
Abstract
Background
Lipids such as cholesterol and triglycerides play an important role in both maternal and foetal energy metabolism. Little is known about maternal lipid levels in pregnancy and their effect on foetal growth. The aim of this study was to assess maternal lipid levels, foetal growth and the risk of small-for-gestational age (SGA) and large-for-gestational age (LGA).
Methods
We included 5702 women from the Generation R Study, a prospective population-based cohort. Maternal lipid levels (total cholesterol, triglycerides and high-density lipoprotein cholesterol [HDL-c]) were measured in early pregnancy (median 13.4 weeks, 90% range [10.5 to 17.2]). Low-density lipoprotein cholesterol (LDL-c), remnant cholesterol and non-HDL-c were calculated. Foetal growth was measured repeatedly by ultrasound. Information on birth anthropometrics was retrieved from medical records. A birth weight below the 10th percentile was defined as SGA and above the 90th percentile as LGA.
Results
Maternal triglyceride and remnant cholesterol levels were associated with increased foetal head circumference and abdominal circumference growth rates. Triglycerides and remnant cholesterol were positively associated with the risk of LGA (odds ratio [OR] 1.11, 95% confidence interval [CI] [1.01 to 1.22] and OR 1.11, 95% CI [1.01 to 1.23], respectively). These associations were independent of maternal pre-pregnancy body mass index, but not maternal glucose levels. We observed no association between maternal lipids in early pregnancy and SGA.
Conclusions
Our study suggests a novel association of early pregnancy triglyceride and remnant cholesterol levels with foetal growth, patterns of foetal growth and the risk of LGA. Future studies are warranted to explore clinical implication possibilities.
Similar content being viewed by others
Background
The worldwide incidence of overweight and obese women of reproductive age is increasing [1,2,3]. High maternal weight and hyperglycaemia are established risk factors for increased foetal growth and a child born large-for-gestational age (LGA). Maternal hyperglycaemia is associated with a higher flux of glucose over the placenta leading to foetal upregulation of insulin, increased foetal growth and ultimately a child born LGA [4,5,6,7,8,9,10].
Because the foetus has a limited capacity for de novo lipogenesis and fatty acid oxidation, it is dependent on maternal triglycerides as source for growth and development [11, 12]. During pregnancy, maternal insulin resistance leads to decreased lipoprotein lipase (LPL) activity and hence 2–3-fold increased maternal triglyceride levels [7, 8, 13]. Maternal triglycerides in the form of both liver-derived very low-density lipoprotein (VLDL) and dietary chylomicrons must first be hydrolysed to free fatty acids (FFA) by placental lipases to allow uptake by the syncytiotrophoblast [13, 14]. There FFA can be stored, metabolized, oxidized or transported into the foetal circulation [13, 15]. Insufficient fatty acid oxidation has been linked to preterm birth and intrauterine growth restriction [16]. On the other hand, maternal triglycerides were shown to correlate more strongly than glucose with newborn percent fat [17, 18].
Adverse birth outcomes, including small-for-gestational age (SGA) and LGA, may affect short-term (e.g. increased morbidity and mortality) and long-term (increased risk of hypertension, diabetes and metabolic syndrome) health of the child [19,20,21].
Lipid levels in early pregnancy are associated with maternal pregnancy complications, such as pre-eclampsia, independent of pre-pregnancy body mass index (BMI) [22]. Our hypothesis is that according to the Developmental Origins of Health and Disease (DOHaD) theory, maternal lipid levels may also lead to adverse birth outcomes such as LGA due to adverse growth patterns [23]. Therefore, the aim of this study is to examine the association of maternal early pregnancy lipid levels with foetal growth, patterns of foetal growth and the risk of SGA and LGA independent of maternal BMI and glucose levels.
Methods
Study design
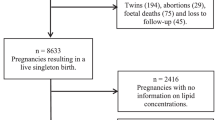
This study was embedded within the Generation R Study, an ongoing population-based prospective cohort study from early pregnancy onwards in Rotterdam, the Netherlands [24]. All pregnant women living in Rotterdam with an expected delivery date between April 2002 and January 2006 were eligible for participation. The study has been approved by the Medical Ethical Committee of the Erasmus Medical Centre Rotterdam, the Netherlands (MEC 198.782/2001/31). All procedures were in accordance with institutional guidelines, and written informed consent was obtained from all participants [25]. For the present study, we included 5702 women with a live born singleton and available information on lipid measurements in early pregnancy. We excluded women with a twin pregnancy, diabetes mellitus and gestational diabetes and those on lipid or glucose regulating treatment during study enrolment (Fig. 1). Gestational diabetes was diagnosed according to Dutch guidelines using the following criteria: either a random glucose level > 11.0 mmol/L, a fasting glucose level ≥ 7.0 mmol/L or a fasting glucose level between 6.1 and 6.9 mmol/L with a subsequent abnormal glucose tolerance test (glucose level > 7.8 mmol/L after glucose intake) [24]. Additional file 2 contains a Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for the current study [26].

Flowchart showing the inclusion and exclusion criteria
Exposure: maternal lipid levels in early pregnancy
Non-fasting plasma samples were obtained in early pregnancy (median 13.4 weeks of gestation, 90% range [10.5 to 17.2]). Total cholesterol (mmol/L), triglyceride (mmol/L) and high-density lipoprotein cholesterol (HDL-c) (mmol/L) concentrations were analysed. LDL-c (mmol/L), remnant cholesterol ([total cholesterol − LDL-c] − HDL-c) and non-HDL-c (total cholesterol − HDL-c) were calculated [22]. Sample processing, storage procedures and the changes in maternal lipid levels per gestational age in the same study population have been described previously [22, 27].
Outcome measures: foetal growth parameters and adverse birth outcomes
The primary outcome of this study was adverse birth outcomes. Secondary outcomes were foetal growth and foetal growth patterns. Ultrasound measurements were performed in mid-pregnancy (median 20.4 weeks of gestation, 90% range [19.1 to 22.5]) and late pregnancy (median 30.2 weeks of gestation, 90% range [29.1 to 31.9]) using protocols describing standardized planes [28,29,30]. Foetal growth parameters included the head circumference, femur length and abdominal circumference. We calculated the estimated foetal weight (EFW) using the Hadlock 3 formula [31]. Longitudinal growth curves and gestational-age-adjusted standard deviation scores (SDS) were constructed for all foetal growth parameters. These gestational-age-adjusted SDS were based on reference growth curves from the whole-study population and represent the equivalent of z-scores [30]. Information on birth anthropometrics (head circumference, length and weight) and gestational age at birth was obtained from medical files and midwife registries. Gestational-age-adjusted SDS for birth weight were constructed using North European growth standards as the reference growth curve and represent the equivalent of z-scores [32]. A birth weight below the 10th percentile, adjusted for gestational age and foetal sex, was defined as SGA and above the 90th percentile as LGA. All children with a birth weight above the 10th percentile and below the 90th percentile were considered average-for-gestational age (AGA).
Covariates
Potential confounders were identified based on the graphical criteria for confounding by visualizing a directed acyclic graph (DAG) (Additional file 1, Figure S1). Of these potential confounders, we included those in the models that changed the effect estimates > 10% for at least one of the outcomes [33]. Maternal questionnaires at study enrolment provided information on maternal age, parity, ethnicity, education, pre-pregnancy body mass index, smoking habits and folic acid supplementation. Pre-pregnancy BMI was highly correlated with BMI measured at study enrolment (Pearson’s correlation coefficient 0.95 [P value < .001]) [34], and therefore, pre-pregnancy BMI was used in the analyses. Non-fasting maternal glucose levels were measured in early pregnancy with the c702 module on a Cobas 8000 analyser as described previously [6, 27]. Women who experienced gestational hypertension and pre-eclampsia in their index pregnancy were classified as having a hypertensive disorder of pregnancy. All diagnoses were cross-validated retrospectively by obstetric records that were obtained from midwife and hospital registries [24, 35]. The criteria for hypertensive disorders of pregnancy were defined by the criteria that applied at the time of study inclusion of Generation R. This was according to the statement from the International Society for the Study of Hypertension in Pregnancy of 2001 [36]. Several overlapping sources (obstetric caregivers and Municipal Health Services) provided information on admission to the Neonatal Intensive Care Unit (NICU) [37].
Statistical analyses
Missing values of the covariates were imputed through multiple imputation procedures [38]. Data were imputed according to the Markov Chain Monte Carlo method. Data were analysed in each set separately, and pooled estimates from the five imputed datasets were used to report the effect estimates and their 95% confidence intervals. For the multiple imputation procedure, we performed 10 iterations [39]. In this study, 0% of women had missing information on maternal age at enrolment and gestational age at the time of blood sampling, 4.2% on ethnicity, 7.4% on educational level, 0.9% on parity, 10.4% on smoking habits, 23.2% on folic acid supplementation, 21.4% on pre-pregnancy BMI and 2.4% on early pregnancy maternal glucose levels. First, we examined baseline characteristics. Thereafter, we examined differences in maternal lipid profiles in women with a child born AGA compared to women with a child born SGA or LGA through a Student t test. Not normally distributed exposure measures were log transformed. To enable comparison of effect estimates, we constructed SD scores (SDS) of exposures. Multivariate linear regression analyses were performed to examine the associations of maternal lipid levels in early pregnancy with foetal growth parameters at birth. We performed multivariate logistic regression analyses to determine the association of lipid levels in early pregnancy with the risk of SGA and LGA. The basic regression model adjusted for maternal age at enrolment, gestational age at the time of blood sampling, parity, ethnicity, educational level, smoking habits and folic acid supplementation. The BMI model additionally adjusted for pre-pregnancy BMI. In a separate glucose model, we additionally adjusted for early pregnancy maternal glucose levels. To assess foetal growth patterns, we examined the associations between lipid levels in early pregnancy and repeatedly measured foetal growth parameters using unbalanced repeated measurement regression models with an unstructured covariance structure. These models take the correlation between repeated measurements of the same individual into account and allow for incomplete outcome data [40]. We included maternal early pregnancy lipid levels in these models as an intercept and as an interaction term with gestational age to estimate foetal growth rates over time [40]. The repeated analyses were conducted without adjustment for covariates, which most clearly reflects clinical practice. Since maternal lipid levels in early pregnancy are associated with pre-eclampsia and since hypertensive disorders of pregnancy are associated with adverse birth outcomes, we additionally performed a regression analysis of lipid levels in early pregnancy with the risk of SGA in LGA in a subgroup excluding women with gestational hypertension or pre-eclampsia in their index pregnancy.
To examine whether the association of early pregnancy lipid levels with adverse birth outcomes was explained by genetic factors and/or lifestyle factors as well, we performed logistic regression analyses in a subset of women including only nulliparous, non-smoking women with a pre-pregnancy BMI < 25 kg/m2. Comparison of women included and excluded in this study was conducted by comparing the characteristics of women included in this study (women with inclusion in early pregnancy, [n = 5702]) to women with inclusion in mid- or late pregnancy (n = 2151).
In all analyses, a P value < .05 was considered statistically significant. Statistical analyses were performed using the IBM Statistical Package for the Social Sciences version 24.0 for Windows (SPSS Incl., Chicago, IL, USA) and the Statistical Analysis System version 9.4 (SAS, Institute Inc., Cary, NC, USA).
Results
We included 5702 women. These women were on average 29.5 (± 5.1) years of age, mostly European (58.6%), and most women had a pre-pregnancy BMI < 25.0 kg/m2 (71.6%). Foetal growth parameters were available in 5499 (96.4%) and 5486 (96.2%) children in mid- and late pregnancy, respectively (Table 1). Of all children, 4526 were born AGA, 564 SGA and 565 LGA. Women with a child born LGA had higher levels of triglycerides and remnant cholesterol in early pregnancy than women with a child born AGA (Table 2). No differences were observed in lipid distribution between women with a child born SGA and AGA.
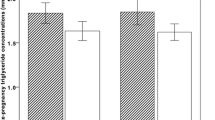
Figure 2 shows that triglycerides and remnant cholesterol were associated with increased foetal head circumference growth rates from late pregnancy onwards resulting in a higher head circumference at birth (0.6 SDS, 95% confidence interval [CI] [0.04 to 1.2] and 0.7 SDS, 95% CI [0.1 to 1.2], respectively) (Table 3). Additionally, triglycerides and remnant cholesterol were associated with increased foetal abdominal circumference growth rates from mid-pregnancy onwards (Fig. 2) resulting in a higher birth weight (18.4 SDS, 95% CI [6.5 to 30.3] and 18.7 SDS 95% CI [6.8 to 30.6], respectively) (Table 3). Maternal lipid levels in early pregnancy were not associated with foetal length and weight growth patterns (Fig. 2 and Table 3).

Differences in foetal growth rates per change in maternal early pregnancy lipid level.
Abbreviations: SDS, standard deviation score; CI, confidence interval; LDL-c, low-density lipoprotein cholesterol; HDL-c, high-density lipoprotein cholesterol. Estimates represent SDS values (95% CI) from repeated measurement regression models that reflect the differences in gestational age-adjusted growth rates in SDS of head circumference, length, weight and abdominal circumference at mid-pregnancy, late pregnancy and at birth per 1 SDS change in maternal early pregnancy lipid levels
Table 4 shows the association of maternal lipid concentrations in early pregnancy with adverse birth outcomes. Triglyceride and remnant cholesterol levels in early pregnancy were positively associated with the risk of LGA. The association of triglycerides and remnant cholesterol with LGA was attenuated when adjusting for pre-pregnancy BMI. However, after adjustment for glucose, the associations were not significant anymore. The negative association between HDL-c and LGA attenuated to non-significant levels after adjustment for pre-pregnancy BMI and early pregnancy maternal glucose levels. Total cholesterol, LDL-c and non-HDL-c were not associated with LGA. We observed no association between maternal lipid levels in early pregnancy and the risk of SGA.
In this study, 218 women had gestational hypertension and 139 women had pre-eclampsia in their index pregnancy. Excluding these women from the analysis, it shows that maternal lipid concentrations in early pregnancy are not associated with SGA and LGA (Additional file 1, Table S1).
Additional file 1, Table S2a, presents the lipid profile of 1915 nulliparous, non-smoking women with a BMI < 25 kg/m2. This more homogeneous subset of relatively healthy women had a less atherogenic lipid profile in early pregnancy, especially lower triglycerides, LDL-c, remnant cholesterol and higher levels of HDL-c than women in the total study population. In this subset of women, we found no association with adverse birth outcomes (Additional file 1, Table S2b).
Discussion
This study shows that maternal triglycerides and remnant cholesterol levels in early pregnancy are associated with increased foetal growth rates, specifically for head and abdominal circumference from mid-pregnancy onwards resulting in a higher head circumference at birth and a higher birth weight. Moreover, triglycerides and remnant cholesterol in early pregnancy are associated with a higher risk of being born LGA, independent of maternal BMI. However, these associations attenuated to non-significant levels after adjustment for early pregnancy maternal glucose levels.
The positive association of triglycerides and birth weight that we found is in line with previous studies examining the associations of maternal triglycerides in early, mid- and late pregnancy with birth weight and LGA [41,42,43,44]. A study of Vrijkotte et al. examined early pregnancy (median 13 weeks, interquartile range 12; 14 weeks) non-fasting total cholesterol and triglyceride levels in 2502 Dutch women [43]. Lipid levels were divided into quintiles, and women in the highest quintile had a mean triglyceride level of 2.15 (± 0.52) mmol/L. In our study, women had lower levels of triglycerides with a mean of 1.72 (± 0.54) mmol/L in the highest quintile. The study of Vrijkotte et al. found that the highest triglyceride quintile was associated with a higher birth weight and a higher prevalence of a child born LGA. However, a limitation of this study is that they did not take the influence of glucose into account, even though this is a well-known confounder for triglyceride levels [45, 46]. In our study, we corrected for both maternal BMI and early pregnancy glucose levels and showed that the positive association between triglycerides and LGA remained significant if maternal BMI was considered. However, after adjustment for glucose levels, the association attenuated to non-significant levels.
A study by Jin et al. measured lipid levels in 934 women during every trimester and, as expected, found that triglyceride levels increased from 2.2 mmol/L in the first trimester to 3 mmol/L [47]. In this study, higher triglyceride concentrations in late pregnancy were associated with an increased risk of LGA but also a lower risk of SGA. Results were adjusted for some confounders including pre-pregnancy BMI but not glucose. In our study, the expected negative association of early pregnancy maternal lipid levels with SGA was not found. However, it should be noted that the study by Jin et al. used no national representative reference curves and that the reference curves dated from 1989. It is doubtful if these reference curves are still valid as improvements in the past decades, such as the educational level of the mothers and prenatal nutritional status, led to an increase in infant weight [48]. It may be possible that this has led to an underestimation of SGA (2.4%) and an overestimation of LGA (26.3%). Maternal triglycerides have also been positively associated with newborn fat which may be a more accurate measure of newborn adiposity than birth weight [17, 18]. Triglycerides and remnant cholesterol levels reflect an impaired metabolism of triglyceride-rich lipoproteins and their remnants, which are controlled by placental lipoprotein lipases such as placental lipoprotein lipase (pLPL) and placental endothelial lipase (pEPL) activity [13, 14].
The only study which assessed maternal remnant cholesterol levels, representative of the remnant lipoproteins, was performed in mice and showed that remnant cholesterol is associated with accelerated foetal growth in mice [49]. In our study, maternal remnant cholesterol levels in early pregnancy are positively associated with foetal growth, increased foetal growth pattern of head circumference and abdominal circumference and the risk of LGA, independent of maternal BMI. After correction for glucose, the association of remnant cholesterol and LGA attenuated to just non-significance. This may be explained by the close relation between remnant cholesterol levels and insulin resistance, the association of insulin resistance with glucose levels and the association of insulin resistance with an atherogenic plasma lipid profile [50,51,52].
To fully comprehend the association of maternal lipid levels and foetal growth, it is important to understand the maternal-placental-foetal transport pathways but also the development of the foetal lipid metabolism. Unfortunately, to date, this is still largely unknown. However, we assume that the contribution of the foetal metabolism will be ignorable or very little in early pregnancy, and therefore, we expect that this will have a limited effect on our results. Our results are in line with a meta-analysis of Wang et al. describing a positive association of triglycerides with LGA and birth weight and a negative association of HDL-c with birth weight [53]. The associations were even stronger in overweight or obese women prior to pregnancy. Our study adds to these findings that the associations are even independent of pre-pregnancy BMI.
It is known that children of mothers with high cholesterol levels in early pregnancy have a higher risk of fatty streaks in the aorta [54]. These fatty streaks are a precursor of atherosclerosis and can result in cardiovascular disease later in life [55]. These results underline the importance of measuring maternal lipid levels in early pregnancy.
It has been suggested that maternal fasting glucose levels, postpandrial glucose levels and non-fasting random samples are appropriate measures of maternal glucose metabolism and are related to adverse birth outcomes [56, 57]. A recent study of Barbour et al. suggests that postpandrial triglyceride levels may be a new target for early intervention in obese pregnancies [17], since postpandrial triglycerides compared to fasting triglycerides are better predictors of newborn adiposity. The findings of our study are independent of maternal BMI, and non-fasting blood values may better reflect the normal physiological state in pregnant women [5, 58]. Therefore, we suggest that further studies are needed to replicate our findings, including fasting blood samples and detailed postpandrial measurements.
A few studies examining the effect of HDL-c levels and the risk of LGA did not observe an association [47, 59]. We hypothesized that HDL-c was in contrast to the other lipid levels negatively associated with foetal growth. However, the negative associations of HDL-c with birth weight and LGA attenuated to non-significance after adjustment for pre-pregnancy BMI and glucose. This may be explained by the inverse association between BMI and HDL-c [60].
In this study, we found no association of lipid levels in early pregnancy with adverse birth outcomes in a subset of relatively healthy women (nulliparous, non-smoking, lean women). If the association of lipid levels with adverse birth outcomes would be fully explained by genetics, we would have expected to also find an association of early pregnancy lipid levels with adverse birth outcomes in this relatively healthy population. Since no association was found, we hypothesize that in addition to genetics, lifestyle factors also play an important role in the association of lipid levels with adverse birth outcomes.
Currently, non-high-density lipoprotein cholesterol (non-HDL-c) is often used to describe the total of pro-atherogenic particles (low-density lipoprotein cholesterol [LDL-c], lipoprotein-a, intermediate-density lipoprotein [IDL] and VLDL). High maternal levels of non-HDL-c may therefore be more specific to depict the future cardiovascular risk of the foetus than maternal hypercholesterolemia [61]. This study is to our knowledge the first study to examine the role of maternal early pregnancy lipids including remnant cholesterol and non-HDL-c in association with LGA independent of maternal pre-pregnancy BMI and glucose levels.
Our results suggest a novel association of early pregnancy maternal lipid levels and the risk of a child born LGA. However, it should be noted that foetal growth alone may be a weak surrogate for perinatal harm since there was no difference in NICU admission for women with a child born AGA compared to women with a child born LGA in our study. Before implementation of lifestyle interventions to decrease maternal lipid levels in early pregnancy, future studies are warranted to examine whether maternal lipid levels are not only associated with foetal growth, but also with subsequent perinatal harm such as shoulder dystocia, neonatal asphyxia and neonatal death.
Strengths and limitations
Blood samples were obtained in a non-fasting state, sampled on nonfixed times throughout the day. This may have led to non-differential misclassification, causing an underestimation of the observed effect estimates. However, several large-scale, population-based studies and registries including children, women, men and patients with diabetes have established that plasma lipids and lipoproteins change only modestly in response to habitual food intake [62,63,64,65,66,67]. Among all studies comparing non-fasting with fasting lipid profiles, minor increases in plasma triglycerides and minor decreases in total and LDL cholesterol concentrations were observed, with no change in HDL cholesterol concentrations [67]. These minor and transient changes in lipid concentrations appear to be clinically insignificant [67]. Naturally, the corresponding changes in concentrations in individuals will differ from mean changes in populations, exactly as concentrations will differ from one fasting measurement to another in the same individual [67]. Lipids and lipoproteins change minimally in response to normal food intake [67, 68]. It is stated that only if non-fasting plasma triglycerides are > 5 mmol/L, a fasting blood sample could be considered [67]. In our study, in only three women, triglycerides exceeded 5 mmol/L. Moreover, using non-fasting samples may also have advantages. As previously mentioned, they may better reflect the normal physiological state in pregnant women. Moreover, non-fasting triglycerides were previously observed to be better predictors of newborn adiposity [17]. Compared to non-responders, study participants were more often of European origin, were higher educated, had a lower pre-pregnancy BMI, were more often nulliparous, smoked more often in their pregnancy and more often used folic acid supplementation (Additional file 1, Table S3). It is not possible to foresee whether and, if so, how this would affect our results. Moreover, we included a relatively healthy population and blood samples were obtained in early pregnancy whilst dyslipidaemia is more profound in mid- and late pregnancy which both may have led to an underestimation of the association between maternal lipid profile in early pregnancy with foetal growth and the risk of LGA [69]. Therefore, our results cannot be extrapolated beyond this context. Pre-pregnancy BMI was calculated from self-reported pre-pregnancy weight. However, pre-pregnancy BMI was strongly correlated with BMI measured at enrolment, which makes misclassification unlikely. Gestational weight gain may also have an effect on our results; however, due to the high percentage of missing information (59.3%) and its occurrence after our exposure, we did not include gestational weight gain to our models. In future studies, the role of gestational weight gain should be further examined.
Conclusion
This study suggests a novel association of triglycerides and remnant cholesterol in early pregnancy with foetal growth rates and the risk of a child born LGA. However, future studies are warranted to explore clinical implication possibilities.
Availability of data and materials
Data requests can be made to the secretariat of Generation R.
Abbreviations
- AGA:
-
Average-for-gestational age
- ApoE:
-
Apolipoprotein E
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- DAG:
-
Directed acyclic graph
- DOHaD:
-
Developmental Origins of Health and Disease
- EFW:
-
Estimated foetal weight
- FFA:
-
Free fatty acids
- HDL-c:
-
High-density lipoprotein cholesterol
- IDL:
-
Intermediate-density lipoprotein
- LDL-c:
-
Low-density lipoprotein cholesterol
- LGA:
-
Large-for-gestational age
- LPL:
-
Lipoprotein lipase
- NICU:
-
Neonatal Intensive Care Unit
- OR:
-
Odds ratio
- pEPL:
-
Placental endothelial lipase
- pLPL:
-
Placental lipoprotein lipase
- SD:
-
Standard deviation
- SDS:
-
Standard deviation scores
- SGA:
-
Small-for-gestational age
- VLDL:
-
Very low-density lipoprotein
References
Poston L, Caleyachetty R, Cnattingius S, Corvalan C, Uauy R, Herring S, Gillman MW. Preconceptional and maternal obesity: epidemiology and health consequences. Lancet Diabetes Endocrinol. 2016;4(12):1025–36.
Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA. 2012;307(5):491–7.
Heslehurst N, Rankin J, Wilkinson JR, Summerbell CD. A nationally representative study of maternal obesity in England, UK: trends in incidence and demographic inequalities in 619 323 births, 1989-2007. Int J Obes. 2010;34(3):420–8.
Boulet SL, Alexander GR, Salihu HM, Pass M. Macrosomic births in the United States: determinants, outcomes, and proposed grades of risk. Am J Obstet Gynecol. 2003;188(5):1372–8.
Group HSCR, Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, Hadden DR, McCance DR, Hod M, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358(19):1991–2002.
Geurtsen ML, van Soest EEL, Voerman E, Steegers EAP, Jaddoe VWV, Gaillard R. High maternal early-pregnancy blood glucose levels are associated with altered fetal growth and increased risk of adverse birth outcomes. Diabetologia. 2019;62(10):1880–90.
Cho HY, Jung I, Kim SJ. The association between maternal hyperglycemia and perinatal outcomes in gestational diabetes mellitus patients: a retrospective cohort study. Medicine (Baltimore). 2016;95(36):e4712.
Ehrenberg HM, Mercer BM, Catalano PM. The influence of obesity and diabetes on the prevalence of macrosomia. Am J Obstet Gynecol. 2004;191(3):964–8.
Gaudet L, Ferraro ZM, Wen SW, Walker M. Maternal obesity and occurrence of fetal macrosomia: a systematic review and meta-analysis. Biomed Res Int. 2014;2014:640291.
Acharya G, Albrecht C, Benton SJ, Cotechini T, Dechend R, Dilworth MR, Duttaroy AK, Grotmol T, Heazell AE, Jansson T, et al. IFPA Meeting 2011 workshop report I: placenta: predicting future health; roles of lipids in the growth and development of feto-placental unit; placental nutrient sensing; placental research to solve clinical problems--a translational approach. Placenta. 2012;33(Suppl):S4–8.
Herrera E. Lipid metabolism in pregnancy and its consequences in the fetus and newborn. Endocrine. 2002;19(1):43–55.
Herrera E, Ortega-Senovilla H. Lipid metabolism during pregnancy and its implications for fetal growth. Curr Pharm Biotechnol. 2014;15(1):24–31.
Heerwagen MJR, Gumina DL, Hernandez TL, Van Pelt RE, Kramer AW, Janssen RC, Jensen DR, Powell TL, Friedman JE, Winn VD, et al. Placental lipoprotein lipase activity is positively associated with newborn adiposity. Placenta. 2018;64:53–60.
Magnusson-Olsson AL, Hamark B, Ericsson A, Wennergren M, Jansson T, Powell TL. Gestational and hormonal regulation of human placental lipoprotein lipase. J Lipid Res. 2006;47(11):2551–61.
Perazzolo S, Hirschmugl B, Wadsack C, Desoye G, Lewis RM, Sengers BG. The influence of placental metabolism on fatty acid transfer to the fetus. J Lipid Res. 2017;58(2):443–54.
Yang Z, Zhao Y, Bennett MJ, Strauss AW, Ibdah JA. Fetal genotypes and pregnancy outcomes in 35 families with mitochondrial trifunctional protein mutations. Am J Obstet Gynecol. 2002;187(3):715–20.
Barbour LA, Farabi SS, Friedman JE, Hirsch NM, Reece MS, Van Pelt RE, Hernandez TL. Postprandial triglycerides predict newborn fat more strongly than glucose in women with obesity in early pregnancy. Obesity (Silver Spring). 2018;26(8):1347–56.
Harmon KA, Gerard L, Jensen DR, Kealey EH, Hernandez TL, Reece MS, Barbour LA, Bessesen DH. Continuous glucose profiles in obese and normal-weight pregnant women on a controlled diet: metabolic determinants of fetal growth. Diabetes Care. 2011;34(10):2198–204.
Eriksson J, Forsen T, Tuomilehto J, Osmond C, Barker D. Fetal and childhood growth and hypertension in adult life. Hypertension. 2000;36(5):790–4.
Forsen T, Eriksson J, Tuomilehto J, Reunanen A, Osmond C, Barker D. The fetal and childhood growth of persons who develop type 2 diabetes. Ann Intern Med. 2000;133(3):176–82.
Gluckman PD, Hanson MA, Cooper C, Thornburg KL. Effect of in utero and early-life conditions on adult health and disease. N Engl J Med. 2008;359(1):61–73.
Adank MC, Benschop L, Peterbroers KR, Smak Gregoor AM, Kors AW, Mulder MT, Schalekamp-Timmermans S, Roeters Van Lennep JE, EAP S. Is maternal lipid profile in early pregnancy associated with pregnancy complications and blood pressure in pregnancy and long term postpartum? Am J Obstet Gynecol. 2019;221(2):150 e151–13.
Barker DJ. The origins of the developmental origins theory. J Intern Med. 2007;261(5):412–7.
Kooijman MN, Kruithof CJ, van Duijn CM, Duijts L, Franco OH, van IJzendoorn MH, de Jongste JC, Klaver CCW, van der Lugt A, Mackenbach JP et al: The Generation R Study: design and cohort update 2017. Eur J Epidemiol 2016, 31(12):1243–1264.
World Medical A. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–4.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, Initiative S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–9.
Kruithof CJ, Kooijman MN, van Duijn CM, Franco OH, de Jongste JC, Klaver CC, Mackenbach JP, Moll HA, Raat H, Rings EH, et al. The Generation R Study: Biobank update 2015. Eur J Epidemiol. 2014;29(12):911–27.
Hadlock FP, Deter RL, Harrist RB, Park SK. Fetal abdominal circumference as a predictor of menstrual age. AJR Am J Roentgenol. 1982;139(2):367–70.
Hadlock FP, Harrist RB, Deter RL, Park SK. Fetal femur length as a predictor of menstrual age: sonographically measured. AJR Am J Roentgenol. 1982;138(5):875–8.
Verburg BO, Steegers EA, De Ridder M, Snijders RJ, Smith E, Hofman A, Moll HA, Jaddoe VW, Witteman JC. New charts for ultrasound dating of pregnancy and assessment of fetal growth: longitudinal data from a population-based cohort study. Ultrasound Obstet Gynecol. 2008;31(4):388–96.
Hadlock FP, Harrist RB, Sharman RS, Deter RL, Park SK. Estimation of fetal weight with the use of head, body, and femur measurements--a prospective study. Am J Obstet Gynecol. 1985;151(3):333–7.
Niklasson A, Ericson A, Fryer JG, Karlberg J, Lawrence C, Karlberg P. An update of the Swedish reference standards for weight, length and head circumference at birth for given gestational age (1977-1981). Acta Paediatr Scand. 1991;80(8–9):756–62.
Santos S, Zugna D, Pizzi C, Richiardi L. Sources of confounding in life course epidemiology. J Dev Orig Health Dis. 2019;10(3):299–305.
Gaillard R, Durmus B, Hofman A, Mackenbach JP, Steegers EA, Jaddoe VW. Risk factors and outcomes of maternal obesity and excessive weight gain during pregnancy. Obesity (Silver Spring). 2013;21(5):1046–55.
Coolman M, de Groot CJM, Jaddoe VW, Hofman A, Raat H, Steegers EAP. Medical record validation of maternally reported history of preeclampsia. J Clin Epidemiol. 2010;63(8):932–7.
Brown MA, Lindheimer MD, de Swiet M, Van Assche A, Moutquin JM. The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertens Pregnancy. 2001;20(1):IX–XIV.
Timmermans S, Bonsel GJ, Steegers-Theunissen RP, Mackenbach JP, Steyerberg EW, Raat H, Verbrugh HA, Tiemeier HW, Hofman A, Birnie E, et al. Individual accumulation of heterogeneous risks explains perinatal inequalities within deprived neighbourhoods. Eur J Epidemiol. 2011;26(2):165–80.
Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, Wood AM, Carpenter JR. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393.
Graham JW, Olchowski AE, Gilreath TD. How many imputations are really needed? Some practical clarifications of multiple imputation theory. Prev Sci. 2007;8(3):206–13.
Twisk J. Applied longitudinal data analysis for epidemiology: a practical guide. Cambridge: Cambridge University Press; 2013.
Geraghty AA, Alberdi G, O'Sullivan EJ, O'Brien EC, Crosbie B, Twomey PJ, McAuliffe FM. Maternal blood lipid profile during pregnancy and associations with child adiposity: findings from the ROLO study. PLoS One. 2016;11(8):e0161206.
Kushtagi P, Arvapally S. Maternal mid-pregnancy serum triglyceride levels and neonatal birth weight. Int J Gynaecol Obstet. 2009;106(3):258–9.
Vrijkotte TG, Algera SJ, Brouwer IA, van Eijsden M, Twickler MB. Maternal triglyceride levels during early pregnancy are associated with birth weight and postnatal growth. J Pediatr. 2011;159(5):736–42 e731.
Di Cianni G, Miccoli R, Volpe L, Lencioni C, Ghio A, Giovannitti MG, Cuccuru I, Pellegrini G, Chatzianagnostou K, Boldrini A, et al. Maternal triglyceride levels and newborn weight in pregnant women with normal glucose tolerance. Diabet Med. 2005;22(1):21–5.
Gobl CS, Handisurya A, Klein K, Bozkurt L, Luger A, Bancher-Todesca D, Kautzky-Willer A. Changes in serum lipid levels during pregnancy in type 1 and type 2 diabetic subjects. Diabetes Care. 2010;33(9):2071–3.
Schaefer-Graf UM, Graf K, Kulbacka I, Kjos SL, Dudenhausen J, Vetter K, Herrera E. Maternal lipids as strong determinants of fetal environment and growth in pregnancies with gestational diabetes mellitus. Diabetes Care. 2008;31(9):1858–63.
Jin WY, Lin SL, Hou RL, Chen XY, Han T, Jin Y, Tang L, Zhu ZW, Zhao ZY. Associations between maternal lipid profile and pregnancy complications and perinatal outcomes: a population-based study from China. BMC Pregnancy Childbirth. 2016;16:60.
Dai L, Deng C, Li Y, Zhu J, Mu Y, Deng Y, Mao M, Wang Y, Li Q, Ma S, et al. Birth weight reference percentiles for Chinese. PLoS One. 2014;9(8):e104779.
Rebholz SL, Burke KT, Yang Q, Tso P, Woollett LA. Dietary fat impacts fetal growth and metabolism: uptake of chylomicron remnant core lipids by the placenta. Am J Physiol Endocrinol Metab. 2011;301(2):E416–25.
Ohnishi H, Saitoh S, Takagi S, Ohata J, Isobe T, Kikuchi Y, Takeuchi H, Shimamoto K. Relationship between insulin-resistance and remnant-like particle cholesterol. Atherosclerosis. 2002;164(1):167–70.
Schaefer EJ, McNamara JR, Shah PK, Nakajima K, Cupples LA, Ordovas JM, Wilson PW, Framingham Offspring S. Elevated remnant-like particle cholesterol and triglyceride levels in diabetic men and women in the Framingham Offspring Study. Diabetes Care. 2002;25(6):989–94.
DeFronzo RA, Ferrannini E. Insulin resistance. A multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Diabetes Care. 1991;14(3):173–94.
Wang J, Moore D, Subramanian A, Cheng KK, Toulis KA, Qiu X, Saravanan P, Price MJ, Nirantharakumar K. Gestational dyslipidaemia and adverse birthweight outcomes: a systematic review and meta-analysis. Obes Rev. 2018;19(9):1256–68.
Palinski W, Napoli C. The fetal origins of atherosclerosis: maternal hypercholesterolemia, and cholesterol-lowering or antioxidant treatment during pregnancy influence in utero programming and postnatal susceptibility to atherogenesis. FASEB J. 2002;16(11):1348–60.
Napoli C, D'Armiento FP, Mancini FP, Postiglione A, Witztum JL, Palumbo G, Palinski W. Fatty streak formation occurs in human fetal aortas and is greatly enhanced by maternal hypercholesterolemia - intimal accumulation of low density lipoprotein and its oxidation precede monocyte recruitment into early atherosclerotic lesions. J Clin Invest. 1997;100(11):2680–90.
Catalano PM, McIntyre HD, Cruickshank JK, McCance DR, Dyer AR, Metzger BE, Lowe LP, Trimble ER, Coustan DR, Hadden DR, et al. The hyperglycemia and adverse pregnancy outcome study: associations of GDM and obesity with pregnancy outcomes. Diabetes Care. 2012;35(4):780–6.
Farrar D, Simmonds M, Bryant M, Sheldon TA, Tuffnell D, Golder S, Dunne F, Lawlor DA. Hyperglycaemia and risk of adverse perinatal outcomes: systematic review and meta-analysis. BMJ. 2016;354:i4694.
Clausen T, Burski TK, Oyen N, Godang K, Bollerslev J, Henriksen T. Maternal anthropometric and metabolic factors in the first half of pregnancy and risk of neonatal macrosomia in term pregnancies. A prospective study. Eur J Endocrinol. 2005;153(6):887–94.
Emet T, Ustuner I, Guven SG, Balik G, Ural UM, Tekin YB, Senturk S, Sahin FK, Avsar AF. Plasma lipids and lipoproteins during pregnancy and related pregnancy outcomes. Arch Gynecol Obstet. 2013;288(1):49–55.
Shamai L, Lurix E, Shen M, Novaro GM, Szomstein S, Rosenthal R, Hernandez AV, Asher CR. Association of body mass index and lipid profiles: evaluation of a broad spectrum of body mass index patients including the morbidly obese. Obes Surg. 2011;21(1):42–7.
Cui Y, Blumenthal RS, Flaws JA, Whiteman MK, Langenberg P, Bachorik PS, Bush TL. Non-high-density lipoprotein cholesterol level as a predictor of cardiovascular disease mortality. Arch Intern Med. 2001;161(11):1413–9.
Langsted A, Freiberg JJ, Nordestgaard BG. Fasting and nonfasting lipid levels: influence of normal food intake on lipids, lipoproteins, apolipoproteins, and cardiovascular risk prediction. Circulation. 2008;118(20):2047–56.
Langsted A, Nordestgaard BG. Nonfasting lipids, lipoproteins, and apolipoproteins in individuals with and without diabetes: 58 434 individuals from the Copenhagen General Population Study. Clin Chem. 2011;57(3):482–9.
Mora S, Rifai N, Buring JE, Ridker PM. Fasting compared with nonfasting lipids and apolipoproteins for predicting incident cardiovascular events. Circulation. 2008;118(10):993–1001.
Sidhu D, Naugler C. Fasting time and lipid levels in a community-based population: a cross-sectional study. Arch Intern Med. 2012;172(22):1707–10.
Steiner MJ, Skinner AC, Perrin EM. Fasting might not be necessary before lipid screening: a nationally representative cross-sectional study. Pediatrics. 2011;128(3):463–70.
Nordestgaard BG, Langsted A, Mora S, Kolovou G, Baum H, Bruckert E, Watts GF, Sypniewska G, Wiklund O, Boren J, et al. Fasting is not routinely required for determination of a lipid profile: clinical and laboratory implications including flagging at desirable concentration cut-points-a joint consensus statement from the European Atherosclerosis Society and European Federation of Clinical Chemistry and Laboratory Medicine. Eur Heart J. 2016;37(25):1944–58.
Langsted A, Nordestgaard BG. Nonfasting versus fasting lipid profile for cardiovascular risk prediction. Pathology. 2019;51(2):131–41.
Alvarez JJ, Montelongo A, Iglesias A, Lasuncion MA, Herrera E. Longitudinal study on lipoprotein profile, high density lipoprotein subclass, and postheparin lipases during gestation in women. J Lipid Res. 1996;37(2):299–308.
Acknowledgements
The Generation R Study is conducted by the Erasmus Medical Centre in close collaboration with the School of Law and Faculty of Social Sciences of the Erasmus University Rotterdam, the Municipal Health Service Rotterdam area, the Rotterdam Homecare Foundation and the Stichting Trombosedienst and Artsenlaboratorium Rijnmond (STAR). We gratefully acknowledge the contribution of participating mothers, general practitioners, hospitals, midwives and pharmacies in Rotterdam.
Funding
The Generation R Study was made possible by financial support from Erasmus MC, University Medical Centre Rotterdam, the Netherlands; the Netherlands Organization for Health Research and Development; the Netherlands Organization for Scientific Research; the Ministry of Health, Welfare and Sport; and the Ministry of Youth and Families.
Author information
Authors and Affiliations
Contributions
MA and LB analysed the data and wrote the article. AK, KP and AS contributed to the design of the paper and assisted with the analyses and writing of the article. MM and SS contributed to the design of the paper, interpretation of the data and revisions and gave input at all stages of the study. JR and ES contributed to the design of the paper, writing of the article, interpretation of the data and revisions and gave input at all stages of the study. All authors have approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study has been approved by the Medical Ethical Committee of the Erasmus Medical Centre in Rotterdam on December 17, 2001 (MEC 198.782/2001/31). Written consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
None declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1:
Figure S1. Directed acyclic graph (DAG) of exposure, outcome and possible covariates. Table S1. Association of maternal lipid profile in early pregnancy with birth outcomes, excluding women with a hypertensive disorder of pregnancy. Table S2a. Maternal lipid profile in early pregnancy of the total population (n = 5702) and a subgroup of nulliparous, non-smoking women with a pre-pregnancy BMI < 25 kg/m2 (n = 1915). Table S2b. Association of maternal lipid profile in early pregnancy with birth outcomes in a subgroup of nulliparous, non-smoking women with a pre-pregnancy BMI < 25 kg/m2 (n = 1915). Table S3. Baseline characteristics between women with and without available lipid measurements in early pregnancy.
Additional file 2.
STROBE statement.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Adank, M.C., Benschop, L., Kors, A.W. et al. Maternal lipid profile in early pregnancy is associated with foetal growth and the risk of a child born large-for-gestational age: a population-based prospective cohort study. BMC Med 18, 276 (2020). https://doi.org/10.1186/s12916-020-01730-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-020-01730-7