount, drinking status, low density lipoprotein (LDL), physical activity, city and education levels. Age was not included in the statistic models for adjustment again, because as a dependent variable, 10-Year CVD Risk was estimated by a multivariable risk factor algorithm where age has been included, further adjustment for age in the statistic models again will lead to overcorrection and conservative association between lung function and CVD risk.
Association of lung function with continuous 10-Year CVD Risk was assessed using general linear model, with adjustment for potential confounders as mentioned above. The association was quantified by using estimated changes and 95% confidence intervals (CIs) of 10-Year CVD Risk with each 5% decrease of FEV1/FVC or each 50-mL decrease of FVC or FEV1 in continuous analyses. We also estimated changes (95% CI) of 10-Year CVD Risk across groups of lung function parameters in categorical analyses with the highest group (L4 or Q4) as the reference.
Logistic regression model was used to calculate the odds ratios (ORs), risk ratios (RRs) and 95% CI for dichotomous 10-Year CVD Risk (individuals with 10-Year CVD Risk ≥10% were regarded as cases) according to the decreasing of baseline lung function level, with adjusting for potential covariates as mentioned above. All statistical analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC), and all p-values were two sided with a significant level at 0.05.
Results
Baseline characteristics
The baseline characteristics of the participants based on groups of FEV1/FVC are presented in Table 1. The mean age of 4019 participants (1304 men; 32.45%) was 53.98 years. Without adjustment for any confounder, the number of smokers, drinkers and participants with high 10-Year CVD Risk (≥10%), as well as age, smoking amount, low density lipoprotein and 10-Year CVD Risk significantly increased across decreasing FEV1/FVC groups (P < 0.001). In further analysis with COPD patients (group L1: FEV1/FVC < 70%), we found an upward trend of 10-Year CVD Risk as the progresses of COPD (from GOLD 1 to GOLD 4, P trend = 0.041) (Table S1). And COPD patients with older age, male sex, smoking or drinking habits achieved higher CVD risk (P < 0.05) (Additional file 1: Table S1).
Association of pulmonary function with 10-year CVD risk
With adjustment for potential covariates, leastsquares means of 10-Year CVD Risk by groups of lung function parameters at baseline are shown in Fig. 1. The highest 10-Year CVD Risk was observed in the lowest group of lung function parameters (L1 [COPD group] or Q1) when compared with those in other groups. Upward trend of 10-Year CVD Risk was significantly associated with decreased lung function groups.

The 10-Year CVD Risk in all participants by groups of lung function parameters using analysis of covariance. Abbreviations: FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; FEV1/FVC, the ratio of FEV1 to FVC. * Significant differences between L4/Q4 and any other lung function group at P < 0.05; # significant differences between L3/Q3 and any other lung function group at P < 0.05; § significant differences between L2/Q2 and any other lung function group at P < 0.05. Adjusted for gender (male/female), height (continuous, m), weight (continuous, kg), abdominal obesity (yes/no), smoking amount (continuous, pack-year), drinking status (drinker/nondrinker), low density lipoprotein (continuous, mmol/L), physical activity (active/inactive), city (Wuhan/Zhuhai) and education levels (middle school or below, high school, university or above)
Table 2 presents an inverse relationship between lung function and continuous 10-Year CVD Risk at baseline. After adjusting for potential confounders, each 5% decrease in FEV1/FVC was associated with a 0.47% increase in 10-Year CVD Risk (P < 0.001). Remarkably monotonic increase of 10-Year CVD Risk was shown when FEV1/FVC gradually decreased (P trend < 0.001). Similar trends and significant associations were also observed between FVC and FEV1 and 10-Year CVD Risk (Table 2).
Table 3 shows a negative association between lung function and dichotomous10-Year CVD Risk at baseline. After adjusting for potential confounders, the OR (95%CI) for the prevalence of high CVD risk (10-Year CVD Risk ≥10%) was 1.12 (1.07, 1.17) with each 5% decrease in FEV1/FVC. Compared with the highest FEV1/FVC group, multi-variate adjusted ORs (95%CI) gradually increased when lung function decreased. From the second highest to the lowest FEV1/FVC group (COPD), they were 1.11 (0.94, 1.31), 1.63 (1.31, 2.03), 2.37 (1.43, 3.91) for high CVD risk. Similar trends and significant relationships were also shown between FVC and FEV1 and 10-Year CVD Risk (Table 3).
After 3 years of follow-up, we recalculated the 10-Year CVD Risk for the 1071 participants included in our longitudinal study, and 214 incident cases of high CVD risk (10-Year CVD Risk ≥10%) were identified. RRs for the incidence of high CVD risk are shown in Table 4. A negative association between baseline lung function and incidence of high CVD risk was observed. The RR (95%CI) was 1.14 (1.03, 1.25) corresponding to each 5% decline in FEV1/FVC. The categorical analysis also showed a significant monotonic RR increase of high CVD risk as the decreasing of FEV1/FVC groups (P trend = 0.021). Compared with the highest FEV1/FVC group, the RRs (95%CI) for high CVD risk were 1.15 (0.80, 1.65), 1.41 (0.85, 2.34), 4.06 (1.46, 11.26) from the second highest to the lowest FEV1/FVC group (COPD). Similarly, significant negative associations of FVC and FEV1 with 10-Year CVD Risk were observed with all P and P trend < 0.001 (Table 4).
Discussion
In the present study, negative cross-sectional and longitudinal associations were identified between lung function and 10-Year CVD Risk. After adjusting for potential confounders, increased prevalence and incidence of high CVD risk (10-Year CVD Risk ≥10%) were observed with the decline of lung function level. Additionally, when 10-Year CVD Risk was further classified into ≥6%/< 6% or > 20%/≤ 20% as also proposed by the Framingham study [3] and practice guideline derived from Framingham database [25], similar trends and significant associations with lung function were also found (data not shown). Our findings help to understand the correlation between lung function and current and future CVD risk. They also have significant implications for public health. Lung function test is a noninvasive clinical diagnostic method and is easy taken after routing training. The significant relationship between reduced lung function and increased CVD risk in ten years indicated that improving lung function or preventing lung function decline may help to prevent CVD.
Lung function has been linked to CVD risk in previous studies [21, 26, 27]. The 4th Korea National Health and Nutrition Examination Survey found that FVC decline was cross-sectionally associated with increased 10-Year CVD Risk [21]. Similarly, a study by Arcari et al. on Italian general population showed that FVC or FEV1 reduction was cross-sectionally associated with elevated 10-Year CVD Risk [27]. However, they did not find the association between FEV1/FVC, a mainly clinical diagnostic indicator for obstructive lung diseases such as COPD, and 10-Year CVD Risk, which is inconsistent with our findings. In our study, we found that not only FVC and FEV1 but also FEV1/FVC reduction was cross-sectionally and longitudinally associated with increased10-Year CVD Risk. Such discrepancy between our study and the published data may be partly due to the differences in race, genetics and lifestyles of the study population. For example, as a common risk factor for CVD, cigarette smoking rate was 22.05% in our study, lower than the mean smoking rate (28.10%) for adults in China [28]. Physical activity rate, a protective factor of CVD, was 48.94% in our study, much higher than the average level (11.90%) of Chinese adults [29]. These factors may lead to more obvious effect of lung function decline on CVD. Additionally, compared with the participants in our study (average BMI: 24.05 kg/m2), the subjects included in Arcari’s study had higher BMI with a mean value of 27.6 kg/m2, which was considered as overweight and on the brink of obesity [30]. As risk factors for CVD [25, 31], overweight and obesity may partly conceal the effects of FEV1/FVC on the risk of CVD in Arcari’s study.
Furtherly, we noted that participants with COPD (FEV1/FVC < 70%) achieved the highest 10-Year CVD Risk in our present study. This result is consistent with those reported by Ford and colleagues. They found that aged adults with obstructive or restrictive impairment had an increased 10-Year CVD Risk compared with those with normal lung function [26]. Besides, accumulating evidence suggested that COPD patients have an elevated risk of CVD and cardiovascular death, and nearly two fifths of COPD patients die of CVD [17, 18, 32].
The underlying mechanisms between pulmonary dysfunction and CVD remain incompletely understood. Generally, pulmonary and cardiovascular functions are closely related in both physiological and pathological conditions. At the circumstance of lung function decline, cardiac pumping function has to increase compensatorily to ensure the body’s oxygen need, which may result in cardiac and vascular overloads, and even cardiovascular injuries [33, 34]. If these situations were not improved timely, cardiovascular events might occur in the near future [33]. Additionally, shared risk factors may partly explain the association between poor lung function and elevated CVD risk [7]. It is well documented that several risk factors for lung function reduction, such as aging and smoking, are also well-established risk factors for CVD [3]. And traditional cardiovascular risk factors such as hypertension, dyslipidemia and diabetes mellitus are common in subjects with lung function impairment including COPD [35]. Air pollutants like particulate matters and polycyclic aromatic hydrocarbons are notable risk factors for both poor lung function and cardiovascular events [36,37,38]. However, the still observed association between lung function and CVD after adjusting for shared risk factors suggested the involvement of additional explanations [20].
Further explanations could be inflammation and oxidative stress, which were reported to have important contributions to both lung function decline and CVD risk increase [7]. Evidence has shown that inflammation markers such as C-reactive protein, fibrinogen and inflammation-sensitive plasma proteins were involved in the inverse relationship between lung function and CVD risk [20, 21, 39]. As a major driving mechanism in the pathophysiology of lung function impairment, elevated oxidative stress in local pulmonary microenvironment may directly affect cardiovascular system [7]. Previous studies suggested that oxidative stress may cause vascular dysfunction through inactivating the endothelial-derived nitric oxide by superoxide anion [40]. Generation of reactive oxygen species (ROS) could promote inflammation in the vascular wall by inducing the production of pro-inflammatory genes and cytokines via the activation of NF-κB [41], whereas in turn, inflammatory cytokines (TNF-α, IL-6, etc.) could increase ROS production by NADPH oxidases [42, 43], causing a vicious circle that exacerbates vascular dysfunction [44]. Moreover, oxidative stress and inflammation could also alter the vascular structure by promoting vascular remodeling, stiffness and atherosclerosis [44,45,46]. Therefore, the inflammation and increased oxidative stress in pulmonary dysfunction may independently increase CVD risk by altering vascular structure and promoting vascular dysfunction and insufficiency [7]. Besides, evidence has shown that pulmonary dysfunction specific inflammation and oxidative stress may elevate cardiovascular risk also through increasing susceptibility to thrombotic or embolic events [47,48,49].
The strengths of our study include a relative large study population and a 3-year follow-up. Based on that, we could investigate the cross-sectional relationship between lung function and CVD risk and longitudinally evaluate the changes after 3 years. And to our knowledge, it is the first prospective study to investigate the relationship between lung function and 10-Year CVD Risk. However, there are still several limitations. First, rather than clinically diagnosed CVD, we evaluated the risk of CVD using a global multivariable risk algorithm, which was clinically used to estimate the 10-Year CVD Risk of individuals. Nevertheless, as an available endpoint, 10-Year CVD Risk do provide useful and elegant composite measures of the classical risk factors for CVD and represent individuals’ overall cardiovascular risk. Moreover, we are not unique in using 10-Year CVD Risk as a composite measure of CVD risk (endpoint), and a similar method was also taken by studies draw from Cardiovascular Risk Factor Multiple Evaluation in Latin America Study [50], Louisville Healthy Heart Study [51], Lifestyle Interventions and Independence for Elders Study [52], International Mobility in Aging Study [53], etc. Second, the CVD risk was merely estimated at baseline and at 3 years of follow-up, and the follow-up time may be relatively short. Further long-time longitudinal study may help to accurately evaluate such relationship.
Conclusions
Our study clearly demonstrated that reduced lung function was cross-sectionally and longitudinally associated with increased CVD risk in a general Chinese population. It suggests that improve lung function or prevent lung function decline may help to prevent CVD. Further studies with long-time follow-up are needed to validate our findings and illuminate the potential mechanisms.
Abbreviations
- BMI:
-
body mass index
- CI:
-
confidence interval
- COPD:
-
chronic obstructive pulmonary disease
- CVD:
-
cardiovascular diseases
- FEV1 :
-
forced expiratory volume in 1 s
- FEV1/ FVC:
-
the ratio of FEV1 to FVC
- FVC:
-
forced vital capacity
- GOLD:
-
global initiative for chronic obstructive lung disease
- HDL:
-
high density lipoprotein
- IL-6:
-
Interleukin-6
- LDL:
-
low density lipoprotein
- NADPH:
-
Nicotinamide adenine dinucleotide phosphate
- NF-κB:
-
nuclear factor kappa B
- OR:
-
odds ratio
- ROS:
-
reactive oxygen species
- RR:
-
risk ratio
- TNF-α:
-
tumour necrosis factor alpha
References
He J, Gu D, Wu X, Reynolds K, Duan X, Yao C, Wang J, Chen CS, Chen J, Wildman RP, et al. Major causes of death among men and women in China. N Engl J Med. 2005;353:1124–34.
Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367:1747–57.
D'Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, Kannel WB. General cardiovascular risk profile for use in primary care: the Framingham heart study. Circulation. 2008;117:743–53.
Grundy SM, Pasternak R, Greenland P, Smith S Jr, Fuster V. Assessment of cardiovascular risk by use of multiple-risk-factor assessment equations: a statement for healthcare professionals from the American Heart Association and the American College of Cardiology. Circulation. 1999;100:1481–92.
Park KH, Kim MK, Kim HS, Park WJ, Cho GY, Choi YJ. Clinical significance of Framingham risk score, flow-mediated dilation and pulse wave velocity in patients with stable angina. Circ J. 2011;75:1177–83.
Burroughs Pena MS, Dunning A, Schulte PJ, Durheim MT, Kussin P, Checkley W, Velazquez EJ. Pulmonary function and adverse cardiovascular outcomes: can cardiac function explain the link? Respir Med. 2016;121:4–12.
Austin V, Crack PJ, Bozinovski S, Miller AA, Vlahos R. COPD and stroke: are systemic inflammation and oxidative stress the missing links? Clin Sci (Lond). 2016;130:1039–50.
Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, Celli BR, Chen R, Decramer M, Fabbri LM, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195:557–82.
Iribarren C, Tolstykh IV, Eisner MD. Are patients with asthma at increased risk of coronary heart disease? Int J Epidemiol. 2004;33:743–8.
Engstrom G, Melander O, Hedblad B. Population-based study of lung function and incidence of heart failure hospitalisations. Thorax. 2010;65:633–8.
Georgiopoulou VV, Kalogeropoulos AP, Psaty BM, Rodondi N, Bauer DC, Butler AB, Koster A, Smith AL, Harris TB, Newman AB, et al. Lung function and risk for heart failure among older adults: the health ABC study. Am J Med. 2011;124:334–41.
Agarwal SK, Heiss G, Barr RG, Chang PP, Loehr LR, Chambless LE, Shahar E, Kitzman DW, Rosamond WD. Airflow obstruction, lung function, and risk of incident heart failure: the atherosclerosis risk in communities (ARIC) study. Eur J Heart Fail. 2012;14:414–22.
Soderholm M, Zia E, Hedblad B, Engstrom G. Lung function as a risk factor for subarachnoid hemorrhage: a prospective cohort study. Stroke. 2012;43:2598–603.
Johnston AK, Mannino DM, Hagan GW, Davis KJ, Kiri VA. Relationship between lung function impairment and incidence or recurrence of cardiovascular events in a middle-aged cohort. Thorax. 2008;63:599–605.
Lee HM, Liu MA, Barrett-Connor E, Wong ND. Association of lung function with coronary heart disease and cardiovascular disease outcomes in elderly: the rancho Bernardo study. Respir Med. 2014;108:1779–85.
Schunemann HJ, Dorn J, Grant BJ, Winkelstein W Jr, Trevisan M. Pulmonary function is a long-term predictor of mortality in the general population: 29-year follow-up of the Buffalo health study. Chest. 2000;118:656–64.
Sin DD, Man SF. Chronic obstructive pulmonary disease as a risk factor for cardiovascular morbidity and mortality. Proc Am Thorac Soc. 2005;2:8–11.
Sin DD, Wu L, Man SF. The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest. 2005;127:1952–9.
Engstrom G, Hedblad B, Janzon L. Reduced lung function predicts increased fatality in future cardiac events. A population-based study. J Intern Med. 2006;260:560–7.
Min KB, Min JY. Reduced lung function, C-reactive protein, and increased risk of cardiovascular mortality. Circ J. 2014;78:2309–16.
Kang HK, Park HY, Jeong BH, Koh WJ, Lim SY. Relationship between forced vital capacity and Framingham cardiovascular risk score beyond the presence of metabolic syndrome: the fourth Korea National Health and nutrition examination survey. Medicine (Baltimore). 2015;94:e2089.
Song Y, Hou J, Huang X, Zhang X, Tan A, Rong Y, Sun H, Zhou Y, Cui X, Yang Y, et al. The Wuhan-Zhuhai (WHZH) cohort study of environmental air particulate matter and the pathogenesis of cardiopulmonary diseases: study design, methods and baseline characteristics of the cohort. BMC Public Health. 2014;14:994.
Standardization of Spirometry, Update. American Thoracic Society. Am J Respir Crit Care Med. 1995(152):1107–36.
Tan WC, Bourbeau J, Aaron SD, Zhou G, Maltais F, Hernandez P, Fitzgerald JM, Marciniuk DD, Walker BL, Sin DD. Global initiative for chronic obstructive lung disease 2017 classification and lung function decline in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197:670–3.
National Cholesterol Education Program Expert Panel on Detection E, treatment of high blood cholesterol in a. third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circulation. 2002;106:3143–421.
Ford ES, Wheaton AG, Mannino DM, Presley-Cantrell L, Li C, Croft JB. Elevated cardiovascular risk among adults with obstructive and restrictive airway functioning in the United States: a cross-sectional study of the National Health and nutrition examination survey from 2007-2010. Respir Res. 2012;13:115.
Arcari A, Magnacca S, Bracone F, Costanzo S, Persichillo M, Di Castelnuovo A, de Curtis A, Zito F, Schunemann HJ, Donati MB, et al. Relation between pulmonary function and 10-year risk for cardiovascular disease among healthy men and women in Italy: the Moli-sani project. Eur J Prev Cardiol. 2013;20:862–71.
Li Q, Hsia J, Yang G. Prevalence of smoking in China in 2010. N Engl J Med. 2011;364:2469–70.
Zhang N, Du SM, Ma GS. Current lifestyle factors that increase risk of T2DM in China. Eur J Clin Nutr. 2017;71:832–8.
Loinard C, Ginouvès A, Vilar J, Cochain C, Zouggari Y, Recalde A, Duriez M, Lévy BI, Pouysségur J, Berra E. Clinical guidelines: identification, evaluation, and treatment of overweight and obesity in adults - statistical data included. Circulation. 2009;120:50–9.
Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham heart study. Circulation. 1983;67:968–77.
Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33:1165–85.
Wilkins MR, Ghofrani HA, Weissmann N, Aldashev A, Zhao L. Pathophysiology and treatment of high-altitude pulmonary vascular disease. Circulation. 2015;131:582–90.
Mcphee SJ, Hammer GD. Pathophysiology of disease an introduction to clinical medicine, sixth edition. Maidenhead: Open University Press; 2010.
Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32:962–9.
Zhou Y, Sun H, Xie J, Song Y, Liu Y, Huang X, Zhou T, Rong Y, Wu T, Yuan J, Chen W. Urinary polycyclic aromatic hydrocarbon metabolites and altered lung function in Wuhan, China. Am J Respir Crit Care Med. 2016;193:835–46.
Hu C, Hou J, Zhou Y, Sun H, Yin W, Zhang Y, Wang X, Wang G, Chen W, Yuan J. Association of polycyclic aromatic hydrocarbons exposure with atherosclerotic cardiovascular disease risk: a role of mean platelet volume or club cell secretory protein. Environ Pollut. 2017;233:45–53.
Pinault LL, Weichenthal S, Crouse DL, Brauer M, Erickson A, Donkelaar AV, Martin RV, Hystad P, Chen H, Fines P, et al. Associations between fine particulate matter and mortality in the 2001 Canadian census health and environment cohort. Environ Res. 2017;159:406–15.
Engstrom G, Lind P, Hedblad B, Wollmer P, Stavenow L, Janzon L, Lindgarde F. Lung function and cardiovascular risk: relationship with inflammation-sensitive plasma proteins. Circulation. 2002;106:2555–60.
Miller AA, Budzyn K, Sobey CG. Vascular dysfunction in cerebrovascular disease: mechanisms and therapeutic intervention. Clin Sci (Lond). 2010;119:1–17.
Marchesi C, Paradis P, Schiffrin EL. Role of the renin-angiotensin system in vascular inflammation. Trends Pharmacol Sci. 2008;29:367–74.
Basuroy S, Bhattacharya S, Leffler CW, Parfenova H. Nox4 NADPH oxidase mediates oxidative stress and apoptosis caused by TNF-alpha in cerebral vascular endothelial cells. Am J Physiol Cell Physiol. 2009;296:C422–32.
Schrader LI, Kinzenbaw DA, Johnson AW, Faraci FM, Didion SP. IL-6 deficiency protects against angiotensin II induced endothelial dysfunction and hypertrophy. Arterioscler Thromb Vasc Biol. 2007;27:2576–81.
Moskowitz MA, Lo EH, Iadecola C. The science of stroke: mechanisms in search of treatments. Neuron. 2010;67:181–98.
Husain K, Hernandez W, Ansari RA, Ferder L. Inflammation, oxidative stress and renin angiotensin system in atherosclerosis. World J Biol Chem. 2015;6:209–17.
Faraci FM. Protecting against vascular disease in brain. Am J Physiol Heart Circ Physiol. 2011;300:H1566–82.
Maclay JD, McAllister DA, Johnston S, Raftis J, McGuinnes C, Deans A, Newby DE, Mills NL, MacNee W. Increased platelet activation in patients with stable and acute exacerbation of COPD. Thorax. 2011;66:769–74.
Tohgi H, Konno S, Takahashi S, Koizumi D, Kondo R, Takahashi H. Activated coagulation/fibrinolysis system and platelet function in acute thrombotic stroke patients with increased C-reactive protein levels. Thromb Res. 2000;100:373–9.
Dayal S, Wilson KM, Motto DG, Miller FJ Jr, Chauhan AK, Lentz SR. Hydrogen peroxide promotes aging-related platelet hyperactivation and thrombosis. Circulation. 2013;127:1308–16.
Schargrodsky H, Hernandez-Hernandez R, Champagne BM, Silva H, Vinueza R, Silva Aycaguer LC, Touboul PJ, Boissonnet CP, Escobedo J, Pellegrini F, et al. CARMELA: assessment of cardiovascular risk in seven Latin American cities. Am J Med. 2008;121:58–65.
DeJarnett N, Conklin DJ, Riggs DW, Myers JA, O'Toole TE, Hamzeh I, Wagner S, Chugh A, Ramos KS, Srivastava S, et al. Acrolein exposure is associated with increased cardiovascular disease risk. J Am Heart Assoc. 2014;3:1–11.
Fitzgerald JD, Johnson L, Hire DG, Ambrosius WT, Anton SD, Dodson JA, Marsh AP, McDermott MM, Nocera JR, Tudor-Locke C, et al. Association of objectively measured physical activity with cardiovascular risk in mobility-limited older adults. J Am Heart Assoc. 2015;4:1–9.
Rosendaal NTA, Alvarado B, Wu YY, Velez MP, da Camara SMA, Pirkle CM. Adolescent childbirth is associated with greater Framingham risk scores for cardiovascular disease among participants of the IMIAS (international mobility in aging study). J Am Heart Assoc. 2017;6:1–13.
Acknowledgments
All volunteers who participated in this study and all members of the study team are greatly acknowledged.
Funding
This study was supported by National Key Research and Development Program (2016YFC1303903 and 2016YFC0901101); Key Program of the National Natural Science Foundation of China (91543207); Fundamental Research Funds for the Central Universities, HUST (2016YXZD044 and 2016JCTD116).
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
WC was responsible for the design of the Wuhan-Zhuhai cohort study and funding obtaining. BW, YZ and WC conceived and designed this study. BW and YZ performed statistical analyses. BW interpreted the data and drafted the manuscript. All authors contributed to the data collection, manuscript revision, important intellectual content and final version approval. WC has full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants enrolled provided written informed consent for participation. The study protocol was approved by the Ethics and Human Subject Committee of Tongji Medical College, Huazhong University of Science and Technology. The methods were carried out in accordance with the approved guidelines.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. Ten-Year CVD Risk by GOLD classification and selected baseline characteristics in COPD patients (N = 101). (DOCX 17 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wang, B., Zhou, Y., Xiao, L. et al. Association of lung function with cardiovascular risk: a cohort study. Respir Res 19, 214 (2018). https://doi.org/10.1186/s12931-018-0920-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-018-0920-y