
Abstract
Background
The Center for Medicare and Medicaid Services (CMS) and the Hospital Quality Alliance began collecting and reporting United States hospital performance in the treatment of pneumonia and heart failure in 2008. Whether the utilization of hospice might affect CMS-reported mortality and readmission rates is not known.
Methods
Hospice utilization (mean days on hospice per decedent) for 2012 from the Dartmouth Atlas (a project of the Dartmouth Institute that reports a variety of public health and policy-related statistics) was merged with hospital-level 30-day mortality and readmission rates for pneumonia and heart failure from CMS. The association between hospice use and outcomes was analyzed with multivariate quantile regression controlling for quality of care metrics, acute care bed availability, regional variability and other measures.
Results
2196 hospitals reported data to both CMS and the Dartmouth Atlas in 2012. Higher rates of hospice utilization were associated with lower rates of 30-day mortality and readmission for pneumonia but not for heart failure. Higher quality of care was associated with lower rates of mortality for both pneumonia and heart failure. Greater acute care bed availability was associated with increased readmission rates for both conditions (p < 0.05 for all).
Conclusions
Higher rates of hospice utilization were associated with lower rates of 30-day mortality and readmission for pneumonia as reported by CMS. While causality is not established, it is possible that hospice referrals might directly affect CMS outcome metrics. Further clarification of the relationship between hospice referral patterns and publicly reported CMS outcomes appears warranted.
Similar content being viewed by others


Background
In 2002 the Center for Medicare and Medicaid Services (CMS) and the Hospital Quality Alliance (HQA) began work on the evaluation and reporting of hospital performance on various process and outcome measures [1]. The resulting Hospital Compare website began reporting 10 core process measures in 2005; better performance on these process measures was correlated with a small improvement in risk-adjusted mortality [2]. Reporting of hospital-level 30-day mortality and readmission rates for acute myocardial infarction, heart failure and pneumonia soon followed.
Prior to reporting these outcomes, internal discussion at CMS addressed the matter of how to handle the question of hospice status [3]. The concern was that exclusion of all hospice patients might introduce a moral hazard, that is, an incentive to prematurely enroll high-risk patients in hospice during their hospital course in order to reduce reported mortality rates. Ultimately, the 30-day mortality rates reported beginning in 2008 excluded patients who were enrolled in hospice prior to or on the first hospital day [4]. No such adjustment was made when reporting of 30-day readmission rates began in 2010, and patients enrolled in hospice were included in these outcome measures [5].
Whether or not these policies have been successful in eliminating systemic bias related to hospice utilization is not known. However, there exist plausible mechanisms by which hospice utilization could lead to differences in outcome measures (both mortality and readmission rates). As 30-day mortality rates exclude patients previously enrolled in hospice, it is possible that hospitals with a higher proportion of patients enrolled in hospice might have lower 30-day mortality rates because of the exclusion of those hospice patients. CMS performs risk-adjustment of these 30-day mortality rates (based upon data abstracted from billing codes) [6] and it is possible that if patients enrolled in hospice have an elevated mortality risk not captured by that risk adjustment, the selective exclusion of those high-risk patients could artifactually reduce the reported 30-day mortality rates by hospitals with a high proportion of high-risk (hospice-enrolled) patients.
For hospital-level readmission rates, if patients on hospice are less likely to be readmitted, then hospitals with a larger proportion of hospice patients may demonstrate lower readmission rates. Both of these possible effects may be wholly independent of the quality of medical care provided.
Using the hospital as the unit of study, we obtained data regarding hospice utilization from the Dartmouth Atlas [7] and CMS-reported outcomes from Hospital Compare [8] in order to evaluate the question of whether the amount of hospice utilization had any association with the mortality and readmission rates reported by CMS for US hospitals. Mortality and readmission rates for pneumonia and heart failure were chosen as outcomes for their potential relevance to end-of-life decision making [9, 10]; acute myocardial infarction was not included given its lower probability of relevance to end-of-life decision making.
Methods
Data
The Center for Medicare and Medicaid Services (CMS) has reported United States hospital-level 30-day mortality rates for pneumonia, acute myocardial infarction and heart failure since 2008, and 30-day readmission rates for those same conditions since 2010 [1].CMS uses administrative claims data to adjust for the variation in acuity and comorbid conditions encountered by different hospitals [11], an approach that has been shown to be comparable to models built using clinical data [6]. 30-day risk-standardized mortality and readmission rates for these conditions are reported as percentages.
As hospice utilization is not reported by CMS, a separate data source was required. The Dartmouth Atlas provides hospital-level data on hospice utilization among patients enrolled in traditional fee-for-service Medicare (Parts A and B) who were hospitalized at some point during the final 2 years of their life with a diagnosis code of one of nine chronic conditions (Additional file 1: Table S1) [12]. Included in this data is the number of days spent in hospice per decedent, percentage of decedents enrolled in hospice and Medicare spending broken down by category, in addition to a variety of other healthcare utilization metrics. Patients with admissions at more than one hospital were assigned to the hospital they used most frequently [12]. The Dartmouth Atlas is a project of the Dartmouth Institute, a center for research, education and policy advocacy [13].
As our unit of measure was the hospital, we obtained data from 2012, the most recent year in which data from both the Dartmouth Atlas and CMS was available (downloaded from their respective websites) [7, 8]. Measures of hospice utilization (Dartmouth Atlas) and 30-day mortality or readmission (CMS) were merged at the hospital level.
This study analyzed publicly available data and did not involve any patient-level information, it was exempted (as per 45 CFR 46.101(b)(4)) from review by the Intermountain Healthcare Institutional Review Board.
Definitions and other variables
Hospice utilization is reported by the Dartmouth Atlas as either percentage of decedents enrolled in hospice or the number of days spent on hospice per decedent for a given hospital. As the percentage of decedents enrolled in hospice could be identical for two hospitals with very early or very late enrollment in hospice, we chose to use days spent on hospice per decedent as it reflects both proportional and temporal hospice utilization.
Several prespecified covariates were included in the model to reduce potential sources of confounding. A composite quality measure was created from process of care measures reported by each hospital to CMS using standard methodology and expressed as a percentage (i.e., mean performance on publicly reported outcome measures, e.g. door-to-balloon time of <90 min for ST-elevation myocardial infarction, or perioperative antibiotics, a full list of which is available in Additional file 1: Table S2) [14]. Median household income of each hospital zip code as well as population density were obtained from United States (US) census data [15, 16]. Acute care beds per 1000 residents in each hospital service area was obtained from the Dartmouth Atlas [7]. Hospitals were divided into the four primary regions of the country as defined by the US Census Bureau, with the Midwestern region set as the reference region for its central location and central-leaning socioeconomic characteristics [17].
Statistical methods
In order to evaluate the possibility of non-linear associations, we performed multivariable quantile regression [18] to describe the association between hospital-level hospice utilization and 30-day mortality and readmission rates for pneumonia and heart failure in 2012 as reported by CMS. As opposed to ordinary regression, which models the mean of an outcome, quantile regression allows modeling of various quantiles; we modeled the 25th, 50th (median) and 75th percentiles. (Further details regarding quantile regression are available in the Additional file 1).
An estimate of effect size regarding hospice utilization and the publicly reported outcome was made by taking the mean of the three regression lines and then calculating the difference in outcome rates for hospitals in the 25th percentile of hospice utilization and those in the 75th percentile of hospice utilization. For ease of interpretation, this change in publicly reported outcome rate was expressed as a function of change in relative percentile of performance.
A linear multilevel regression was also performed as a sensitivity analysis, with random intercepts grouped by region (allowing for variance in baseline hospice utilization rates by region), and all other above variables as fixed effects. Standard assumptions of linear mixed models (i.e. normal distribution, no within-group correlation in the covariance structure) were applied.
We performed all analyses in the R Statistical Package, version 3.1.3 [19].
Results
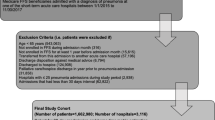
The total number of United States hospitals with data from both CMS (30-day mortality and readmission rates, N = 4477) and the Dartmouth Atlas (mean days on hospice per decedent, N = 2503) was 2196.
Each hospital reported the mean number of days spent in hospice per decedent during the last 6 months of life. The median for reporting hospitals was 19.8 days with an interquartile range (IQR) of 15.2–24.6. The percentage of patients enrolled in hospice at time of death was also reported; the median of reporting hospitals was 52.0% (IQR 43.6–59.7). Additional data is in Additional file 1: Table S3, listed by quantiles of hospice utilization.
Median values of CMS-reported outcomes for pneumonia: 30-day mortality rates were 12.0% (IQR 10.7–13.1) and 30-day readmissions rates were 18.5% (IQR 17.4–19.8). For heart failure, 30-day mortality rates were 11.5% (IQR 10.4–12.7) and 30-day readmission rates were 24.7% (IQR 23.4–26.1).
Pneumonia 30-day mortality rates
Higher rates of hospice utilization were associated with decreased 30-day pneumonia mortality for hospitals in the 25th (p = 0.02), 50th (p < 0.001) and 75th percentiles (p = 0.04), after controlling for covariates, including quality of care scores. Hospital 30-day pneumonia mortality rates are presented as a scatterplot in Fig. 1, which illustrates the utility of quantile regression (25th, 50th and 75th percentiles) to better model non-linearities in the data.

Scatterplot of 30-day pneumonia mortality rates and mean number of days in hospice per decedent; quantile regression lines are blue (25th, median and 75th percentiles), the ordinary least squares line is dotted red
Higher quality of care scores, higher median income and greater population density were also associated with lower rates of 30-day mortality for all 3 quantiles (p < 0.05), as reported in Table 1. Hospitals in the southern region of the US had higher 30-day mortality rates for pneumonia (Table 1) than those in the reference group (Midwest).
Pneumonia 30-day readmission rates
Higher rates of hospice utilization were consistently associated with lower 30-day pneumonia readmission rates for hospitals in the 25th (p = 0.02), 50th (p = 0.002) and 75th percentiles (p = 0.04), after controlling for covariates, including quality of care metrics (Table 2).
A greater number of acute care beds available per 1000 residents and higher population density were associated with higher readmission rates (p < 0.05) in all 3 quantiles. Higher quality of care scores were also associated with higher readmission rates in the 50th and 75th percentiles, while higher median income was associated with higher readmission rates in the 25th and 50th percentiles (p < 0.05). The western US had lower readmission rates in comparison to the reference group (Midwest).
Heart failure 30-day mortality rates
Increased hospice utilization was associated with higher 30-day mortality in the 25th percentile (p = 0.01), but not in the 50th and 75th percentiles (Additional file 1: Table S4). Higher quality of care scores were associated with decreased 30-day mortality rates for heart failure in all 3 quantiles (p < 0.05). Higher population density was associated with lower 30-day mortality rates in all 3 quantiles (p < 0.05) and higher median income was associated with lower 30-day mortality rates in 2 of 3 quantiles (p < 0.05). No regional effects were observed.
Heart failure 30-day readmission rates
Higher rates of hospice utilization were associated with lower 30-day readmission rates for heart failure in the 50th percentile (median) only (p = 0.01), as seen in Additional file 1: Table S5.
A greater number of acute care beds available per 1000 residents was associated with higher readmission rates in all 3 quantiles (p < 0.05), as were greater median income and higher population density (p < 0.05). Higher quality of care scores were not associated with heart failure readmission rates. The Northeast and Southern regions had higher rates of readmission in comparison to the Midwestern region.
More detail regarding each of the above quantile regressions is available in the Additional file 1: Table S6-S9.
Effect size
For both pneumonia mortality and readmission, a change in hospice utilization sufficient to move from the 25th to the 75th percentile would be associated with a change in pneumonia mortality or readmission rates equivalent to at most 5% relative to other reporting hospitals.
Sensitivity analysis
Higher rates of hospice utilization were associated with lower 30-day mortality and readmission rates for pneumonia as well as lower 30-day readmission rates for heart failure (p < 0.05 for all) in a multilevel model (random intercept, grouped by region) performed as a sensitivity analysis. Lattice plots of regional hospice utilization and publicly reported pneumonia mortality rates are available in Fig. 2, with further detail regarding each of the multilevel models in the Additional file 1: Table S10-S13.

Hospice utilization and pneumonia mortality rates for the four regions of the United States
Discussion
Among hospitals reporting both hospice utilization and CMS outcomes during 2012, those hospitals with higher rates of hospice utilization reported lower 30-day mortality and readmission rates for pneumonia. These associations persisted after controlling for quality of care. These results raise questions about whether and to what extent patients’ choices to undertake less aggressive medical therapy might influence the hospital-level outcome rates reported by CMS.
Importantly, the two major outcome measures (30-day mortality and 30-day hospital readmission) handle hospice status differently. Hospital 30-day mortality rates exclude patients enrolled in hospice before the second hospital day, while 30-day readmission rates include hospice patients.
Our finding that hospitals with a greater proportion of patients enrolled in hospice have lower CMS-reported 30-day mortality rates for pneumonia suggests that the exclusion of these patients may have introduced an artifact in hospital-level reported 30-day mortality rates. This is likely caused by an interaction between the severity of illness risk-adjustment performed by CMS and higher mortality seen in hospice patients that is not captured by that CMS risk-adjustment algorithm (based as it is on data abstracted from billing codes) [6]. If preferentially high-risk patients are systematically excluded from certain hospitals at a higher rate, it then follows that those same hospitals might similarly report an artifactually lower 30-day mortality rate than comparable hospitals with a lower proportion of excluded high-risk (i.e., hospice-enrolled) patients. Our findings are compatible with, although not proof of, such a mechanism, among patients with pneumonia.
Readmission rates are calculated differently; hospice patients are included in these measures. If patients enrolled in hospice have a lower risk of readmission (based on a likely desire to die at home or another non-hospital setting) [20], then hospitals with higher rates of hospice utilization should have lower readmission rates, which is, again, what we observed for pneumonia.
Such associations could also represent a measure of quality that is not captured in the standard quality metrics (i.e., hospitals with higher hospice utilization also provide better care not measured by current metrics or communities that support hospice measures have distinct demographics, as may be the case in La Crosse, Wisconsin) or it could represent the above methods of accounting for patients on hospice. No matter the mechanism, this could create a moral hazard, an incentive for healthcare facilities to encourage hospice use independent of individual patients’ desires for it.
In other words, CMS-reported outcomes may inadvertently incentivize certain institutional or community initiatives [21], that lead to higher rates of hospice utilization independent of patient characteristics and/or preferences. That payments to hospitals by CMS are also partly linked to performance on these CMS-reported outcome rates (via the Value Based Purchasing program) adds a complex financial component to this discussion. Whether this specific incentive shapes hospice strategy at the community or hospital level is not known: we do not believe such a moral hazard is responsible for the main associations found in our study.
Pneumonia is an important disease state relevant to questions about end-of-life decision making, as it is frequently the cause of death in vulnerable patients with multiple comorbidities towards the end of life [22, 23]. No consistent effect of hospice utilization was observed for heart failure mortality and readmission in our primary analysis. Whether this reflects a difference in the mechanism of death, the underlying CMS risk-adjustment algorithms (the heart failure readmission model has very limited predictive accuracy) [24], the availability of “rescue” therapies for advanced heart failure [25], the longitudinal relationship with a heart failure team, or perhaps masking of an effect by collinearity with other covariates is unknown.
The effect size in our study was modest, but we believe that it likely underestimates the true effect size. Our analysis used matched hospital data, but the CMS-reported outcomes were condition-specific, whereas hospice utilization was reported by the Dartmouth Atlas using patients with any of a panel of chronic illnesses [12]. The populations are not strictly overlapping, even as they come from the same hospitals. We suspect that condition-specific hospice utilization would confirm our findings, with a more robust effect size, by decreasing experimental noise from unrelated patient populations. A sensitivity analysis, using a multilevel model confirmed the main findings of this study.
Our findings also add to the study of resource utilization and healthcare preferences, which have reported mixed results in terms of reducing readmission rates and other markers of healthcare utilization following interventions designed to increase the use of palliative care services (including hospice) [26,27,28,29]. The amount of hospice utilization observed in our study is consistent with previously published results and trends [30]. We also observed that hospitals with higher quality of care scores had lower 30-day mortality rates for both pneumonia and heart failure, consistent with a 2006 study of CMS measures [2], and a multicenter study of Medicare patients in 1997 [31].
Our analysis also found an association between acute care bed availability and readmission rates, echoing a 1994 study of hospitals in Boston and New Haven that found readmission rates after inpatient treatment for one of five conditions was 60% higher in Boston, a finding not explained by severity of illness [32]. Say’s Law of classical economics [33], ‘supply creates its own demand’, may apply to this association between bed availability and readmission rates, independent of patient outcomes or preferences [34, 35].
Other researchers have also identified unexpected interactions between publicly reported outcomes and patient-level factors associated with end-of-life decision making. In a study of California inpatients with pneumonia, higher DNR (Do Not Resuscitate, an advance directive that precludes resuscitation in the event of cardiac arrest) rates were associated with higher mortality rates. However, after adjusting for patient DNR status and inter-hospital variability in DNR rates, those hospitals with higher DNR rates were found to have lower pneumonia mortality rates, suggesting that taking this information into account could lead to more accurate reporting [36].
Our findings have limitations. Unmeasured confounding could introduce bias, although we controlled for quality of care, geographical region, and acute care bed availability as well as more local effects such as median income and population density. The exact metric of hospice utilization, mean number of days in hospice per decedent for a given hospital, was chosen as it reflected both duration and proportion of hospice utilization. As the unit of study was the hospital, our results cannot necessarily be generalized to other levels of measurement, such as individual patients or larger geographic associations. No adjustment was made for the multiple comparisons made in this study.
Conclusion
In conclusion, we present evidence that higher rates of hospice utilization are associated with lower 30-day pneumonia mortality and readmission rates as reported by CMS. The extent to which this association represents or fails to represent the values and priorities of individual patients and their families deserves further study to be sure that regulatory incentives appropriately align with patient-centered medical care.
Abbreviations
- CMS:
-
Center for medicare and medicaid services
- DNR:
-
Do not resuscitate
- HQA:
-
Hospital quality alliance
- US:
-
United States
References
Center for Medicare and Medicaid Services. Hospital Compare. 2015; https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/hospitalqualityinits/hospitalcompare.html. Accessed 7 Nov 2015.
Werner RM, Bradlow ET. Relationship between Medicare’s hospital compare performance measures and mortality rates. JAMA. 2006;296(22):2694–702.
Center for Medicare and Medicaid Services. Frequently asked questions: implementation and maintenance of CMS mortality measures for AMI & HF. 2007; https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/hospitalqualityinits/downloads/hospitalmortalityaboutami_hf.pdf. Accessed 7 Nov 2015.
Cassel JB, Jones AB, Meier DE, Smith TJ, Spragens LH, Weissman D. Hospital mortality rates: how is palliative care taken into account? J Pain Symptom Manag. 2010;40(6):914–25.
Jea S. CMS Hospital quality Chartbook 2014. New Haven: Yale New Haven Health Services Corporation Center for Outcomes Research and Evaluation; 2014.
Bratzler DW, Normand SL, Wang Y, et al. An administrative claims model for profiling hospital 30-day mortality rates for pneumonia patients. PLoS One. 2011;6(4):e17401.
The Dartmouth Institute. The Dartmouth atlas of health care. 2015; http://www.dartmouthatlas.org/. Accessed 9 Sep 2015.
Center for Medicare and Medicaid Services. Outcome Measures. 2015; https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/hospitalqualityinits/outcomemeasures.html. Accessed 9 Sep 2015.
Abdel-Karim IA, Sammel RB, Prange MA. Causes of death at autopsy in an inpatient hospice program. J Palliat Med. 2007;10(4):894–8.
National Center for Health Statistics. Hyattsville: Health, United States, 2012: With Special Feature on Emergency Care; 2013.
Suter LG, Li SX, Grady JN, et al. National patterns of risk-standardized mortality and readmission after hospitalization for acute myocardial infarction, heart failure, and pneumonia: update on publicly reported outcomes measures based on the 2013 release. J Gen Intern Med. 2014;29(10):1333–40.
The Dartmouth Institute for Health Policy and Clinical Practice. Methods appendix. Trends and Variation in End-of-Life Care for Medicare Beneficiaries with Severe Chronic Illness. The Trustees of Dartmouth College: 2011.
The Dartmouth Institute. About. 2015; http://tdi.dartmouth.edu/about. Accessed 7 Nov 2015.
Center for Medicare and Medicaid Services. CMS HQI Demostration project: composite quality score methodology overview. 2004.
United States Census Bureau. American community survey 2012 5-year estimates. 2012; http://factfinder2.census.gov/. Accessed 15 Feb 2016.
United States Census Bureau. Summary file 1 of 2010 census. 2010; http://factfinder2.census.gov/. Accessed 15 Feb 2016.
U.S. Census Bureau. Regions and divisions. 2015; https://www2.census.gov/geo/docs/maps-data/maps/reg_div.txt. Accessed 25 May 2016.
Cade BS, Noon BR. A gentle introduction to quantile regression for ecologists. Front Ecol Environ. 2003;1:412–20.
R Core Team. R: A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2015. http://www.R-project.org/.
Barclay JS, Kuchibhatla M, Tulsky JA, Johnson KS. Association of hospice patients' income and care level with place of death. JAMA Intern Med. 2013;173(6):450–6.
Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med. 1998;158(4):383–90.
van der Maaden T, de Vet HC, Achterberg WP, et al. Improving comfort in people with dementia and pneumonia: a cluster randomized trial. BMC Med. 2016;14(1):116.
van der Maaden T, van der Steen JT, de Vet HC, Hertogh CM, Koopmans RT. Prospective observations of discomfort, pain, and Dyspnea in nursing home residents with dementia and pneumonia. J Am Med Dir Assoc. 2016;17(2):128–35.
Yale New Haven Health Services Corporation/Center for Outcomes Research and Evaluation. Risk-Adjustment Models for AMI and HF 30-Day Mortality. Prepared for the Center for Medicare and Medicaid Services: 2005.
Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. 2001;345(20):1435–43.
Gade G, Venohr I, Conner D, et al. Impact of an inpatient palliative care team: a randomized control trial. J Palliat Med. 2008;11(2):180–90.
Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733–42.
Brumley R, Enguidanos S, Jamison P, et al. Increased satisfaction with care and lower costs: results of a randomized trial of in-home palliative care. J Am Geriatr Soc. 2007;55(7):993–1000.
Bakitas M, Lyons KD, Hegel MT, et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: the project ENABLE II randomized controlled trial. JAMA. 2009;302(7):741–9.
Han B, Remsburg RE, McAuley WJ, Keay TJ, Travis SS. National trends in adult hospice use: 1991-1992 to 1999-2000. Health Aff (Millwood). 2006;25(3):792–9.
Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA. 1997;278(23):2080–4.
Fisher ES, Wennberg JE, Stukel TA, Sharp SM. Hospital readmission rates for cohorts of Medicare beneficiaries in Boston and new haven. N Engl J Med. 1994;331(15):989–95.
Say JB. A treatise on political economy. Philadelphia: Grigg, Elliott & co.; 1848.
Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending. Part 1: the content, quality, and accessibility of care. Ann. Intern. Med. 2003;138(4):273–87.
Barnato AE, Herndon MB, Anthony DL, et al. Are regional variations in end-of-life care intensity explained by patient preferences?: a study of the US Medicare population. Med Care. 2007;45(5):386–93.
Walkey AJ, Weinberg J, Wiener RS, Cooke CR, Lindenauer PK. Association of do-not-Resuscitate Orders and Hospital Mortality Rate among Patients with Pneumonia. JAMA Intern Med. 2016;176(1):97–104.
Acknowledgements
The authors would like to thank Theodore G. Lieu for his feedback and attention.
Funding
The study detailed in this manuscript was performed without any sources of funding to declare.
Availability of data and materials
The datasets analyzed during in the course of this study are publicly available at: https://data.medicare.gov/.
Author information
Authors and Affiliations
Contributions
Contributions to manuscript: Conception (SMB, SL), data acquisition (SL), data analysis (SL, ELW, IS, VN, SMB), writing manuscript (SL, SMB), revising manuscript for important intellectual content (SL, ELW, SJB, IS, JO, VN, SMB), approval of final copy (SL, ELW, SJB, IS, JO, VN, SMB). SL had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
As this study analyzed publicly available data and did not involve any patient-level information, it was exempted (as per 45 CFR 46.101(b)(4)) from review by the Intermountain Healthcare Institutional Review Board.
Consent for publication
No patient-level information is contained in this manuscript, therefore no consent has been obtained.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Online Data Supplement. Table S1. Chronic conditions in the dartmouth atlas chronic illness cohort. Table S2. Inpatient quality indicators collected by the center for medicare and medicaid services, 2012. Table S3. Hospital characteristics by quantile of hospice utilization. Table S4. Quantile regression of heart failure 30-day mortality rates. Table S5. Quantile regression of heart failure 30-day readmission rates. Table S6. Pneumonia mortality quantile regression detailed results. Table S7. Pneumonia readmission quantile regression detailed results. Table S8. Heart failure mortality quantile regression detailed results. Table S9. Heart failure readmission quantile regression detailed results. Table S10. Pneumonia mortality multi-level model. Table S11. Pneumonia readmission multi-level model. Table S12. Heart failure mortality multi-level model. Table S13. Heart failure readmission multi-level model. (DOCX 42 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lah, S., Wilson, E.L., Beesley, S. et al. Association of hospice utilization and publicly reported outcomes following hospitalization for pneumonia or heart failure: a retrospective cohort study. BMC Health Serv Res 18, 12 (2018). https://doi.org/10.1186/s12913-017-2801-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-017-2801-3