
Abstract
Background
Non-cemented acetabular cup components demonstrated different clinical performance depending on their surface texture or bearing couple. However, clinical osseointegration needs to be proved for each total joint arthroplasty (TJA) design. Aim of this study was to detect the in vivo migration pattern of a non-cemented cup design, using model-based roentgen stereophotogrammetric analysis with elementary geometrical shape models (EGS-RSA) to calculate early cup migration.
Methods
Interchangeable applicability of the model-based EGS-RSA method next to gold standard marker-based RSA method was assessed by clinical radiographs. Afterwards, in vivo acetabular cup migration for 39 patients in a maximum follow up of 120 months (10 years) was calculated using model-based EGS-RSA.
Results
For the axes with the best predictive capability for acetabular cup loosening, mean (±SD) values were calculated for migration and rotation of the cup. The cup migrated 0.16 (±0.22) mm along the cranio-caudal axis after 24 months and 0.36 (±0.72) mm after 120 months, respectively. It rotated − 0.61 (±0.57) deg. about the medio-lateral axis after 24 months and − 0.53 (±0.67) deg. after 120 months, respectively.
Conclusions
Interchangeable applicability of model-based EGS-RSA next to gold standard marker-based RSA method could be shown. Model-based EGS-RSA enables an in vivo migration measurement without the necessity of TJA specific surface models. Migration of the investigated acetabular cup component indicates significant migration values along all the three axes. However, migration values after the second postoperative year were within the thresholds reported in literature, indicating no risk for later aseptic component loosening of this TJA design.
Similar content being viewed by others


Background
The medical intervention for hip osteoarthritis finally ends with a surgical treatment of the affected joint by total hip arthroplasty (THA) [1]. Forecasts for primary and revision THA procedures predict an increasing case number [2]. However, THA presents an established orthopaedic intervention with a reported survivorship greater than 95% at 10-year and 80% at 25-year follow-up [3]. National registries [4] and clinical studies [5, 6] indicate that THA survivorship is affected by several factors like total joint arthroplasty (TJA) design, bearing couple or surface texture of non-cemented designs. In summary, THA failure most often is caused by aseptic loosening [3, 4, 7] and periprosthetic joint infection [8, 9], both associated with an important economic impact [10].
According THA, the interpretation of survivorship rates must be performed separately for femoral stem and acetabular cup components. For instance Hallan et al. [11] reported a good survivorship at 15-years follow-up for non-cemented femoral stems, whereas non-cemented metal-backed acetabular cup components revealed poor clinical outcome in comparison to cemented all-polyethylene components. Non-cemented metal backed cups showed different clinical outcomes, i.e. grit-blasted and hydroxyapatite-coated acetabular cups indicate a three times higher risk of revision than hydroxyapatite-coated, threaded acetabular cups in cause of aseptic loosening [11]. Palomäki et al. [12] reported data for uncemented cups of the second generation, collected within the Finnish Arthroplasty Register, showing survival rates similar to cemented treatment. However, these results based on mid-term data, longtime data for these cups were still necessary.
The clinical performance of non-cemented coated TJA components in general depends on several factors predicting the bony osseointegration: (i) properties of the implant surface likewise surface texture, coating layer thickness and applied pore size, (ii) host bone quality, (iii) surgical site preparation, (iv) preoperative loading conditions and (v) preventing initial and chronic infections [13, 14].
If the bony osseointegration of a TJA design fails, loosening of the implant will occur. Gold standard method to assess the in vivo fixation of TJA components presents Roentgen Stereophotogrammetric Analysis (RSA) [15, 16]. It is important to monitor TJA fixation within preclinical trials using gold standard methods, since worst case scenarios of clinical TJA failure – likewise the Boneloc cement disaster within the early 1990s – could be avoided [17,18,19,20] and the migration pattern of TJA is affected by the implant design and its fixation philosophy [21, 22]. Using RSA, early implant migration within the first two postoperative years could be detected, which has been shown to correlate well with later aseptic loosening of femoral stems [23] and acetabular cups [24, 25].
Several variations of RSA exist, i.e. using markers attached to the implant (marker-based RSA) or a surface model of the investigated TJA components (model-based RSA) to calculate early implant migration [20, 26]. The interchangeable applicability of the both methods has been demonstrated [27,28,29]. Model-based RSA using elementary geometrical shape (EGS-RSA) is an approach which uses geometrical bodies likewise spheres or cylinders to calculate migration by rigid body kinematics instead of implant specific surface models [30,31,32,33].
Nieuwenhuijse et al. [24] identified thresholds for micromotion of a cemented acetabular cup to distinguish between safe or at risk implants. This research group found cranial migration > 1.76 mm or sagittal rotational migration > 2.53 deg. within the first two postoperative years to be risk factors for subsequent aseptic component failure of acetabular cups. Although a cemented cup was investigated, the authors state that the results of their study should be independent of the fixation method [24]. In accordance with this statement, Pijls et al. [25] reported in a systematic review a similar threshold for cemented as well as uncemented cups. A mean cranial migration of 0.2 mm or less was classified as acceptable, with revision rates of < 5% after 10 years.
Aim of this study is to determine the in vivo migration behavior of a non-cemented titanium cup (Phoenix cup; Peter Brehm GmbH, Weisendorf, Germany) for 10 years, using model-based EGS-RSA. The authors hypothesize that no translational migration > 1.7 mm in cranial direction or rotational migration > 2.5 deg. around anterior-posterior axis is detectable within a two-year follow-up. Thus, the authors expect good ten-year performance of the cup with a revision rate of less than 5% caused by aseptic implant failure.
Methods
Retrospectively, out of a former classical marker-based RSA study of 50 patients (Fig. 1a), RSA radiographs were analysed using model-based RSA approach with a hemisphere elementary geometrical shape surface model (Fig. 1b). Marker-based migration calculation was not possible due to implant-marker occlusion problems (in 43 of 50 cases) within the RSA radiographs (Fig. 1c, d). But using a model-based RSA approach with EGS models, migration calculation was possible in 39 of 50 cases.

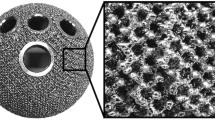
a Non-cemented titanium (TiAl6V4) acetabular cup component, composed of a cylinder attached to the rim of a spherical segment, covered by TiRC coating (Titan Rough Coating) with a surface layer thickness of approximately 300 μm, a surface roughness of Rz = 100–150 μm and four additional attached and pairwise-arranged tantalum markers for marker-based RSA measurements. This special RSA cup was in accordance with legal rules. b For model-based EGS-RSA approach, a hemisphere model with a curvature radius and implant height according to the technical drawings of the investigated cup component was generated. The local EGS model coordinate system was set to the centre of gravity. All axes were aligned perpendicular to each other. c Left image of an RSA reference radiographic image pair with three of four visible implant markers. Implant marker no. 4 occluded by the implant itself within the RSA image. d Occluded implant marker problem for marker-based RSA approach. Left image out of the same patient follow up series, with occluded implant markers no. 3 (x) and 4. As at least three implant markers were necessary for marker-based RSA approach, for this RSA image pair a migration calculation was not possible
Surgical treatment
All included patients showed clinical signs of hip osteoarthritis and were treated by primary THA with a non-cemented titanium acetabular cup component (Phoenix cup, Peter Brehm GmbH, Weisendorf, Germany) (Fig. 1a). The Phoenix cup is a hemispherical press-fit cup with a titanium rough coating and a surface roughness of Rz 100–150 μm. A single well skilled surgeon performed all the surgeries, using a direct lateral approach. For each patient six to eight CE-certified tantalum markers (diameter: 1.0 mm) were inserted during surgery to the implant surrounding acetabular bone.
RSA measurement setup
A uniplanar RSA setup consisting of two x-ray tubes (Multix RD 82477–01 Vertix ACS and Mobilett Plus; Siemens, Berlin, Germany) was used. Both x-ray tubes were positioned at an angle of 40 deg. in relation to each other and 1.40 m above the calibration cage (Umea Cage 43 calibration cage, RSA BioMedical Innovations AB, Umea, Sweden). The THA treated hip joints of the supine patients were arranged within the intersection of the two x-ray pathways. Accuracy of this RSA setup was determined using a custom made phantom model (Table 1), as double examinations were declined by the ethical committee to minimize x-ray exposure of the patients.
Measurement protocol
Reference RSA image pairs were taken within the first two postoperative days before load bearing of the treated hip joint. Follow-up examinations were performed at six, 12 weeks, six, 12, 24, 60 and 120 months postoperatively.
The RSA image pairs of all patients (n = 50) were analysed using model-based RSA software package (MBRSA 3.4, MEDIS specials, Leiden, Netherlands) and custom made EGS models of the investigated acetabular cup component (Fig. 1b). Standard thresholds were applied to verify the quality of the calibration procedure and the rigid body error of the detected bone markers of the acetabular bone [34,35,36]. If all quality criteria were fulfilled in the image pairs, these datasets were included for statistical analysis, indicating that no artefacts or analysis errors were present. Only patients with at least one follow-up at 2 years, 5 years or 10 years were included.
RSA image analyses were performed in accordance with the recommendations of the RSA ISO standard 16,087:2013(E) [36] and the guidelines proposed by Valstar et al. [34]. All patients gave their written informed consent to study participation and to data publication. The Ethics Committee of Friedrich-Alexander-Universität Erlangen-Nürnberg approved the study (registration no. 1.077).
Statistics
Calculated migrations of clinical data were presented as mean (±SD). An analysis of variance including Bonferroni correction was used to prove significant changes of migration values between the follow-ups. The level of significance was set to p < 0.05. Statistical analyses were performed using SPSS 24.0 (SPSS Inc., Chicago, Illinois, USA).
Results
Patient cohort
Within this retrospective analysis, 11 patients of the entire patient cohort (n = 50) had to be excluded due to technical errors (e.g. high rigid body error of the bone markers at the postoperative) (n = 4), death (n = 1), study exclusion for reasons unrelated to the implant (n = 4) or for unknown reasons (n = 2). In summary radiographs for 39 patients, which completely fulfilled analysis criteria for model-based EGS-RSA measurement were included. After the 2-years follow-up, 16 patients dropped out of the study for infirmity not related to the implant (n = 8) or for unknown reasons (n = 8), as it was not possible to contact the latter patients. After the 5-years follow-up, again five more patients got lost to the study for unknown reasons (Fig. 2).

Flowchart of dropouts and missing patients. Green boxes: attending patients on follow-up. Pale green boxes: patients missing the correspondent follow-up. Red boxes: final dropouts
The entire patient cohort (n = 39) consisted of 24 women and 15 men (18 left and 21 right hip replacements). The mean age of the patients at time of surgery was 67.2 (±9.5) years, ranging from 35.8 to 79.6 years.
Experimental accuracy of marker- and model-based EGS-RSA for the investigated cup component
Maximum bias (±SD) for marker-based RSA was − 0.03 (±0.06) mm (95% CI between < 0.01 and 0.22 mm) in cranio-caudal direction (y-axis), for model-based EGS-RSA, it was − 0.06 (±0.18) mm (95% CI between − 0.27 and 0.43 mm) along anterior-posterior direction (z-axis), for the both investigated relative motion set points of 0.5 mm and 1.5 mm (Table 1).
Clinical cup migration data
Highest mean (±SD) migrations were observable along medio-lateral direction (x-axis) with 0.29 (±0.52) mm at 60 months and along cranio-caudal direction (y-axis) with 0.36 (±0.27) mm at 120 months (Table 2). Rotational migration about the y-axis was not calculated according to axisymmetric implant geometry. For the remaining axes the highest rotation occurred around medio-lateral direction of − 0.61 (±0.57) deg. at 24 months follow-up (Table 2).
For the most predictable axis of acetabular cup loosening, migration along cranio-caudal axis increased continuously from 0.11 (±0.22) mm at 6 weeks up to 0.36 (±0.27) mm at 120 months.
In cranio-caudal direction significant migration values according to the reference follow-up examination were observable for the 6 months follow-up (p = 0.029), 12 months follow-up (p = 0.029), 24 months follow-up (p = 0.017) and 120 months follow-up (p < 0.001). However, for the 60 months follow-up (p = 0.114) no significant difference to the reference follow-up could be observed (Fig. 3a, Table 2). For rotation about medio-lateral axis a significant different mean (p = 0.034) compared to the reference follow up was observable at 24 months (Fig. 3b, Table 2). For remaining migrations and rotations, significance criteria were not fulfilled.

Calculated acetabular cup migration (a) along cranio-caudal direction [mm] and (b) about medio-lateral direction [deg] at six, 12 weeks, six, 12, 24, 60 and 120 months follow-up. The boxes represent 50% of included data (bound the 25th to 75th percentile) with the median (horizontal line), smallest and largest value (whisker bars) as well as outliers (circles) and extreme values (stars). Dotted horizontal lines indicate threshold for cranial (> 1.76 mm) acetabular cup migration according to Nieuwenhuijse et al. [24]
Discussion
Accuracy determined by using a phantom investigation showed better values for the marker-based RSA than for the model-based EGS-RSA method. However, both methods provided results within the range of RSA accuracy reported by Kärrholm [37], which is between 0.05 and 0.5 mm for translational migration. Thus, we consider that the loss of accuracy from using model-based EGS-RSA is acceptable for a clinical application of the methodology.
The clinical outcome of the investigated cup component indicates statistically significant migration according to the reference examination along the cranio-caudal axis at the 6 months (0.16 mm; p = 0.029), 12 months (0.16 mm; p = 0.029) and 24 months follow-up (0.17 mm; p = 0.017). At 120 months follow up, migration of the cup component increased significantly up to 0.36 (±0.27) mm (p < 0.001). It is important to note that in the first 24 months the observable maximum mean migration in cranial (0.11 mm) direction occurred within the first 6 weeks after surgery (Table 2). Afterwards a steady state mode of the detected migration was observable for the upcoming follow-up intervals within the first 5 years. Between five and 10 years the cup continued to migrate in cranial direction again by another 0.17 mm.
The only observable significant different rotation occurred around the medio-lateral axis at the 24 months follow-up (− 0.61 deg.; p = 0.034).
Two patients showed especially noticeable migration greater than 1.0 mm in the medial direction (Pat 1; 1.7 mm) and of approximately 1.0 mm in lateral direction (Pat 2) within the first 6 weeks, after which the cup appeared to stabilise up to the 24 months follow up (Fig. 4a). However, Pat 2 cup starts to migrate again in lateral direction after 24 months follow up. Conventional anterior-posterior radiographs indicate no clinical signs of loosening (e.g. radiolucent lines).

Calculated acetabular cup migration [mm] at six, 12 weeks, six, 12, 24, 60 and 120 months follow-up along (a) medio-lateral, b cranio-caudal and (c) anterior-posterior direction. d Mean ± SD value for each patient, classified at 24 months follow up according to Pijls et al. [25] as an acceptable cup (blue graph; migration < 0.2 mm represented by black dotted line) and cup at risk (green graph; migration between 0.2 mm and 1.0 mm represented by black dotted line). Red dotted line indicates threshold (> 1.76 mm) for cranial acetabular cups migration at risk according to Nieuwenhuijse et al. [24]
Some patients (n = 13 at 24 months; n = 11 at 120 months, including Pat 1) showed migration between 0.2 mm and 1.0 mm in cranial direction (Fig. 4b), however no cups were identified to migrate more than 1.0 mm. The maximum cranial migration value was observable after 6 weeks with 0.76 mm (Pat 1), which remained unchanged for this patient during the next follow-up investigations. Thus, this cup seems to have stabilised with no further migration in this direction.
In anterior-posterior direction one patient (Pat 3) had a migration value of − 1.28 mm at 6 weeks follow-up, which increased to > − 2.0 mm at the 24 months follow up (Fig. 4c).
Cranial migration is seen as a relevant predictive value for late aseptic loosening of acetabular cup components [24, 25, 38, 39]. In a systematic review, Pijls et al. [25] reported an average increase of 10% in the 10-year revision rate for every millimetre of cranial migration of an acetabular cup component. The authors suggested that inferior components could be identified by RSA within the first two postoperative years, thereby avoiding their widespread implementation. Furthermore, they provided proximal migration thresholds for acetabular cups, whereas cups with a mean cranial migration of 0.2 mm or less were classified as acceptable, with revision rates of < 5% after 10 years. In contrast, cups with a mean cranial migration of 1.0 mm or more were classified as unacceptable, with a > 5% risk for 10-year revision.
For the investigated cup component, a mean proximal migration of 0.17 mm occurred after two postoperative years (n = 36 patients at 24 months), which is less than the proposed threshold of 0.2 mm suggested by Pijls et al. [25]. In summary, 13 patients at 24 months were classified at risk (migration between 0.2 mm and 1.0 mm), no patient could be classified as unacceptable (migration > 1.0 mm). These results indicate good performance for the investigated cup component, according to suggestion of Pijls et al. [25]. As none of the followed implants had to be revised after 10 years, this study verifies the suggestions of Pijls et al. [25].
One limitation of this study was the absence of rotational measurements about the cranio-caudal axis. Due to technical restrictions of EGS-RSA, analysis of this rotational migration could not be conducted as the cup has an axis-symmetrical design. This is a well-known problem in model-based RSA [40]. Nonetheless, migration in cranial direction and rotation about the anterior-posterior axis could be calculated, which are the essential movements to predict later cup loosening [24, 25]. Current studies evaluate computed tomography (CT) as an alternative measurement tool to RSA to analyze implant migration. They describe comparable accuracy and precision values for CT-based methods, especially in experimental settings [41,42,43,44]. Moreover, CT-based migration measurement could handle some disadvantages of RSA: CT is available in almost every hospital, picture acquisition does not require a special setup or briefed personnel, migration in all directions can be calculated, and there is no problem of marker occlusion by the implant [45]. On the other hand, conventional CT examinations expose patients to higher radiation doses than stereoradiographs, but there is some evidence that a reduction of CT radiation dose does not impair the accuracy of migration analysis [42, 43]. However, there is still a lack of clinical trials and long-term examinations evaluating CT-based migration measurement. Besides, there are still some problems to deal with, as for example artifacts of metallic implants, the influence of soft tissue or the immobilization of patients during CT scanning [44]. In summary, CT-based methods need further validation before they can be considered as an alternative to gold standard RSA.
Another limitation of this study is the number of drop-outs. However, the drop-out rate is comparable to those of other RSA studies [23, 24, 46,47,48]. During the crucial period of the first 2 years, that are relevant for RSA-prognosis, eleven patients had to be excluded. The remaining number of 39 patients also complies with the RSA guidelines proposed by Valstar et al., who recommend a number of 15–25 patients for the special case of RSA studies [34].
Unfortunately, it is not possible to define prognostic migration thresholds out of the results, as there was no implant failure observable in 10 years of follow-up. However, the results confirm the above-mentioned thresholds of previous studies.
The migration pattern of the investigated acetabular cup component showed migration along all the three axes, particularly in medio-lateral and cranio-caudal direction. Migration along the latter mentioned direction is considered to be the most important prognostic factor for a later aseptic loosening but was still within acceptable limits according to Pijls et al. [25]. It would be interesting to follow the patients for a longer period in order to evaluate how the migration pattern of all axes will influence the long-term stability of the investigated non-cemented acetabular cup.
Conclusions
Model-based EGS-RSA enables an in vivo migration measurement of TJA components without the necessity of TJA specific surface models. The investigated acetabular cup component demonstrates significant differences for calculated migration values along the most predictable axis of acetabular cup loosening, migration along cranio-caudal axis with 0.17 (±0.24) mm at 24 months. However, the measured in vivo cup migration at 2 years of follow-up were within the acceptable thresholds reported in literature [24, 25]. For the cranio-caudal axis, migration continuously increased up to 0.36 (±0.27) mm at 120 months follow-up but is still within above mentioned thresholds. However, performed migration measurement by model-based EGS-RSA within this study highlights the importance and benefit of RSA for the evaluation of implants. There may be other possible applications in the future, such as the early detection of septic loosening of joint implants [49].
Abbreviations
- EGS - RSA:
-
Roentgen stereophotogrammetric analysis using elementary geometrical shape models
- CT:
-
Computed tomography
- EGS:
-
Elementary geometrical shapes
- RSA:
-
Roentgen stereophotogrammetric analysis
- SD:
-
Standard deviation
- THA:
-
Total hip arthroplasty
- TJA:
-
Total joint arthroplasty
References
Hochberg MC, Altman RD, Brandt KD, Clark BM, Dieppe PA, Griffin MR, Moskowitz RW, Schnitzer TJ. Guidelines for the medical management of osteoarthritis. Part I Osteoarthritis of the hip American College of Rheumatology. Arthritis Rheum. 1995;38(11):1535–40.
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–5.
Pivec R, Johnson AJ, Mears SC, Mont MA. Hip arthroplasty. Lancet. 2012;380(9855):1768–77.
Registry AOANJR: Annual Report 2016. 2016, 2017(11.04.2017).
Pakvis D, Luites J, van Hellemondt G, Spruit M. A cementless, elastic press-fit socket with and without screws. Acta Orthop. 2012;83(5):481–7.
Strom H, Kolstad K, Mallmin H, Sahlstedt B, Milbrink J. Comparison of the uncemented cone and the cemented Bimetric hip prosthesis in young patients with osteoarthritis: an RSA, clinical and radiographic study. Acta Orthop. 2006;77(1):71–8.
Chalmers PN, Sporer SM, Levine BR. Correlation of aspiration results with aseptic loosening in total hip arthroplasty. J Arthroplast. 2013;28(9):1671–6.
Portillo ME, Salvado M, Alier A, Sorli L, Martinez S, Horcajada JP, Puig L. Prosthesis failure within 2 years of implantation is highly predictive of infection. Clin Orthop Relat Res. 2013;471(11):3672–8.
Trampuz A, Zimmerli W. Prosthetic joint infections: update in diagnosis and treatment. Swiss Med Wkly. 2005;135(17–18):243–51.
Kurtz SM, Ong KL, Schmier J, Mowat F, Saleh K, Dybvik E, Karrholm J, Garellick G, Havelin LI, Furnes O, et al. Future clinical and economic impact of revision total hip and knee arthroplasty. J Bone Joint Surg Am. 2007;89(Suppl 3):144–51.
Hallan G, Dybvik E, Furnes O, Havelin LI. Metal-backed acetabular components with conventional polyethylene: a review of 9113 primary components with a follow-up of 20 years. J Bone Joint Surg Br. 2010;92(2):196–201.
Palomaki A, Lempainen L, Matilainen M, Eskelinen A, Remes V, Virolainen P, Makela KT. Survival of uncemented cups from a single manufacturer implanted from 1985 to 2013: Finnish arthroplasty register data. Arch Orthop Trauma Surg. 2017;137(3):311–20.
Muschler GF, Nakamoto C, Griffith LG. Engineering principles of clinical cell-based tissue engineering. J Bone Joint Surg Am. 2004;86-A(7):1541–58.
Isaacson BM, Jeyapalina S. Osseointegration: a review of the fundamentals for assuring cementless skeletal fixation. Orthop Res Rev. 2014;6:55–65.
Sundfeldt M, Carlsson LV, Johansson CB, Thomsen P, Gretzer C. Aseptic loosening, not only a question of wear: a review of different theories. Acta Orthop. 2006;77(2):177–97.
Valstar ER, HS Gill R. Radiostereometric analysis in orthopaedic surgery: editorial comment. Clin Orthop Relat Res. 2006;448:2.
Gebuhr P, Stentzer K, Thomsen F, Levi N. Failure of total hip arthroplasty with Boneloc bone cement. Acta Orthop Belg. 2000;66(5):472–6.
Furnes O, Lie SA, Havelin LI, Vollset SE, Engesaeter LB. Exeter and charnley arthroplasties with Boneloc or high viscosity cement. Comparison of 1,127 arthroplasties followed for 5 years in the Norwegian arthroplasty register. Acta Orthop Scand. 1997;68(6):515–20.
Riegels-Nielsen P, Sorensen L, Andersen HM, Lindequist S. Boneloc cemented total hip prostheses. Loosening in 28/43 cases after 3-38 months. Acta Orthop Scand. 1995;66(3):215–7.
Karrholm J, Gill RH, Valstar ER. The history and future of radiostereometric analysis. Clin Orthop Relat Res. 2006;448:10–21.
Acklin YP, Jenni R, Bereiter H, Thalmann C, Stoffel K. Prospective clinical and radiostereometric analysis of the Fitmore short-stem total hip arthroplasty. Arch Orthop Trauma Surg. 2016;136(2):277–84.
Kutzner KP, Freitag T, Donner S, Kovacevic MP, Bieger R. Outcome of extensive varus and valgus stem alignment in short-stem THA: clinical and radiological analysis using EBRA-FCA. Arch Orthop Trauma Surg. 2017;137(3):431–9.
Karrholm J, Borssen B, Lowenhielm G, Snorrason F. Does early micromotion of femoral stem prostheses matter? 4-7-year stereoradiographic follow-up of 84 cemented prostheses. J Bone Joint Surg Br. 1994;76(6):912–7.
Nieuwenhuijse MJ, Valstar ER, Kaptein BL, Nelissen RG. Good diagnostic performance of early migration as a predictor of late aseptic loosening of acetabular cups: results from ten years of follow-up with roentgen stereophotogrammetric analysis (RSA). J Bone Joint Surg Am. 2012;94(10):874–80.
Pijls BG, Nieuwenhuijse MJ, Fiocco M, Plevier JW, Middeldorp S, Nelissen RG, Valstar ER. Early proximal migration of cups is associated with late revision in THA: a systematic review and meta-analysis of 26 RSA studies and 49 survivalstudies. Acta Orthop. 2012;83(6):583–91.
Valstar ER, de Jong FW, Vrooman HA, Rozing PM, Reiber JH. Model-based roentgen stereophotogrammetry of orthopaedic implants. J Biomech. 2001;34(6):715–22.
Kaptein BL, Valstar ER, Stoel BC, Reiber HC, Nelissen RG. Clinical validation of model-based RSA for a total knee prosthesis. Clin Orthop Relat Res. 2007;464:205–9.
Hurschler C, Seehaus F, Emmerich J, Kaptein BL, Windhagen H. Comparison of the model-based and marker-based roentgen stereophotogrammetry methods in a typical clinical setting. J Arthroplast. 2009;24(4):594–606.
Seehaus F, Emmerich J, Kaptein BL, Windhagen H, Hurschler C. Experimental analysis of model-based roentgen Stereophotogrammetric analysis (MBRSA) on four typical prosthesis components. J Biomech Eng. 2009;131(4):041004.
Kaptein BL, Valstar ER, Spoor CW, Stoel BC, Rozing PM. Model-based RSA of a femoral hip stem using surface and geometrical shape models. Clin Orthop Relat Res. 2006;448:92–7.
Prins AH, Kaptein BL, Stoel BC, Nelissen RG, Reiber JH, Valstar ER. Handling modular hip implants in model-based RSA: combined stem-head models. J Biomech. 2008;41(14):2912–7.
Borlin N, Rohrl SM, Bragdon CR. RSA wear measurements with or without markers in total hip arthroplasty. J Biomech. 2006;39(9):1641–50.
Valstar ER, Spoor CW, Nelissen RG, Rozing PM. Roentgen stereophotogrammetric analysis of metal-backed hemispherical cups without attached markers. J Orthop Res. 1997;15(6):869–73.
Valstar ER, Gill R, Ryd L, Flivik G, Borlin N, Karrholm J. Guidelines for standardization of radiostereometry (RSA) of implants. Acta Orthop. 2005;76(4):563–72.
Soderkvist I, Wedin PA. Determining the movements of the skeleton using well-configured markers. J Biomech. 1993;26(12):1473–7.
Standardization IOf: International Standard ISO 16087:2013(E). Implants for surgery – Roentegen stereophotogrammetric analysis for the assessment of migration of orthopaedic implants. 2013, ISO 16087:2013(E).
Karrholm J. Roentgen stereophotogrammetry. Review of orthopedic applications. Acta Orthop Scand. 1989;60(4):491–503.
Karrholm J, Herberts P, Hultmark P, Malchau H, Nivbrant B, Thanner J. Radiostereometry of hip prostheses. Review of methodology and clinical results. Clin Orthop Relat Res. 1997;344:94–110.
Klerken T, Mohaddes M, Nemes S, Karrholm J. High early migration of the revised acetabular component is a predictor of late cup loosening: 312 cup revisions followed with radiostereometric analysis for 2-20 years. Hip Int. 2015;25(5):471–6.
Seehaus FEJ, Kaptein BL, Windhagen H, Hurschler C. Applicability of model-based RSA for an axis symmetric hip resurfacing prosthesis design. J Biomech. 2008;41:S38.
Boettner F, Sculco P, Lipman J, Renner L, Faschingbauer M. A novel method to measure femoral component migration by computed tomography: a cadaver study. Arch Orthop Trauma Surg. 2016;136(6):857–63.
Boettner F, Sculco PK, Lipman J, Saboeiro G, Renner L, Faschingbauer M. The effect of a low radiation CT protocol on accuracy of CT guided implant migration measurement: a cadaver study. J Orthop Res. 2016;34(4):725–8.
Broden C, Olivecrona H, Maguire GQ Jr, Noz ME, Zeleznik MP, Skoldenberg O. Accuracy and precision of three-dimensional low dose CT compared to standard RSA in acetabular cups: an experimental study. Biomed Res Int. 2016;2016:5909741.
Scheerlinck T, Polfliet M, Deklerck R, Van Gompel G, Buls N, Vandemeulebroucke J. Development and validation of an automated and marker-free CT-based spatial analysis method (CTSA) for assessment of femoral hip implant migration: in vitro accuracy and precision comparable to that of radiostereometric analysis (RSA). Acta Orthop. 2016;87(2):139–45.
Otten V, Maguire GQ Jr, Noz ME, Zeleznik MP, Nilsson KG, Olivecrona H. Are CT scans a satisfactory substitute for the follow-up of RSA migration studies of Uncemented cups? A comparison of RSA double examinations and CT datasets of 46 Total hip arthroplasties. Biomed Res Int. 2017;2017:3681458.
Wolf O, Mattsson P, Milbrink J, Larsson S, Mallmin H. The effects of different weight-bearing regimes on press-fit cup stability: a randomised study with five years of follow-up using radiostereometry. Int Orthop. 2012;36(4):735–40.
Budde S, Seehaus F, Schwarze M, Hurschler C, Floerkemeier T, Windhagen H, Noll Y, Ettinger M, Thorey F. Analysis of migration of the Nanos(R) short-stem hip implant within two years after surgery. Int Orthop. 2016;40(8):1607–14.
Nilsson KG, Theodoulou A, Mercer G, Quinn SJ, Krishnan J. Mid-term migration of a cementless, porous acetabular cup: a 5 year Radiostereometric analysis. J Orthop. 2017;14(4):454–60.
Sesselmann S, Hausotte T, Timmermann M, Liebsch G, Forst R, Trampuz A, Jacobsen A. Radiostereometric analysis as a need for early detection of septic loosening. EC Orthopaedics. 2015;2(3):87–94.
Acknowledgements
The present work was performed in partial fulfilment of the requirements for obtaining the degree “Dr. med.” (AJ). None of the data is published yet.
Funding
We thank the public research funding organization Deutsche Arthrose-Hilfe e.V. (Frankfurt am Main, Germany) for the financial support to realize this study. The funding body had no influence on the design of the study.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
Each of the authors (AJ, FS, YH, HC, AS, RF, SS) has read and concurs with the content in the final manuscript. The following authors have designed the study (SS), gathered and analysed the data (AJ, FS, YH, HC, SS), written the initial draft, and ensured the accuracy of the data and analysis (AJ, FS, YH, HC, AS, RF, SS).
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee of the Friedrich-Alexander-Universität Erlangen-Nürnberg approved the study (registration no. 1.077). All patients gave their written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Jacobsen, A., Seehaus, F., Hong, Y. et al. Model-based roentgen stereophotogrammetric analysis using elementary geometrical shape models: 10 years results of an uncemented acetabular cup component. BMC Musculoskelet Disord 19, 335 (2018). https://doi.org/10.1186/s12891-018-2259-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-018-2259-4