
Abstract
Background
Bone stress fractures are overuse injuries commonly encountered in sports and military medicine. Some fatigue fractures lead to morbidity and loss of active, physically-demanding training days. We evaluated the incidence, anatomical location, risk factors, and preventive measures for fatigue fractures in young Finnish male conscripts.
Methods
Five cohorts of 1000 men performing military service, classified according to birth year (1969, 1974, 1979, 1984, 1989), were analysed. Each conscript was followed for his full military service period (180 days for conscripts with rank and file duties, 270 days for those with special training, 362 days for officers and highly trained conscripts). Data, including physical activity level, were collected from a standard pre-information questionnaire and from the garrisons’ healthcare centre medical reports. Risk factor analysis included the conscripts’ service class (A, B), length of military service, age, height, weight, body mass index, smoking, education, previous diseases, injuries, and subjective symptoms, as well as self-reports of physical activity before entering the service using a standard military questionnaire.
Results
Fatigue fractures occurred in 44 (1.1%) of 4029 men, with an incidence of 1.27 (95% confidence interval: 0.92–1.70) per 1000 follow-up months, and mostly (33/44, 75%) occurred at the tibial shaft or metatarsals. Three patients experienced two simultaneous stress fractures in different bones. Most fatigue fractures occurred in the first 3 months of military service. Conscripts with fatigue fractures lost a total of 1359 (range 10–77) active military training days due to exemptions from duty. Conscripts reporting regular (> 2 times/week) physical activity before entering the military had significantly fewer (p = 0.017) fatigue fractures. Regular physical activity before entering the service was the only strong explanatory, protective factor in the model [IRR = 0.41 (95% CI: 0.20 to 0.85)]. The other measured parameters did not contribute significantly to the incidence of stress fractures.
Conclusion
Regular and recurrent high-intensity physical activity before entering military service seems to be an important preventive measure against developing fatigue fractures. Fatigue fractures should be considered in conscripts seeking medical advice for complaints of musculoskeletal pain, and taken into consideration in planning military and other physical training programs.
Similar content being viewed by others


Background
Intense or recently intensified physical activity can lead to stress fractures, overuse injuries that are commonly encountered in sports and military medicine. Stress fractures commonly occur in long-distance runners, dancers, and other athletes, as well as in military trainees and soldiers [1,2,3]. Stress fractures are generally classified as either fatigue fractures, which occur in normal bone due to loading with abnormal forces, or insufficiency fractures, which occur in abnormal bone after loading with normal forces [1,2,3].
The risk of fatigue fracture is often related to the amount of physical activity, such as running, marching with loads, and walking [4, 5]. Not all factors that predispose to the development of stress fractures, however, are known. For example, some studies suggest a possible genetic predisposition for stress fractures [6, 7]. A low serum 25(OH)D concentration is also associated with bone fatigue fractures [8].
Bone stress injuries are categorized as either high-risk or low-risk, depending on the potential adverse sequelae and long-term morbidity [9]. A high percentage of patients with a displaced femoral neck fatigue fracture (high-risk) experience long-term morbidity, while patients with a non-displaced femoral neck fatigue fracture (low-risk) are not predisposed to long-term morbidity if dislocation is avoided [10, 11].
Stress fractures often lead to military discharge during basic training [12]. Recruits developing a stress fracture during their basic training period are at higher risk for stress fractures during subsequent training [13]. Such stress fractures may also increase the number of sick days, thereby disrupting military training. In the military, it is very important to understand not only the benefits of physical training, but also the short-term risks. Even relatively minor injuries might be costly in terms of lost training time and reduced combat readiness of soldiers [14]. Good physical fitness resulting from physical training is considered an essential element of readiness, but may lead to an increased incidence of training-related injuries.
Despite numerous studies of conscripts, recruits, and military personnel, population-based studies are required to better elucidate the incidence and risk factors for developing stress fractures. In the present cohort study, we evaluated the incidence, risk factors, and consequences of fatigue fractures, as well as the effectiveness of applied preventive measures among male conscripts during their compulsory military service period in Finland.
Methods
All Finnish males are required to serve in the military, with approximately 80% of each generation performing their service annually. Each year in January or July, new groups of conscripts begin their training. The majority of conscripts fulfil their service requirements at 19 to 20 years of age, although the age ranges from 18 to 29. The military training requirement is 180 days for conscripts with rank and file duties, 270 days for those with special training, and 362 days for officers and highly trained conscripts.
Subjects of the present study were 5000 conscripts randomly selected from the Finnish population registry, 1000 each born in 1969, 1974, 1979, 1984, or 1989, that were compared with each other over time. Military service documents were confirmed for 4327 of the men; of these, 298 were excluded because of a change in the service selection after entering the military or discharge for health reasons. Data for 4029 men were thus included in the analysis. The study received approval from the Institutional Review Board of the Finnish Defence Forces and the Ethics Committee of Helsinki University Hospital (267/13/03/09).
Basic training lasts 8 weeks and is intended to prepare the conscripts both mentally and physically for the military. Instruction is provided regarding the basic knowledge, performance, and skills required for military service. Physical training accounts for an average of ~ 17 h per week and includes combat skills, marching, and other physically demanding training such as close-order drills. Sport-related physical training (SRPT) accounts for ~ 6.5 h per week. Physical training proceeds progressively mainly through SRPT to help conscripts reach their maximal performance capacity by the end of the military service period. To reduce the risk of stress injuries while ramping up the physical training load, training is lightest during the first 2–6 weeks of training and individualized as much as possible [15,16,17]. SRPT is increased to support physical activity loading in the middle 8 weeks of service when there are fewer physically demanding training activities. In the troop training phase (latter 8 weeks), additional physical loading is provided by combat exercises and combat shooting camps, which often last several days at a time, and exercise training is intended mainly to promote recovery and mental relaxation.
Military training requires carrying heavy loads, such as combat dress and gear weighing ~ 25 kg, personal weapons, and other required equipment. The SRPT and physical training demands during the earlier phases help conscripts to cope with the greater demands of battlefield training and to increase their resistance to stress injury. Details of the basic training are available elsewhere [18].
Prior to entering military service, the Finnish Defence Forces require all conscripts to complete a pre-information questionnaire regarding socio-economic factors, health self-assessment, baseline health behaviour, school success, education level, father’s occupation, urbanization ranking of place of residence, physical activity level, prior sporting activities, sports club membership, participation in competitive sports, significant health factors, previous sports injuries, orthopaedic surgery, regular medication, chronic disease, impairment or disability, and presence of pain in seven different anatomic regions in the last month. Additionally, the questionnaire includes questions about the use of tobacco and alcohol, and frequency of drunkenness. Conscripts are asked how they think they compare with similar age mates and what they think about the physical demands placed on a soldier. The details of the questionnaire were reported previously [19,20,21,22,23]. All conscripts who participated in the present study served as either Class A (full combat or field troop training) or Class B (lightened or service training) [24].
Any visit to the garrison health care centre by the conscripts to seek medical advice was coded according to International Classification of Diseases (ICD)-9 or ICD-10 diagnosis codes indicating stress fracture. Only fatigue fractures were included in the present analysis. For each visit to the garrison health care centre, the medical reports were reviewed and the following data were recorded: examination date, symptoms, diagnosis, and resulting exemptions from duty. In all but one case, a plain radiograph was obtained to confirm the diagnosis. In our institution, when the diagnosis of stress fracture is uncertain on the basis of a plain radiograph, scintigraphy or magnetic resonance imaging (MRI) is performed. The imaging modalities and diagnostic criteria remained the same for the entire study.
Statistical analysis
The results are provided in the tables as means with standard deviations, and reported in the text as absolute and relative (%) counts. The t-test and chi-square test were applied to analyse the significance of differences between groups. Statistical analysis of the time-to-event was performed using the product-limit approach by applying the bootstrap 95% confidence interval [CI] of the cumulative incidence function. A multivariable forward stepwise Poisson regression model was used to determine the independent effect of fatigue fractures. The Poisson regression model was tested using the goodness-of-fit test and assumptions of overdispersion in the Poisson model were tested using the Lagrange multiplier test. Analyses were performed using the Stata 14.1, StataCorp LP (College Station, TX, USA) statistical package.
Results
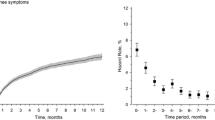
Fatigue fractures were detected in 44 (1.1%) of the study population (n = 4029 men; Tables 1 and 2). The incidence of fatigue fractures during military service was 1.27 (95% CI: 0.92–1.70) per 1000 follow-up months (Fig. 1). According to the medical reports, one of the stress fractures was diagnosed 1 week prior to beginning military service. None of conscripts in the study developed insufficiency fractures. Diagnosis was based on clinical examination (patient history and palpable tender bony mass) alone in 1 case; clinical and radiological investigation in 38 cases; clinical findings, plain radiographs, and MRI in 2 cases; and clinical findings, plain radiographs, and scintigraphic examination in 3 cases. Thus, in addition to radiographs, MRI or scintigraphy was needed to confirm the diagnosis in five cases.

Cumulative incidence of stress fractures during military service
The incidence was similar among the different age cohorts, although the prevalence tended to increase slightly in the two most recent cohorts (Fig. 2). The age cohorts did not differ significantly in the incidence of fatigue fractures (p = 0.21). All 44 fatigue fractures were located in the lower extremities (Fig. 3). The majority of fatigue fractures, 33 (75%) were located in the tibial shaft or metatarsals. In three patients, two simultaneous stress fractures were detected: one had both tibial and metatarsal fatigue fractures, another had bilateral fatigue fractures in the upper part of the femoral shaft, and a third had a femoral shaft fracture and a fatigue fracture of the calcaneal bone (Table 2). Most fatigue fractures occurred within the first 4 months of military service (Fig. 1).

Occurrence of fatigue fractures. Birth cohorts did not differ significantly (p = 0.21)

Anatomical location of stress fractures in lower extremities
Conscripts with fatigue fractures lost a total of 1359 (range 10–77) active military training days due to exemptions from duty. Diagnosis of fatigue fracture led to reclassification by the garrison physician of two conscripts serving in Class A (full combat or field troop training) to Class B conscripts (lightened or service training). In addition, three conscripts were classified as Class E conscripts; i.e., military service had to be discontinued until a physician deemed them capable of completing their remaining military service.
Conscripts who reported regular (> 2 times/week) physical activity (i.e., physical exercise causing sweating and breathlessness) before entering military service had significantly fewer bone fatigue fractures (p = 0.017, Table 1). Other measured parameters, such as body mass index, did not significantly affect the incidence of stress fractures. All of the variables shown in Table 1 were included in the multivariate forward Poisson regression model (Table 3), and only physical activity was a significant explanatory variable [IRR = 0.41 (95% CI: 0.20 to 0.85)].
Discussion
The findings of the present study suggest that engaging in highly physical activity, i.e., physical exercise causing sweating and breathlessness, more than twice a week before entering military service, protects young adult men from fatigue fractures during military service. To the best of our knowledge, this is the first report that regular physical activity prior to entering military service diminishes the incidence of fatigue fractures in young adult men during military service. Thus, engaging in regular, continuous, highly physical activity, before entering military service appears to be an important preventive measure that should be emphasised.
The low incidence of fatigue bone fractures, 1.1%, in the present cohort study indicates that the physical training load of the study population was not too heavy for the bones of a large majority of the conscripts. According to recent reports, the incidence of stress fractures in military recruits or conscripts ranges between 1.6 and 5.0% [25,26,27]. The low incidence of stress fractures in the present study indicates that the physical training level during compulsory military service was not too strenuous. Stress fractures should be considered, however, when conscripts present to the clinic with complaints of musculoskeletal pain, and taken into account when planning military and other physical training programs.
In the present study, conscripts suffering from fatigue fractures lost a total of 1359 (range 10–77) active military training days due to exemptions from duty. Stress fractures also caused service class changes. Stress fractures in athletes and military trainees results in a loss of active training days, and may be associated with adverse consequences and long-term morbidity [8, 28]. Physicians treating military trainees should keep these conditions in mind when military trainees complain of musculoskeletal pain. Some earlier epidemiologic studies suggested that the incidence of stress fractures can be reduced by altering modifiable risk factors of stress fractures, such as training volume, running distance, and possibly the use of shock-absorbent insoles in military boots [29, 30].
Our study has a number of strengths. First, we analysed five large age cohorts resulting in a total 4029 conscripts. The 5-year interval between the cohorts allowed us to evaluate the incidence over time. Furthermore, the medical examination and treatment in military health care centres and military hospitals was consistent for every conscript according to the policy of the Finnish Defence Forces. The present study also has some limitations. The present study is a registry-based study, and thus does not allow for exploration of theoretical or biological explanations for the findings. Only MRI can reveal the early stages of a stress fracture, i.e., bone pathology. According to the standard policy of the Finnish Defence Forces, MRI was not used to identify low-risk stress injuries, such as those in the metatarsal bones, because they can usually be detected on plain radiography. The use of MRI to evaluate every clinically suspicious bone stress injury would likely increase the accuracy of the diagnosis of stress fractures and reveal more bone stress injuries, but this would not reflect normal clinical practice for examining and treating fatigue fractures.
The majority (75%) of fatigue fractures detected in the present cohort study were located in the tibial shaft or metatarsals. This finding is consistent with those of previous studies of both Finnish athletes and conscripts [31, 32]. In a previous study of US Marine Corps recruits, bone stress injuries were less commonly detected in the pelvis, hip, thigh, and knee [33]. In running athletes, metatarsal shaft stress fractures are the most common type, representing up to 20% of stress fractures in the athletic population [34]. These fractures reportedly account for 38% of all stress fractures of the lower limb [12]. Among soldiers, the anatomical distribution of stress fractures differs for Israeli elite troops, with a higher incidence of tibial and femoral stress fractures during the first and second phases of training, and a higher incidence of metatarsal stress fractures in the third phase [35].
Conclusions
The main finding of the present study is that highly physical activity, physical exercise causing sweating and breathlessness more than twice a week before entering military service may protect young adult men from fatigue fractures. Thus, regular and recurrent high-intensity physical activity before entering military service seems to be an important preventive measure against developing fatigue fractures. Engaging in regular continuous highly physical activity before entering military service should be encouraged and emphasised.
Abbreviations
- ICD:
-
International Classification of Diseases
- SRPT:
-
Sport-related physical training
References
Pegrum J, Crisp T, Padhiar N. Diagnosis and management of bone stress injuries of the lower limb in athletes. BMJ. 2012;344:e2511. https://doi.org/10.1136/bmj.e2511.
Anderson MW, Greenspan A. Stress fractures. Radiology. 1996;199:1–12.
Daffner RH, Pavlov H. Stress fractures: current concepts. AJR Am J Roentgenol. 1992;159:245–52.
Jones BH, Hauschild VD. Physical training, fitness, and injuries: lessons learned from military studies. J Strength Cond Res. 2015;29(Suppl. 11:S57–64.
Knapik JJ, Graham BS, Rieger J, Steelman R, Pendergrass T. Activities associated with injuries in initial entry training. Mil Med. 2013;178(5):500–6.
Korvala J, Hartikka H, Pihlajamäki H, Solovieva S, Ruohola JP, Sahi T, Barral S, Ott J, Ala-Kokko L, Männikkö M. Genetic predisposition for femoral neck stress fractures in military conscripts. BMC Genet. 2010;11:95.
Varley I, Greeves JP, Sale C, Friedman E, Moran DS, Yanovich R, Wilson PJ, Gartland A, Hughes DC, Stellingwerff T, Ranson C, Fraser WD, Gallagher JA. Functional polymorphisms in the P2X7 receptor gene are associated with stress fracture injury. Purinergic Signal. 2016;12:103–13.
Ruohola JP, Laaksi I, Ylikomi T, Haataja R, Mattila VM, Sahi T, Tuohimaa P, Pihlajamäki H. Association between serum 25(OH)D concentrations and bone stress fractures in Finnish young men. J Bone Miner Res. 2006;21:1483–8.
Harmon KG. Lower extremity stress fractures. Clin J Sport Med. 2003;13:358–64.
Pihlajamäki HK, Ruohola JP, Kiuru MJ, Visuri TI. Displaced femoral neck fatigue fractures in military recruits. J Bone Joint Surg Am. 2006;88:1989–97.
Pihlajamäki HK, Ruohola JP, Weckström M, Kiuru MJ, Visuri TI. Long-term outcome of undisplaced fatigue fractures of the femoral neck in young male adults. J Bone Joint Surg Br. 2006;88:1574–9.
Waterman BR, Gun B, Bader JO, Orr JD, Belmont PJ Jr. Epidemiology of lower extremity stress fractures in the United States military. Mil Med. 2016;181(10):1308–13.
Milgrom C, Giladi M, Chisin R, Dizian R. The long-term followup of soldiers with stress fractures. Am J Sports Med. 1985;13(6):398–400.
Jones BH, Cowan DN, Tomlinson JP, Robinson JR, Polly DW, Frykman PN. Epidemiology of injuries associated with physical training among young men in the army. Med Sci Sports Exerc 1993;25(2):197-203.
Jones BH, Knapik JJ. Physical training and exercise-related injuries. Surveillance, research and injury prevention in military populations. Sports Med. 1999;27(2):111–25.
Rosendal L, Langberg H, Skov-Jensen A, Kjaer M. Incidence of injury and physical performance adaptations during military training. Clin J Sport Med. 2003;13(3):157–63.
Mattila VM, Niva M, Kiuru M, Pihlajamäki H. Risk factors for bone stress injuries: a follow-up study of 102,515 person-years. Med Sci Sports Exerc. 2007;39(7):1061–6.
Santtila M. Effects of added endurance or strength training on cardiovascular and neuromuscular performance of conscripts during the 8-week basic training period. In: studies in sport, physical education and health 146, 2010, University of Jyväskylä, Finland.
Frilander H, Miranda H, Mutanen P, Martelin T, Pihlajamäki H, Viikari-Juntura E. Trends in musculoskeletal disorders and related health care utilization among conscripts in Finland, 1967-2006. Mil Med. 2012;177:1069–74.
Mattila VM, Sillanpää P, Visuri T, Pihlajamäki H. Incidence and trends of low back pain hospitalisation during military service--an analysis of 387,070 Finnish young males. BMC Musculoskelet Disord. 2009;10:10.
Parkkari J, Taanila H, Suni J, Mattila VM, Ohrankämmen O, Vuorinen P, Kannus P, Pihlajamäki H. Neuromuscular training with injury prevention counselling to decrease the risk of acute musculoskeletal injury in young men during military service: a population-based, randomised study. BMC Med. 2011;9:35.
Taanila H, Hemminki AJ, Suni JH, Pihlajamäki H, Parkkari J. Low physical fitness is a strong predictor of health problems among young men: a follow-up study of 1411 male conscripts. BMC Public Health. 2011;11:590.
Pihlajamäki HK, Parviainen MC, Kautiainen H, Kiviranta I. Incidence and risk factors of exercise-related knee disorders in young adult men. BMC Musculoskelet Disord. 2017;18(1):340.
Multimäki P, Parkkola K, Sourander A, Haavisto A, Nikolakaros G, Helenius H. Military fitness class of Finnish 18-year-old men--prediction of military fitness class at call-up with the YASR and sociodemographic factors. Soc Psychiatry Psychiatr Epidemiol. 2005;40:57–63.
Armstrong DW 3rd, Rue JP, Wilckens JH, Frassica FJ. Stress fracture injury in young military men and women. Bone. 2004;35(3):806–16.
Lappe J, Davies K, Recker R, Heaney R. Quantitative ultrasound: use in screening for susceptibility to stress fractures in female army recruits. J Bone Miner Res. 2005;20(4):571–8.
Taanila H, Suni J, Pihlajamäki H, Mattila VM, Ohrankämmen O, Vuorinen P, Parkkari J. Aetiology and risk factors of musculoskeletal disorders in physically active conscripts: a follow-up study in the Finnish defense forces. BMC Musculoskeletal Disord. 2010;11:146.
Pentecost RL, Murray RA, Brindley HH. Fatigue, insufficiency, and pathologic fractures. JAMA. 1964;187:1001–4.
Jacobs JM, Cameron KL, Bojescul JA. Lower extremity stress fractures in the military. Clin Sports Med. 2014;33(4):591–613.
Jones BH, Thacker SB, Gilchrist J, Kimsey CD Jr, Sosin DM. Prevention of lower extremity stress fractures in athletes and soldiers: a systematic review. Epidemiol Rev. 2002;24(2):228–47.
Korpelainen R, Orava S, Karpakka J, Siira P, Hulkko A. Risk factors for recurrent stress fractures in athletes. Am J Sports Med. 2001;29:304–10.
Ruohola JP, Kiuru MJ, Pihlajamäki HK. Fatigue bone injuries causing anterior lower leg pain. Clin Orthop Relat Res. 2006;444:216–23.
Schneiders AG, Sullivan SJ, Hendrick PA, Hones BD, McMaster AR, Sugden BA, Tomlinson C. The ability of clinical tests to diagnose stress fractures: a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2012;42(9):760–71.
Rice H, Fallowfield J, Allsopp A, Dixon S. Influence of a 12.8-km military load carriage activity on lower limb gait mechanics and muscle activity. Ergonomics. 2017;60(5):649–56.
Finestone A, Milgrom C, Wolf O, Petrov K, Evans R, Moran D. Epidemiology of metatarsal stress fractures versus tibial and femoral stress fractures during elite training. Foot Ankle Int. 2011;32(1):16–20.
Acknowledgements
Data collection for the present study was supported by the Headquarters of Finnish Defence Forces, Helsinki, Finland as well as by the Centre for Military Medicine, Helsinki and Viitasaari, Finland.
Funding
This study was financially supported by the Competitive State Research Financing of Seinäjoki Central Hospital and the Finnish Scientific Advisory Board for Defense.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available because they were retrospectively obtained from institutional registries and records that are not available for an open access repository. The data are available from the corresponding author upon reasonable request.
Author information
Authors and Affiliations
Contributions
HP planned, conducted and reported this research with IK. HP was the principal writer of the manuscript. HKy, MP and IK contributed to writing and reviewing the manuscript. MP took part in data collection and interpretation. HKa contributed to planning of this research and performed all statistical analyses. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee of the Hospital District of Helsinki and Uusimaa approved the study (267/13/03/09). The current study was based on registry data and no clinical patients were enrolled; therefore, informed consent of the patients was not required. Approval to use the data was granted by Institutional Review Board of the Finnish Defence Forces.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Pihlajamäki, H., Parviainen, M., Kyröläinen, H. et al. Regular physical exercise before entering military service may protect young adult men from fatigue fractures. BMC Musculoskelet Disord 20, 126 (2019). https://doi.org/10.1186/s12891-019-2513-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-019-2513-4