
Abstract
Background
Intimate partner violence (IPV) affects one in every three women globally. Previous studies have revealed that women’s experiences of different forms of IPV are significantly associated with a higher rate of unintended pregnancy, reduced uptake of contraception, and reduced ability to make decisions regarding their fertility. The aim of this study was to investigate whether previously observed relationships between IPV and unintended pregnancy in Ethiopia are mediated by contraceptive use and women’s autonomy.
Methods
This study was performed using nationally representative data from the 2016 Ethiopian Demographic and Health Survey (EDHS). A subsample of married women of reproductive age reporting a pregnancy within the 5 years preceding 2016 and who participated in the domestic violence sub-study of the survey were included in analyses. Logistic regression models, together with the product of coefficients method, were used to estimate direct and mediated effects.
Results
Twenty six percent of participants reported an unintended pregnancy in the 5 years preceding the survey. Sixty-four percent reported having ever experienced IPV (a composite measure of physical, sexual, emotional abuse, and partner controlling behaviour). After adjusting for potential confounding factors, unintended pregnancy was significantly positively associated with reporting sexual IPV, emotional IPV, IPV (a composite measure of physical, sexual, or emotional abuse), and multiple partner controlling behaviour. However, IPV (as a composite of all four forms), physical IPV, and partner control (single act) were not significantly associated with unintended pregnancy. Women’s autonomy, but not contraception use, had a significant partial mediation effect in the relationships between some forms of IPV and unintended pregnancy. Women’s autonomy mediated about 35, 35, and 43% of the total effect of emotional IPV, IPV (physical, sexual, and/or emotional), and multiple partner control on unintended pregnancy respectively.
Conclusion
Women’s autonomy appears to play a significant role in mediating the effect of IPV on unintended pregnancy in Ethiopia. Maternal health service interventions in Ethiopia could incorporate measures to improve women’s decision-making power to reduce the negative reproductive health effects of IPV.
Similar content being viewed by others


Background
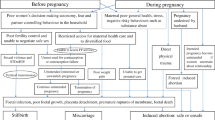
Intimate partner violence (IPV) includes acts of physical aggression, psychological abuse, sexual coercion and controlling behaviours within an intimate relationship [1]. IPV affects one in every three women globally [2]. It has several effects on women’s physical, mental, and reproductive health [3,4,5]. The reproductive health consequences of IPV include sexually transmitted infections [6,7,8], obstetric complications such as haemorrhage, abortion, hypertensive disorders, and foetal complications [3, 9], and reduced utilization of maternal health services [4, 10].
Studies have revealed that women’s experiences of different forms of IPV are significantly associated with a higher rate of unintended pregnancy [11,12,13,14,15,16,17], defined as pregnancies that are either unwanted or mistimed. Other studies have also demonstrated that IPV is associated with reduced uptake of contraception [18,19,20,21,22,23]. Women who report abuse are also more likely to have partners that make decisions for them about contraception and whether and when to have a baby [24,25,26,27]. This implies that women experiencing IPV have reduced ability to use contraception and make decisions regarding their fertility, both of which could negatively affect their ability to enact their reproductive intentions.
There is evidence that unintended pregnancy is mainly the result of inadequate contraception practice such as incorrect/non-use of contraception, discontinuation of contraceptives, and contraceptive failure [28,29,30,31]. Researchers also identified that low women’s autonomy is a significant predictor of unintended pregnancy [32,33,34]. Women’s autonomy relates to women’s power and ability to control over resources, making their own decisions, improve and maintain their health, and seek necessary information for their reproductive choices [32]. There is recognition of the importance of the interplay between IPV with contraception use, IPV with women’s autonomy, IPV with unintended pregnancy, contraception use with unintended pregnancy, and women’s autonomy with unintended pregnancy. However, there is limited evidence on the pathways by which the four experiences are inter-related i.e. how IPV affects unintended pregnancy through contraception use and women’s autonomy is less known. Furthermore, some researchers [11, 14, 35] who investigated the relationship between IPV and unintended pregnancy have treated the contraception use variable as a confounder; they explain that IPV might affect unintended pregnancy by affecting women’s contraception use. However, we argue that in the interplay between these three experiences, contraception use should be considered as a mediator rather than a confounder. In mediation, a third variable (the mediator) partly conveys the causal relationship between the exposure and outcome (Exposure → Mediator → Outcome). In contrast, with confounding a third variable (the confounder) causally affects both the exposure and the outcome. Adjustment for confounders is necessary to estimate unbiased causal effects, but confounders do not convey the causal relationship among the exposure and outcome [36].
The current study is from Ethiopia, which is generally characterized by high gender inequality, high fertility (total fertility rate of 4.6 children per woman) [37], low contraception use (only 36% of women use modern contraception) [37], high rates of unintended pregnancy (25%) [37], and one of the highest national rates of IPV (ranging from 20 to 78% in different areas of the country) [38]. In the current analysis, we hypothesized that women’s lifetime experience of IPV would be associated with contraception use and women’s autonomy in a sample of married Ethiopian women. While IPV may affect unintended pregnancy, it is likely that this effect would be mediated by contraception use and women’s autonomy that are influenced by IPV and affect unintended pregnancy.
Most available literature on IPV and its negative effects preclude defining partner controlling behaviour as a form of IPV, and consider IPV as a composite measure of physical, sexual, and emotional abuse. However, there is evidence that partner controlling behaviour is a reflection of power dynamics in an intimate relationship and indicates imminent risk of other forms of abuse [27, 39]. Studies have also revealed that partners’ control influences women’s decision-making power [27], health service access and utilization [27, 40], and fertility control [15, 41, 42]. Therefore, we have adopted the World Health Organization (WHO) definition of IPV (1 p89) and included partner control as a form of IPV in our analysis.
The hypotheses tested in this study were:
-
1)
Women who have experienced any form of IPV are more likely to have higher odds of unintended pregnancy than women who have not experienced IPV.
-
2)
Composite measures of IPV are positively associated with unintended pregnancy.
-
3)
Contraception use and women’s autonomy mediate the impact of IPV on unintended pregnancy.
-
4)
The concentration of partner controlling behaviours has a more significant effect on the mediators and the outcome than any single behaviour.
Methods
Data source, design and population
This study used data from the 2016 Ethiopian Demographic and Health Survey (EDHS), which was a cross-sectional national survey conducted from 18 January to 27 June 2016. In total, 15,683 women aged 15–49 years were sampled using random selection. For the domestic violence sub-study, only one married woman per household was selected and 5860 women were interviewed [37]. Due to the complex sampling procedures (multi stage stratified cluster sampling) used by the EDHS, sampling weights were adjusted for differences in probability of selection that allow extrapolation of results to the national level of representativeness [37].
Sample size
For this analysis, 2969 (weighted) married women who had been pregnant within 5 years preceding 2016, who had complete data related to their reproductive intentions and responded to the IPV questionnaire were included. For mothers with more than one pregnancy, we used the most recent pregnancy for the study (Fig. 1).

Schematic representation of participant selection procedure
Key: EDHS, Ethiopian Demographic and Health Survey; IPV, Intimate Partner Violence; *the final sample shown is unweighted and the weighted sample, which is reported throughout the paper, is 2,969
Measurement and variables
Dependent variable
In the woman’s questionnaire of the EDHS, the reproductive intentions of the women about each pregnancy and/or birth within the past 5 years were measured by asking participants to recall their feelings at the time of pregnancy. The optional answers were: wanted at that time of pregnancy (planned), wanted the pregnancy to happen later (mistimed), and did not want the pregnancy at all (unwanted). For the purposes of this analysis, an unintended pregnancy was defined as a pregnancy in the past 5 years that was either mistimed (i.e. the pregnancy was wanted but occurred earlier (within 2 years) than expected) or unwanted [37]. As such, the pregnancy intention of participants was categorized as unintended or intended.
Exposure variable
In the EDHS, women were asked whether or not they had experienced violent and controlling acts within their relationship, perpetrated by their husband/partner for currently married women and recent husband/partner for previously married women. Respondents were categorized as having experienced lifetime IPV if they reported experiencing at least one act of IPV [37]. Table 1 presents the questions used to assess IPV and the form of IPV the questions measuring. To further test the hypothesis that the concentrations of behaviours have a more significant effect than any single behaviour on unintended pregnancy, we recoded the partner controlling behaviour variable into none, single act, and multiple acts (where women reported two or more acts of partner controlling behaviour). We have also further investigated IPV as a composite measure of physical, sexual, and emotional abuse to allow comparison with previous research following a similar approach.
Mediator variables
Two variables − women’s autonomy and contraceptive use before the pregnancy − were considered as potential mediators. The EDHS questionnaire asked about women’s autonomy in decision-making regarding her own health care, major household purchases, and visits to her family or relatives. Women’s autonomy was coded as ‘yes’ if women reported being involved in all the three decisions, either alone or with partner or with any other person (in which she has a say in the decisions) [37]. The contraceptive use variable, which was women’s contraceptive use status before the pregnancy, was extracted from the contraceptive calendar data based on the Demographic and Health Survey (DHS) contraceptive calendar guide [43]. Then, contraceptive use variable was grouped into ‘yes’ if women used any method of contraception prior to the most recent pregnancy and ‘no’ if women didn’t use any contraception.
Covariates
Seven potentially confounding variables were identified based on prior knowledge [11,12,13, 35, 44] and context. Accordingly, current age of the respondent (15–19/20–24/25–29/30–34/35–39/40–44/45–49 years), respondent’s educational status (No formal education /primary/secondary+), religion (Christian/Muslim/other), rurality (urban/rural), region (11 administrative regions), number of children ever born (≤ 1/2 − 3/ ≥ 4), and wealth index were controlled for in the final analysis. Household wealth index was measured based on the number and kind of goods households had and housing characteristics (drinking water, toilet facility, flooring material and availability of electricity), and was generated using principal component analysis and classified into quintiles from 1 (very poor) to 5 (very rich) [37]. The DHS standard recode manual was used to define and code variables [45].
Statistical analysis
Univariate descriptive statistics were calculated for variables. Chi-square statistics were calculated to compare IPV experience and participant characteristics by pregnancy intention. Survey data analysis techniques with Stata’s ‘svy’ command were used throughout the analysis to account for complex survey data. All the analyses was conducted using Stata version 15.0 [46].
The analysis involved two steps. First, we assessed the independent association of each IPV form with unintended pregnancy using logistic regression models, adjusting for potential confounders. Then, the IPV forms showing significant association with unintended pregnancy in step one were further analysed to assess whether the hypothesized mediators mediated the observed relationships using mediation analysis with multiple mediators. Mediation analysis helps to understand the mechanisms through which exposure variables affect dependent variables [47].
To evaluate the unadjusted associations between the exposure variables (different forms of IPV), potentially mediating factors (contraceptive use and women’s autonomy), and the outcome (unintended pregnancy), we first constructed initial path models with mediating variables using the Structural Equation Modelling (SEM) builder in Stata. Then, fully adjusted multivariate mediation models were constructed using the Stata ‘gsem’ command controlling for potential confounders. Exposure variables (except partner controlling behaviour which was a categorical variable: none, single and multiple acts), mediating factors and unintended pregnancy were modelled as a binary variable. Hence, the entire path models i.e. paths linking exposure variables to mediators (path a), paths linking mediators to the outcome (path b), and paths linking exposure variables to the outcome (path c) represented a logistic model.
The mediation analysis was conducted based on the Baron and Kenny (1986) approach of testing mediation [47]. Accordingly, bivariate associations were calculated along the three paths between the three variables: Path a, Path b, and Path c. Mediation exists when the outcome variable is simultaneously regressed onto the exposure and the mediator, i.e. controlled for paths a and b, the coefficient for path c (indicated by c′) is reduced in both magnitude and significance level. If path c′ is reduced to zero, this indicates full mediation. If path c′ is not reduced to zero but still reduced in both magnitude and significance level, this suggests partial mediation [47].
In addition, we employed the product of coefficients method to statistically test if the exposure variables indirectly affected unintended pregnancy through the mediators. In the products method, path a and path b coefficients are multiplied and divided by the product of their related standard errors [48]. The Stata ‘nlcom’ command was used to statistically evaluate this; significant result of the ‘indirect effects’ indicates that mediation exists. The ‘nlcom’ command also enables to estimate the direct effect (path c′), indirect (mediated) effects (path a ∗ path b), and total effect (path c′ + (path a ∗ path b)) of IPV and partner controlling behaviours on unintended pregnancy. We executed ‘nlcom’ three times to estimate the indirect effects: once for each of the two specific indirect effects of the two mediators (contraceptive use and women’s autonomy) and once for the total indirect effect. Finally, the proportion of total effect that is mediated was calculated as \( \frac{coefficient\ of\ indirect\ effect\ }{coefficient\ of\ total\ effect}\ast 100\% \)[49].
Results
Participant characteristics
The mean age of respondents was 29 years (SD±7 years, range: 15–49 years). The majority of study participants had no formal education (62.9%), were Christian (61.0%) and living in a rural area (87.2%). In total, 36.4% of participants reported having no decision-making autonomy and 76.0% of participants reported not having used any form of contraceptive before the pregnancy. Additional characteristics of participants are shown in Table 2.
About 26% of women reported that their last pregnancy was unintended and 64% of participants reported having ever experienced IPV (a composite measure of physical, sexual, emotional abuse, and partner controlling behaviour). The least prevalent form of IPV was sexual IPV, (n = 353 (11.9%)), and the most prevalent form was partner controlling behaviour, (n = 1675 (56.4%)) (Table 2).
In univariate analysis, compared to those who reported an intended pregnancy, women who reported an unintended pregnancy reported lower rates of decision-making autonomy (p < 0.001) and contraceptive use (p = 0.029), and a higher number of children (p < 0.001) (Table 2).
The association of different forms of IPV with unintended pregnancy
In the unadjusted logistic model, a significant association was observed between unintended pregnancy and having experienced sexual IPV (Crude Odds Ratio (COR) 1.78, 95% CI: 1.26, 2.50), emotional IPV (COR 1.52, 95% CI: 1.13, 2.04), IPV (physical, sexual, and/or emotional) (COR 1.46, 95% CI: 1.13, 1.90), and having experienced multiple acts of partner control (COR 1.67, 95% CI: 1.24, 2.24). There was no significant association between unintended pregnancy and experiencing physical IPV (COR 1.23, 95% CI: 0.93, 1.64), a single act of partner control (COR 1.34, 95% CI: 0.99, 1.83), and IPV as a composite measure of all four forms (COR 1.20, 95% CI: 0.90, 1.59) (Table 3).
After adjusting for potential confounders, the significant associations of unintended pregnancy with sexual IPV (Adjusted Odds Ratio (AOR) 1.71, 95% CI: 1.18, 2.48), emotional IPV (AOR 1.40, 95% CI: 1.02, 1.93), IPV (physical, sexual, and/or emotional) (AOR 1.39, 95% CI: 1.05, 1.85), and multiple partner control (AOR 1.57, 95% CI: 1.16, 2.14) persisted (Table 3).
Mediation analysis results
In the first mediation model (Fig. 2a, Table 4), sexual IPV was significantly associated with unintended pregnancy (path c, β = 0.539, p = 0.004) but sexual IPV was not significantly associated with contraceptive use (path a1, β = 0.033, p = 0.872) nor with women’s autonomy (path a2, β = − 0.351, p = 0.053). After controlling for contraception use and women’s autonomy, the coefficient for sexual IPV was decreased in magnitude and significance (path c′, β = 0.505, p = 0.008). However, as both path a’s in this model were not significant, neither mediator met established criteria for mediation.

a-d Mediation effects for contraceptive use and women’s autonomy on the relationship between different forms of IPV and unintended pregnancy
Key: Multiple regression coefficients determined by steps 1–3 of the mediation analysis are given along the path line. ***p < 0.001, **p < 0.01, *p < 0.05. All models were adjusted for age, number of children, education, religion, household wealth index, rurality, and region
In the second mediation model (Fig. 2b, Table 4), emotional IPV was significantly associated with contraceptive use (path a1, β = − 0.404, p = 0.007), women’s decision-making autonomy (path a2, β = − 0.380, p = 0.006), and unintended pregnancy (path c, β = 0.339, p = 0.037). The association between women’s autonomy and unintended pregnancy, controlling for emotional IPV, was also significant (Path b2, β = − 0.539, p < 0.001) but the association between contraceptive use and unintended pregnancy was not significant (Path b1, β = − 0.269, p = 0.103). In addition, the path from women’s autonomy to contraception use was not significant (β = 0.057, p = 0.699). After controlling for contraception use and women’s autonomy, the association between emotional IPV and unintended pregnancy was decreased in magnitude and lost significance (path c′, β = 0.281, p = 0.094). Therefore, the effect of emotional IPV on unintended pregnancy was partially mediated by women’s autonomy but contraception use did not indicate any mediation effect in this relationship as Path b1 was not significant.
In the third mediation model (Fig. 2c, Table 4), IPV (physical, sexual, and/or emotional) was significantly negatively associated with women’s autonomy (path a2, β = − 0.307, p = 0.009) and IPV was significantly positively associated with unintended pregnancy (path c, β = 0.332, p = 0.021). The negative association between women’s autonomy and unintended pregnancy, controlling for IPV, was also significant (Path b2, β = − 0.537, p < 0.001). However, the associations between IPV with contraception use (path a1), contraception use with unintended pregnancy (path b1), and women’s autonomy with contraception use were not significant. After controlling for women’s autonomy and contraception use, the coefficient for IPV was decreased in magnitude and significance (path c′, β = 0.300, p = 0.040). Therefore, the effect of IPV on unintended pregnancy was partially mediated by women’s autonomy, but not by contraception use.
In the final mediation model (Fig. 2d, Table 4), multiple partner control was significantly associated with contraceptive use (path a1, β = − 0.391, p = 0.006) and women’s autonomy (path a2, β = − 0.661, p < 0.001). When multiple partner control was adjusted in the model, women’s autonomy (Path b2, β = − 0.519, p < 0.001), but not contraception use (Path b1, β = − 0.259, p = 0.113), was significantly associated with unintended pregnancy. After controlling for contraception use and women’s autonomy, the coefficient for multiple partner control decreased in magnitude from path c, β = 0.453 to path c′, β = 0.365 and reduced in significance from p = 0.004 to p = 0.022, indicating partial mediation of the effects of multiple partner control on unintended pregnancy by women’s decision-making autonomy. Again, despite path a1 was significant and path c′was reduced in both magnitude and significance, contraceptive use did not meet established mediation criteria because path b1 was not significant.
Overall, in the multivariate logistic mediation analysis, three partial mediation effects were identified. The first effect was the association between emotional IPV and unintended pregnancy, which was partially mediated by women’s decision-making autonomy after controlling for potential confounders. Accordingly, the direct, indirect effect through women’s autonomy, total indirect effect, and total effects of emotional IPV on unintended pregnancy were (AOR 1.32, 95% CI: 0.95, 1.84), (AOR 1.23, 95% CI: 1.04, 1.46), (AOR 1.37, 95% CI: 1.08, 1.74), and (AOR 1.81, 95% CI: 1.26, 2.60) respectively. Therefore, the total proportion mediated was 52.8% and women’s autonomy alone mediated 34.5% of the total effect of emotional IPV on unintended pregnancy. The second effect was IPV (physical, sexual, and/or emotional) and unintended pregnancy, which was again partially mediated by women’s autonomy. Accordingly, the direct effect of IPV on unintended pregnancy was AOR 1.35 (95% CI: 1.01, 1.80), indirect effect through women’s autonomy was AOR 1.18 (95% CI: 1.01, 1.37), and total indirect effect was AOR 1.18 (95% CI: 1.01, 1.39). Therefore, about 35.4% of the total effect of IPV on unintended pregnancy was mediated by women’s autonomy. The third effect was the partial mediation effect of women’s autonomy in the association between multiple partner controlling behaviour and unintended pregnancy. In this model, the mediators mediated about 55% of the total effect of multiple partner controlling behaviours on unintended pregnancy, while women’s autonomy alone mediated 42.4% of the total effect (Table 5).
Discussion
The current study investigated unintended pregnancy in relation to different forms of IPV in Ethiopia and the role contraceptive use and women’s autonomy plays in these relationships. We computed a series of multiple mediation logistic analyses to examine the interplay between the IPV types, contraceptive use, women’s autonomy, and unintended pregnancy. Women’s autonomy, but not contraceptive use, had a significant partial mediation role in the relationship of unintended pregnancy with some forms of IPV and unintended pregnancy. Given that unintended pregnancies are common in Ethiopia and women have less power in intimate relationships, this study provides insights into the need to develop and initiate culturally appropriate women’s empowerment interventions in maternal health programs to mitigate some of the negative reproductive health impacts of IPV.
Women’s experience of IPV (physical, sexual, and/or emotional) was associated with unintended pregnancy, which is in line with previous research that investigated the association between combined forms of IPV with unintended pregnancy [11,12,13, 35, 50]. Though our study was cross-sectional, which limits our ability to draw conclusions regarding causality, the effect of IPV on unintended pregnancy was both direct and indirect. The direct effect could be through coerced pregnancy (coercion by husband to become pregnant) or coerced unprotected sex (coercion by partner to have sex against her will) [41, 42]. This study further revealed that IPV might influence unintended pregnancy indirectly by reducing women’s autonomy. This could be because abusive partners might dominate women economically and emotionally that may cause women’s inability to make decisions freely [32].
In this study, contraception use did not show any mediation role in the relationship between IPV and unintended pregnancy. A similar finding from the U.S also revealed that the significant association between IPV and unintended pregnancy, where abused women were twice as likely as non-abused women to have had an unintended pregnancy, was not mediated by condom use. In this study, condom use had a positive association with unintended pregnancy and IPV had a negative association with condom use but both associations were not significant [51]. While some previous evidence has shown that IPV is associated with contraception use [18,19,20], in this study the association between IPV and contraception use was not significant. In Ethiopia, contraceptive use is generally low; for example, in this sample, only 24% of women were using contraception. Women in an abusive relationship share similar other socio-cultural and religious factors that hinders Ethiopian women from contraception access and use such as religious objection, community disapproval, rumours and perceived side effects among others [37]. As a result, there may be other immediate factors influencing women’s contraception use.
This study revealed that emotional IPV was negatively associated with women’s autonomy and women’s autonomy, in turn, was negatively associated with unintended pregnancy. However, there was no direct association between emotional IPV and unintended pregnancy after adjusting for women’s autonomy. This implies that the association between emotional IPV and unintended pregnancy was explained by the role of decision-making autonomy as mediator. Women who experienced emotional abuse could have reduced control over their reproductive choices and, potentially, reduced access to resources to achieve this. There is also evidence that emotional IPV is often accompanied by other forms of IPV [2] and the synergistic effect of these co-occurrences might lead to the strong association between emotional IPV and low women’s autonomy.
In this study, multiple partner controlling behaviour was significantly associated with unintended pregnancy, low contraceptive use, and low women’s autonomy. Simultaneously, women’s autonomy was associated with unintended pregnancy suggesting that not only partner control and unintended pregnancy were associated, but also partner control may influence unintended pregnancy by reducing women’s autonomy. Partner controlling behaviour is a reflection of power dynamics in an intimate relationship and husbands’ attempt to closely control and monitor their wives’ behaviour may affect women’s autonomy, contraceptive access and use, and fertility control [15, 27, 40,41,42]. Our finding demonstrated that the higher the number of partner controlling behaviours, the more severely a woman was being controlled; therefore, her autonomy in decision-making is lower, and her ability to control her fertility is more likely to be compromised compared with women not subjected to controlling behaviours. In Ethiopia, where patriarchal views are common, controlling behaviour is considered an acceptable behaviour for husbands in interactions with their wives [52, 53]. For this reason, women who have not experienced any partner control and those who experienced single partner control might not differ significantly in terms of the impact of partner control on their reproductive intentions.
The current study showed that physical IPV was associated with women’s autonomy, but not with contraceptive use nor unintended pregnancy. It is reasonable to think that women for fear of physical abuse might not have overall freedom and might therefore refrain from making their own decisions. The lack of a significant association between physical abuse and unintended pregnancy is supported by some previous research [35, 44] but contradicts findings from other studies [11, 50, 54]. In contrast, sexual IPV was significantly associated with unintended pregnancy but sexual IPV did not show a significant association with contraceptive use and women’s autonomy. This implies that the association between sexual IPV and unintended pregnancy was direct and could be because of forced unprotected sex despite risk of pregnancy during the ‘unsafe period of conception’ [41].
In this study, a lack of autonomy was strongly associated with high odds of unintended pregnancy in all the models. The more women have autonomy, the more likely they are to have access to and control over resources, access to health care, and the ability to decide on fertility (how many children to have and when to have the children) [32] thereby protecting them from unintended pregnancy. Contrary to the general perception, the association between contraception use and unintended pregnancy was not significant. The majority of women in the sample (76%) were not utilizing contraception and we assume that this high non-use may have affected the results. Moreover, further is required to understand what types of contraception were used, how effective these contraceptives were, and how consistently women have been using contraception. Lastly, while we hypothesized that there might be a relationship between the two mediators, that is, when women are autonomous, they are more likely to use contraception, our study did not show any significant association between these two variables. In this study, we have measured women’s overall autonomy in household matters and this might not necessarily reflect their autonomy in contraceptive choices.
As there is no prior study that has examined the role of IPV on unintended pregnancy and how women’s autonomy and contraception use plays a role in this relationship, the findings could contribute to design interventions for women in abusive relationships in Ethiopia that help mitigate the detrimental reproductive health effects of IPV. However, the findings should be considered in light of some limitations. Data for the current analysis were drawn solely from a cross-sectional study so causal inferences could not be made. Women with unintended pregnancies or low autonomy in decision-making may enter into violent relationships. Therefore, future prospective studies are needed to examine the temporal order of the IPV-unintended pregnancy association and potential mediators in this relationship. The partial mediation maintains that women’s autonomy accounts for some, but not all, of the relationship between some forms of IPV and unintended pregnancy. This implies that the assumed pathways are not entirely established. Another limitation is that although potential confounding variables were included, there could still be some residual confounding effects. Reports of IPV may also be underestimated due to social desirability bias. However, the study has strictly followed WHO strategies for domestic violence research which should minimize such under-reporting [55].
Conclusions
This study has indicated that sexual IPV, emotional IPV, IPV (physical, sexual, and/or emotional), and multiple controlling behaviours were associated with unintended pregnancy. The associations of emotional IPV, IPV (physical, sexual, and/or emotional), and multiple controlling behaviours with unintended pregnancy were partially mediated by women’s autonomy where women’s autonomy mediated about 35, 35, and 43% of the total effect of these relationships, respectively. However, there was no mediation effect of contraception use in the relationships between these forms of IPV and unintended pregnancy. Reproductive health programs and strategies designed to improve fertility choices among women in Ethiopia should address both intra- and interpersonal factors in order to create conditions under which women are empowered to involve in making decisions about their own fertility. Interventions with women’s partners that reduce the incidence of IPV are also necessary. In the meantime, focussed interventions on improving victimized women’s decision-making power may help mitigate the effect of IPV on unintended pregnancy and other reproductive health problems.
Availability of data and materials
The datasets supporting the conclusions of this article are freely available to the public at www.measuredhs.com and can be accessed after request is made to and approved by the DHS program.
Abbreviations
- AOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- COR:
-
Crude odds ratio
- DHS:
-
Demographic and health survey
- EDHS:
-
Ethiopian demographic and health survey
- IPV:
-
Intimate partner violence
- WHO:
-
World Health Organization
References
Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R. world report on violence and health. Geneva: World Health Organization; 2002.
World Health Organization (WHO). Global and Regional Estimates of Violence against Women: Prevalence and Health Effects of Intimate Partner Violence and Nonpartner Sexual Violence. Geneva: World Health Organization; 2013.
Black MC. Intimate partner violence and adverse health consequences. Am J Lifestyle Med. 2011;5(5):428–39.
Sunita K, Kiersten J. Profiling Domestic Violence: A Multi-Country Study. Calverton: ORC Macro; 2004.
Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359(9314):1331–6.
Laanpere M, Ringmets I, Part K, Karro H. Intimate partner violence and sexual health outcomes: a population-based study among 16-44-year-old women in Estonia. Eur J Pub Health. 2013;23(4):688–93.
Lary H, Maman S, Katebalila M, McCauley A, JM. Exploring the association between HIV and violence: young people’s experiences with infidelity, violence and forced sex in Dar es Salaam, Tanzania. Int Fam Plann Perspect. 2004;30:200–6.
Sori AT. Poverty, sexual experience and HIV vulnerability risks: evidence from Addis Ababa, Ethiopia. J Biosoc Sci. 2012;44(6):677–701.
Devries KM, Kishor S, Johnson H, Stöckl H, Bacchus LJ, Garcia-Moreno C, et al. Intimate partner violence during pregnancy: analysis of prevalence data from 19 countries. Reprod Health Matters. 2010;18(36):158–70.
Mohammed BH, Johnston JM, Harwell JI, Yi H, Tsang KW, Haidar JA. Intimate partner violence and utilization of maternal health care services in Addis Ababa, Ethiopia. BMC Health Serv Res me. 2017;17(1):178.
Rahman M, Sasagawa T, Fujii R, Tomizawa H, Makinoda S. Intimate partner violence and unintended pregnancy among Bangladeshi women. J Interpers Violence. 2012;27(15):2999–3015.
Pallitto CC, O'Campo P. The relationship between intimate partner violence and unintended pregnancy: analysis of a national sample from Colombia. Int Fam Plann Perspect. 2004;30(4):165–73.
Pallitto CC, Garcia-Moreno C, Jansen HA, Heise L, Ellsberg M, Watts C, et al. Intimate partner violence, abortion, and unintended pregnancy: results from the WHO multi-country study on Women's health and domestic violence. Int J Gynaecol Obstet. 2013;120(1):3–9.
Begum S, Dwivedi SN, Pandey A, Mittal S. Association between domestic violence and unintended pregnancies in India: findings from the National Family Health Survey-2 data. Natl Med J India. 2010;23(4):198–200.
Tiwari S, Gray R, Jenkinson C, Carson C. Association between spousal emotional abuse and reproductive outcomes of women in India: findings from cross-sectional analysis of the 2005-2006 National Family Health Survey. Soc Psychiatry Psychiatr Epidemiol. 2018;53(5):509–19.
Kamal SM. Domestic violence, unwanted pregnancy and pregnancy termination among urban women of Bangladesh. J Family Reprod Health. 2013;7(1):11–22.
Abeya S, Afework MF, Yalew AW. Health Effects of Intimate Partner Violence against Women: Evidence from Community Based Cross Sectional Study in Western Ethiopia. Sci Technol Arts Res J. 2013;2:48.
Maxwell L, Devries K, Zionts D, Alhusen JL, Campbell J. Estimating the effect of intimate partner violence on Women’s use of contraception: a systematic review and meta-analysis. PLoS One. 2015;10(2):e0118234.
Stephenson R, Jadhav A, Hindin M. Physical domestic violence and subsequent contraceptive adoption among women in rural India. J Interpers Violence. 2012;28(5):1020–39.
Williams CM, Larsen U, McCloskey LA. Intimate partner violence and Women's contraceptive use. Violence Against Women. 2008;14(12):1382–96.
Gee RE, Mitra N, Wan F, Chavkin DE, Long JA. Power over parity: intimate partner violence and issues of fertility control. Am J Obstet Gynecol. 2009;201(2):148.e1–7.
Bishwajit G, Yaya S. Domestic violence: a hidden barrier to contraceptive use among women in Nigeria. Open Access J Contracept. 2018;9:21–8.
Elouard Y, Weiss C, Martin-Hilber A, Merten S. Sexual violence as a risk factor for family planning-related outcomes among young Burundian women. Int J Public Health. 2018;63(1):13–22.
Bauleni EM, Hooker L, Vally HP, Taft A. Intimate-partner violence and reproductive decision-making by women attending Victorian maternal- and child-health services: a cross-sectional study. Aust J Prim Health. 2018;24(5):422–7.
Pearson E, Andersen KL, Biswas K, Chowdhury R, Sherman SG, Decker MR. Intimate partner violence and constraints to reproductive autonomy and reproductive health among women seeking abortion services in Bangladesh. Int J Gynaecol Obstet me. 2017;136(3):290–7.
Grace KT, Anderson JC. Reproductive coercion: a systematic review. Trauma Violence Abuse. 2018;19(4):371–90.
Krantz G, Nguyen DV. The role of controlling behaviour in intimate partner violence and its health effects: a population based study from rural Vietnam. BMC Public Health. 2009;9:143.
Tsui AO, McDonald-Mosley R, Burke AE. Family planning and the burden of unintended pregnancies. Epidemiol Rev. 2010;32(1):152–74.
Bishwajit G, Tang S, Yaya S, Feng Z. Unmet need for contraception and its association with unintended pregnancy in Bangladesh. BMC Pregnancy Childbirth. 2017;17(1):186.
Bradley SE, Croft T, Rutstein SO. The impact of contraceptive failure on unintended births and induced abortions: estimates and strategies for reduction. DHS analytical studies. Calverton: ICF Macro; 2011.
Jain AK, Winfrey W. Contribution of contraceptive discontinuation to unintended births in 36 developing countries. Stud Fam Plan. 2017;48(3):269–78.
Rahman M. Women’s autonomy and unintended pregnancy among currently pregnant women in Bangladesh. Matern Child Health J. 2012;16(6):1206–14.
Brown SS, Eisenberg L, editors. The best intentions: unintended pregnancy and the well-being of children and families. Washington, D.C: National Academies Press; 1995.
Adhikari R, Soonthorndhada K, Prasartkul P. Correlates of unintended pregnancy among currently pregnant married women in Nepal. BMC Int Health Hum Rights. 2009;9(1):17.
Stockl H, Hertlein L, Himsl I, Delius M, Hasbargen U, Friese K, et al. Intimate partner violence and its association with pregnancy loss and pregnancy planning. Acta Obstet Gynecol Scand. 2012;91(1):128–33.
MacKinnon DP, Krull JL, Lockwood CM. Equivalence of the mediation, confounding and suppression effect. Prev Sci. 2000;1(4):173–81.
Central Statistical Agency (CSA) [Ethiopia], ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, and Rockville: CSA and ICF; 2017.
Semahegn A, Mengistie B. Domestic violence against women and associated factors in Ethiopia; systematic review. Reprod Health. 2015;12(1):78.
Gage AJ, Hutchinson PL. Power, control, and intimate partner sexual violence in Haiti. Arch Sex Behav. 2006;35(1):11–24.
Gautam S, Jeong H-S. The role of women’s autonomy and experience of intimate partner violence as a predictor of maternal healthcare service utilization in Nepal. Int J Environ Res Public Health. 2019;16(5):895.
Miller E, McCauley HL, Tancredi DJ, Decker MR, Anderson H, Silverman JG. Recent reproductive coercion and unintended pregnancy among female family planning clients. Contraception. 2014;89(2):122–8.
Samankasikorn W, Alhusen J, Yan G, Schminkey DL, Bullock L. Relationships of reproductive coercion and intimate partner violence to unintended pregnancy. J Obstet Gynecol Neonatal Nurs. 2019;48(1):50–8.
MEASURE DHS/ICF International. DHS Contraceptive Calendar Tutoria. Rockville: The Demographic and Health Surveys Program; 2018.
Taft AJ, Powell RL, Watson LF. The impact of violence against women on reproductive health and child mortality in Timor-Leste. Aust N Z J Public Health. 2015;39(2):177–81.
MEASURE DHS/ICF International. Demographic and Health Surveys Standard Recode Manual for DHS 7. Rockville: The Demographic and Health Surveys Program; 2018.
StataCorp. Stata statistical software: Release 15. College Station, TX: StataCorp LLC; 2017.
Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173.
MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83–104.
Bruin J. Command to compute new test UCLA; 2006. Available from: https://stats.idre.ucla.edu/stata/faq/how-can-i-do-mediation-analysis-with-a-categorical-iv-in-stata/.
Silverman JG, Gupta J, Decker MR, Kapur N, Raj A. Intimate partner violence and unwanted pregnancy, miscarriage, induced abortion, and stillbirth among a national sample of Bangladeshi women. Bjog. 2007;114(10):1246–52.
Cha S, Masho SW, Heh V. Partner violence victimization and unintended pregnancy in Latina and Asian American women: analysis using structural equation modeling. Women Health. 2017;57(4):430–45.
Abeya SG, Afework MF, Yalew AW. Intimate partner violence against women in West Ethiopia: a qualitative study on attitudes, woman's response, and suggested measures as perceived by community members. Reprod Health. 2012;9:14.
Garcia-Moreno C, Jansen HAFM, Ellsberg M, Heise L, Watts CH. Prevalence of intimate partner violence: findings from the WHO multi-country study on women's health and domestic violence. Lancet. 2006;368(9543):1260–9.
Zakar R, Nasrullah M, Zakar MZ, Ali H. The association of intimate partner violence with unintended pregnancy and pregnancy loss in Pakistan. Int J Gynaecol Obstet. 2016;133(1):26–31.
World Health Organization (WHO). Putting women first: ethical and safety recommendations for research on domestic violence against women. Geneva: World Health Organization; 2001.
Acknowledgements
We are grateful to the Central Statistical Agency of Ethiopia and Measure DHS program, which allowed us to access and use the data freely. We are also thankful to the women who participated in the survey and shared their IPV experiences. We thank the University of Newcastle, the Hunter Medical Research Institute, and the Research Centre for Generational Health and Ageing for creating a quality research environment for us to accomplish this work.
Funding
This study is partially funded by the University of Newcastle, Australia which has provided a full scholarship for the student researcher (primary author) and supported him in obtaining statistical support and training. The second author (MLH) is funded by an Australian Research Council Discovery Early Career Research Award. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
TYT is involved from the conception of the study to the write up of the manuscript. MLH, CC, EH and DL made substantial contributions in supervising the overall research activities (conception, proposal development, data preparation and analysis, and write up of the manuscript). All authors involved in revising the manuscript. The author(s) read and approved the final manuscript.
Authors’ information
Tenaw Yimer Tiruye is a Ph.D. student at the University of Newcastle, Australia. His research focuses on the determinants, consequences and responses to intimate partner violence. He is interested in evaluating multidimensional effects of intimate partner violence on maternal and child health and generating evidence for decision-making. Dr. Melissa L. Harris is a postdoctoral research fellow at the University of Newcastle. Dr. Harris has an interest in chronic diseases management, including the impacts of psychological factors on physical health and healthcare outcomes and contraceptive practices of women. Dr. Catherine Chojenta is a postdoctoral research fellow at the University of Newcastle. She is a public health researcher with a particular focus on women’s health and wellbeing across the life course. Dr. Elizabeth Holliday is an Associate Professor and senior biostatistician in the School of Medicine and Public Health at the University of Newcastle. Her particular focus is promoting statistical excellence in medical research. Prof Deb Loxton is a professor of public health at the University of Newcastle. She is a co-director of research center for generational health and aging and co-director of Australian longitudinal study on women’s health. She has interest on examining the health and wellbeing of women who have lived with violent partners, and the impact of reproductive health options and choices on women.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The original survey was conducted after being ethically approved by the National Research Ethics Review Committee (NRERC) (Ref. No: 3.10/114/2016). The interview continued only if participants consent to participate and privacy was certain. Prior to analysis, we have obtained permission from the DHS program and ethical approval from University of Newcastle Human Research Ethics Committee (Ref. No: H-2018-0055).
Consent for publication
‘Not applicable’.
Competing interests
The authors have declared that no competing interests exist. All authors agreed on the submission of the manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tiruye, T.Y., Harris, M.L., Chojenta, C. et al. The mediation effect of contraceptive use and women’s autonomy on the relationship between intimate partner violence and unintended pregnancy in Ethiopia. BMC Public Health 20, 1408 (2020). https://doi.org/10.1186/s12889-020-09514-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-020-09514-7