
Abstract
Background
In Perú, HIV disproportionately affects men who have sex with men (MSM). Despite widespread access to treatment, the high rate of new HIV infections has remained unchanged over the last decade. Low knowledge of HIV status associated with late diagnosis is a key factor underlying the high HIV incidence observed in this setting, creating conditions for efficient onward transmission. Improving access to HIV testing and prevention services for those at highest risk is an important public health priority. Sex-on-premise venues (SOPVs) – saunas, sex clubs, pornographic movie theaters, hourly hotels, and bars/discos with areas where sex is permitted – may be opportune sites for outreach; however, further research on SOPVs and the populations who frequent them is needed to inform such efforts.
Methods
We conducted a cross-sectional online survey of adult MSM in Lima, Perú to evaluate patterns of SOPV attendance, associated sexual risk behaviors, and attitudes toward SOPV-based interventions. Participants were recruited through outreach to social media networks affiliated with local LGBTQ-aligned community groups. Our primary analytic objective was to estimate the association of HIV-related sexual risk behaviors and SOPV attendance. Additionally, we performed exploratory analyses to describe risk behavior stratified by SOPV category and to examine the relationship between SOPV attendance and the use of online platforms to meet sex partners.
Results
Overall, 389 MSM completed the survey from November 2018 through May 2019, of whom 68% reported attending an SOPV in the last 3 months. SOPV attendance was associated with multiple sexual risk behaviors, including transactional sex, group sex, substance use around the time of sex, and higher number of partners. Over two thirds of SOPV attendees indicated they would accept HIV testing if offered at SOPVs.
Conclusions
SOPV attendance was common among MSM in Lima who participated in our survey, and SOPV attendees reported significantly greater engagement in sexual risk behaviors related to HIV transmission. Attitudes toward hypothetical SOPV-based interventions were generally favorable. These findings suggest that outreach at SOPVs may be an effective mechanism for reaching a particularly high-risk sub-population of MSM in Perú to deliver targeted HIV testing and prevention interventions.
Similar content being viewed by others


Background
As in most of the Americas, the HIV epidemic in Perú is concentrated among men who have sex with men (MSM) and transgender women (TW). Prevalence among these groups countrywide in 2018 was reported to be 12 and 16%, respectively [1], although in the capital city of Lima it may be substantially higher, with estimates ranging from 18-20% among MSM and 17-30% among TW [2,3,4,5,6]. In addition, high HIV incidence persists, with some studies reporting rates of >10 per 100 person-years [3, 4, 7]. Most notable, however, is the fact that HIV incidence in Perú has not significantly changed over the last decade – despite the broad scale-up of antiretroviral treatment (ART) access during this time. While UNAIDS estimates suggest a stable overall incidence rate of 1.1 (confidence interval [CI] 0.7 – 1.8) per 100 person-years in 2010 compared to 0.9 (CI 0.5 – 1.6) in 2017 [1], data from the Peruvian Ministry of Health show a 27% increase (from 4677 to 5926 cases) in new HIV diagnoses over this same time period [8]. Since 2004 the Ministry of Health has provided antiretroviral treatment (ART) at no cost to individuals with HIV infection who meet clinical and immunologic criteria [9], and has moved to extend ART coverage to all Peruvians living with HIV following the release of the World Health Organization (WHO) “treat all” recommendations in 2015 [10,11,12]. In contrast to the expansion in access to ART for HIV treatment, the use of antiretroviral drugs for pre-exposure prophylaxis (PrEP) is not yet subsidized in Perú and access remains quite limited, with fewer than 1500 active PrEP users estimated in the country currently [13].
Delayed diagnosis of HIV infection is an important factor fueling onward sexual transmission in Perú [14,15,16,17]. One recent study estimated that just 24% of MSM and TW living with HIV in Perú have been diagnosed, and among these only half are linked to care and on ART [18] – falling far short of the UNAIDS “90-90-90” targets [19]. To close these gaps in Perú’s HIV services continuum, new approaches are needed that more effectively engage vulnerable MSM and TW. Strategies that aim to address the underlying psychological and structural barriers experienced by members of these communities – including stigma, fear, low risk perception, and geographic factors [20,21,22,23] – are most likely to have success.
Previous research suggests that offering HIV testing at community-based venues can reach individuals who may not otherwise access traditional clinic-based services [24,25,26,27,28], including in Perú [5, 7, 29]. Sex-on-premise venues (SOPVs), which are social venues that provide a space to meet and have sex with other patrons, may be fitting sites for such outreach. Although sex is the primary, and often overtly stated, purpose of many SOPVs (e.g. sex clubs, pornographic movie theaters, and most saunas/bathhouses), the term also encompasses commercial establishments where sex is permitted or encouraged, even if not explicitly endorsed as its reason for being (e.g. hourly hotels and bars/discos with dark rooms) [30, 31]. Studies from high-income countries (HIC) with concentrated HIV epidemics affecting MSM, including Australia and the United States, have found an association between SOPV attendance and high-risk sexual behavior [32,33,34,35,36]. In addition, the feasibility of delivering sexual health interventions at SOPVs has been well documented in HIC settings, including programs offering safer sex counseling, free condom distribution, on-site testing for HIV and other sexually transmitted infections (STI), and distribution of HIV self-testing kits [37,38,39,40,41,42,43,44,45,46,47]. While intervention uptake among SOPV patrons was relatively modest in two studies that assessed this outcome (uptake was 24% [37] and 51% [39], respectively), several studies demonstrated SOPV-based HIV/STI testing to be effective at reaching individuals at high risk, including those who may not otherwise come to be tested in healthcare facilities. In contrast to the evidence base from HICs, research related to SOPVs and the populations who attend them in low- and middle-income countries (LMIC) such as Perú remains extremely limited.
Despite the paucity of evidence on the role of SOPVs in Perú’s HIV epidemic – and in the Latin American context more broadly – several factors suggest that SOPVs may be ideal sites at which to conduct outreach to Peruvian MSM and TW at highest risk for HIV infection. MSM and TW in Perú commonly live at home with their family of origin [48, 49], where conservative social norms [50] and stigma related to gender and sexuality [51,52,53] can create powerful disincentives to bringing sex partners home. By functioning as alternative locations where MSM and TW can go to meet sex partners, SOPVs may play a fundamentally different – and relatively more important – role in Perú as compared to regions with more progressive social norms, including the HIC settings where much of the existing literature on SOPVs is based. Additionally, the use of online platforms to facilitate efficient identification of sex partners – including geosocial networking apps – is increasing in Perú [49]. SOPVs may be important meeting places for sex after meeting a prospective partner online. Importantly, SOPVs are by definition physical locations where individuals gather. Thus, in contrast to internet-based outreach, SOPVs are sites where HIV testing and biomedical prevention interventions could be delivered directly. Several recent studies among MSM and TW in Lima demonstrated high uptake of HIV testing, as well as high rates of new HIV diagnoses, at bars and other public social venues – including some SOPVs [5, 7, 29]. However, we were unable to identify any dedicated research from Perú – or any other Latin American country – focusing specifically on SOPVs or their clientele. One possible explanation is that SOPVs are only now being appreciated, and their importance emphasized, in the context of the surging popularity of online platforms to meet sex partners. In order to better understand the role of SOPVs within high-risk sexual networks in Perú, and to inform future SOPV-based outreach strategies to deliver HIV testing and prevention interventions, we conducted an online survey of MSM and TW in Lima. The goals of this study were to evaluate the prevalence and patterns of SOPV attendance, the association of SOPV attendance with sexual risk behaviors, and the attitudes toward potential SOPV-based interventions in these communities.
Methods
Study population and design
We conducted a cross-sectional, internet-based survey among MSM and TW in Lima, Perú. Adults 18 years of age or greater who identified as either MSM or TW were eligible. We recruited participants by disseminating a link to the survey via social media platforms affiliated with a local LGBTQ-aligned community-based organization in Lima. An initial landing page included the consent form, basic instructions, and eligibility criteria. This was formatted for both desktop and mobile access, enabling survey participation from any computer or mobile device with an internet connection. Prior to accessing the survey, individuals were required to provide an electronic signature as an attestation of their eligibility and informed consent. Participation was completely anonymous and no incentive was offered. The study underwent bioethics review and received approvals from both the Vía Libre Comité Institucional de Bioética (Lima, Perú) and the University of Washington Institutional Review Board (Seattle, USA).
Survey instrument
REDCap [54] was used for survey instrument development and administration, as well as data collection and storage. The survey included a total of 19 main questions, some of which branched to sub-questions based on the response (Additional file 1). Depending on the number of sub-questions prompted (based on answers to the main questions), survey completion took approximately 10-15 min. We collected basic demographic data and asked participants about venue attendance and sexual behaviors in the past 3 months, including how/where they met their recent partners and where they went to have sex, as well as online platforms used to meet partners. In addition to questions about SOPV attendance and sexual behaviors in general, we collected more detailed venue-specific data for participants who reported sex at an SOPV with either their last or penultimate partner (in the last 3 months). This included information about the physical and environmental features of the venue(s) they attended, sexual behaviors there (both observed and participated, including condom use), and attitudes toward hypothetical venue-based sexual health interventions such as condom/lubricant distribution and point-of-care testing for HIV and other sexually transmitted infections (STIs).
Statistical analysis
After reaching our target of 400 completed surveys, data were exported from REDCap into Stata version 15 (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC) for analysis. We used descriptive statistics to summarize the proportion of participants who reported attending an SOPV in the last 3 months, as well as participant characteristics, including demographics, sexual behaviors (including the overall proportion who used an online platform to meet a sex partner in the last 3 months), knowledge of biomedical HIV prevention (e.g. PrEP, “U=U”), attitudes toward venue-based HIV testing and prevention interventions, and other venue-specific factors. The objective of our primary analysis was to evaluate the relationship between sexual risk behaviors and SOPV attendance in the previous 3 months. We defined an SOPV as any of the following 5 venue categories: sauna, hotel, sex club, pornographic movie theater, or bar/disco known to permit sex. Additionally, we defined two categories of SOPV attendance: meeting a partner at, and having sex at, an SOPV. We estimated the crude prevalence ratio (PR) and 95% confidence interval (CI) for each factor of interest (all of which were coded as dichotomous variables), comparing the proportion with a given factor among participants who reported meeting a partner at (or having sex at) an SOPV in the previous 3 months to the proportion among those who did not. To further examine patterns of SOPV attendance and use of online platforms to identify sex partners, we conducted several exploratory sub-analyses, stratifying by SOPV category, using the detailed venue-level data collected on the last two partners. All statistical testing to estimate confidence intervals and prevalence ratios used the Chi-squared distribution. Statistical testing to assess for differences in proportions used either the Chi-squared or Fisher’s exact test.
Results
From November 26, 2018 through May 16, 2019 a total of 389 MSM and 8 TW completed the online survey. Two transgender male and two cisgender female identifying individuals also completed a survey but were excluded from the analysis as they did not meet predetermined inclusion criteria. Additionally, because the low number of TW participants was insufficient to draw meaningful inferences for this important but distinct sub-population [55], we restricted our analysis to cisgender MSM only.
Demographic and behavioral characteristics
Among 389 MSM, 77% identified as homosexual, 19% as bisexual, and 3% as heterosexual (Table 1). Median age was 30 years (interquartile range [IQR] 25 – 37), and just under half (47%) had a university degree or higher (likely a reflection of the social media sites used for recruitment). Over three quarters lived with at least one family member, and more than half lived with one or both parents. Participants reported a median of 3 total sex partners (IQR 2 – 5) in the last 3 months. Nearly half reported sex under the influence of either drugs or alcohol, about one third participated in group sex, and about a quarter reported transactional sex (either received payment or paid for sex); however, only 2% identified as a sex worker. Overall, 85% reported ever being tested for HIV and 26% reported being HIV positive, the vast majority (94%) of whom indicated they were taking ART. When given a statement illustrating the concept of “U=U” (i.e. that sexual transmission of HIV is virtually impossible from an HIV-infected person with an undetectable viral load on ART), roughly half (53%) indicated this was true. A somewhat larger proportion (73%) reported that they had ever heard of PrEP.
Prevalence of SOPV attendance and online platform use to meet sex partners
Recent SOPV attendance was common, as was the use of online platforms to meet a sex partner (Table 2). Overall, 68% reported either meeting a partner or having sex at an SOPV at least once in the last 3 months (42% met a partner at an SOPV and 61% had sex at an SOPV). The most common SOPV category for meeting a new partner was bars/discos, while the most common SOPV category for having sex was hotels. The use of online platforms to meet sex partners was also common: overall, 78% reported meeting a partner online in the last 3 months (median 3 online partners, IQR 1 – 5). Grindr was by far the most frequently reported online platform, followed by Facebook and WhatsApp.
Association of SOPV attendance and sexual risk characteristics
SOPV attendees, as compared to MSM who did not attend an SOPV in the last 3 months, were more likely to report several sexual risk behaviors, including group sex, transactional sex, sex under the influence of alcohol, sex with a “casual” partner, and ≥ 3 sex partners in the last 3 months; these associations were statistically significant in all cases regardless of whether evaluated with respect to meeting a partner or to having sex at an SOPV (Table 3). SOPV attendees were somewhat more likely to report having ever been tested for HIV. However, self-reported HIV seropositivity was not associated with SOPV attendance. Meeting a partner at an SOPV, but not having sex at an SOPV, was associated with older age and higher monthly income. Having sex at an SOPV, but not meeting a partner at an SOPV, was associated with living with family and with having a recent online partner. We performed sensitivity analyses excluding self-reported HIV-positive individuals, which did not substantively alter our findings regarding the relationship between SOPV attendance and sexual risk behaviors.
Sexual Risk Behaviors and Online Platform Use Stratified by SOPV Category
Stratification by SOPV category revealed heterogeneity in the sexual risk behaviors reported by populations of MSM as defined by attendance of different categories of venue to either meet a partner or have sex (Table 4). For this exploratory sub-analysis, we define SOPV attendance as either meeting a partner or having sex at a given type of SOPV and we report only descriptive statistics, as participants could indicate they attended multiple venues, precluding the use of inferential statistical tests.
Among participants who met their last or penultimate partner online, we tabulated the SOPV categories they attended to have sex with that same partner. Of 241 participants who met their last partner online, 66 (27%) had sex at a hotel, 4 (2%) at a sauna, and 2 (< 1%) at a bar or disco; none had sex at a porno theater or sex club. Of 173 participants who met their penultimate partner online, 54 (31%) had sex at a hotel, 2 (1%) at a sauna, 1 (< 1%) at a sex club, and 1 (< 1%) at a bar/disco; none had sex at a porno theater. Overall, compared to those who did not meet a partner online, participants who met any recent partner online were more likely to report sex at a hotel (54% among those with a recent online partner vs 34% among those with no recent online partner, p = 0.001) or at a bar/disco (11% vs 2%, p = 0.016) in the last 3 months, but not at a sauna (22% vs 21%, p = 0.916), sex club (8% vs 6%, p = 0.532), or porno theater (4% vs 5%, p = 0.749).
Sexual risk at SOPVs and attitudes toward SOPV-based interventions
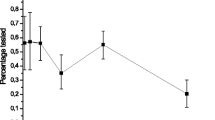
For MSM who had sex at an SOPV with at least one of their last two partners (N = 177), we tabulated venue-specific data on sexual encounters with their last (n = 138) and/or penultimate (n = 113) partners. Participants indicated that condoms were available when they had a sexual encounter at an SOPV 49% of the time overall, including 48% of the time at hotels, 57% at saunas, 76% at sex clubs, 25% at porno theaters, and 0% at bars/discos. Lube was available at the SOPV for 27% of the encounters (29% at hotels, 29% at saunas, 13% at sex clubs, 0% at porno theaters, and 50% at bars/discos). Alcohol was present at the SOPV 29% of the time for SOPVs overall (24% at hotels, 43% at saunas, 75% at sex clubs, 0% at porno theaters, and 50% at bars/discos) and group sex occurred at 20% of encounters (12% at hotels, 33% at saunas, 75% at sex clubs, 50% at porno theaters, and 50% at bars/discos). Attitudes toward hypothetical SOPV-based sexual health interventions, such as HIV/STI testing and condom/lube distribution, varied based on the category of SOPV in question, but generally indicated a high level of acceptability (Fig. 1).

Attitudes Toward Hypothetical SOPV-Based HIV/STI Testing and Sexual Health Interventions. Venue-level data are based on an aggregate total of n = 251 responses corresponding to the SOPVs where a total of N = 177 MSM reported having a sexual encounter with their last (n = 138) and/or penultimate (n = 113) partner in the last 3 months. SOPV sex-on-premise venue; STI sexually transmitted infection. *Excludes participants who self-report being HIV positive
Discussion
More than two thirds of our study population attended an SOPV either to meet a sex partner or to have sex in the last 3 months, suggesting that SOPV attendance may be quite common among MSM in Lima. In addition, those who attended an SOPV were significantly more likely to report behaviors associated with elevated risk of HIV and STI transmission, including group sex, transactional sex, sex under the influence of alcohol, sex with a casual partner, and more overall partners. Notably, the majority of SOPV attendees indicated favorable attitudes toward theoretical SOPV-based sexual health interventions such as condom/lubricant distribution and HIV/STI testing.
Although SOPV attendance was associated with several sexual risk behaviors, one notable exception was condomless anal sex. One possible explanation is that we asked questions about sexual positioning and condom use with reference to only the last two partners, rather than asking about all recent partners (as was asked for other behaviors). However, similar results to ours were observed in a large online survey conducted in the mid-2000s of MSM in the US, which found that meeting a partner at a physical venue (e.g. bars/clubs, bathhouses, and public outdoor spaces) was associated with risk behaviors such as alcohol use – but not with condomless anal sex [33]. In our exploratory analyses, sexual risk behavior also appeared to vary by SOPV category. For example, compared with other categories, the proportion of MSM reporting nearly every risk characteristic (except condomless anal sex) was higher for sex clubs (Table 4). In contrast, hourly hotels, which were by far the most common SOPV attended, appeared to be frequented by lower risk clientele. Taken together, these results suggest that more nuanced data collection may be necessary to characterize sexual risk behaviors associated with SOPV attendance in this setting. Such information, including the identification of specific SOPVs attended by the highest risk clientele, would be particularly germane to the development of SOPV-based outreach strategies to deliver HIV testing and other sexual health interventions.
The vast majority (78%) of our sample population reported meeting a sex partner online in the last 3 months. This is consistent with observations from a large contemporaneous online survey of MSM in Brazil, Mexico, and Perú conducted in 2018 by Torres et al., which found that 81% of Peruvian MSM reported using apps for sexual encounters [57]. Notably, these estimates are roughly double what was found in two studies of MSM in Lima from just a few years ago, including one conducted in 2013-2014 (in person) and another in 2012-2013 (online), which reported 37 and 44% of participants had a recent online partner, respectively [3, 49]. Together these findings likely reflect the rapid expansion in recent years of access to low-cost internet services and mobile devices in Perú; however, the use of an online survey, which selects for individuals with internet access, may have also played a small role in the higher estimates observed in both our study and by Torres et al. [57]. In addition, geosocial networking applications (e.g. Grindr), which have been associated with increased sexual risk behavior and STI incidence in some settings [58,59,60], have had substantial growth in popularity since the two earlier studies.
Our results also shed light on the relationship between online platform use and SOPV attendance. MSM who had sex at an SOPV, but not those who met a partner at an SOPV, were significantly more likely to report meeting a recent partner online. This mirrored what we observed for one’s living situation: living with family was associated having sex at an SOPV but not meeting a partner at one. One potential explanation for this pattern is that, although online platforms can facilitate the identification of sex partners, stigma precludes those who live with family from having sex with these partners at home. SOPVs might fill this void by offering places outside of the home where MSM can have sex with online partners. We also found that, when stratified by SOPV category, the association between SOPV attendance and online platform use was significant only for hotels and bars/discos, suggesting that these venues may be preferred rendezvous sites for meeting online partners for sex, perhaps because identifying new sex partners in person may be easier at saunas, sex clubs, and porno theaters.
The primary limitation of this study relates to its generalizability. Our sampling method, which relied on recruitment through local social media networks, selected a population that is somewhat more educated and affluent than the general population of MSM in Lima. Therefore, our estimates of SOPV attendance and sexual behavior may not reflect the experiences of MSM in lower socioeconomic strata. Self-reported HIV prevalence was 26%, which is within the range reported by other studies of MSM in Lima [5, 6]. However, over 80% of MSM in this study reported having ever received an HIV test and over 90% of those who self-reported being HIV positive indicated they were taking ART. In both cases, these rates are somewhat higher than past population estimates of HIV testing and ART coverage, respectively, in the region [1, 18], suggesting above average access to health services. If so, the estimates derived from our sample population may in fact under-represent the risk profile of MSM in Lima on average. Future studies of SOPV attendance and associated sexual risk behaviors in Lima should consider utilizing alternative sampling strategies to include MSM in less affluent communities, as well as TW – an extremely vulnerable population that our online recruitment strategy did not adequately reach.
Although, overall, participants reported favorable attitudes toward SOPV-based HIV/STI testing interventions (Fig. 1), interpretation of these data is limited by the small sample size for sex clubs, porno theaters, and bars/discos. The use of a survey to evaluate acceptability of hypothetical interventions may also overestimate uptake in real-world settings. Nevertheless, our results, which indicate that over two thirds of MSM would either “definitely” (45%) or “probably” (23%) accept SOPV-based HIV testing, are consistent with direct observations from the field, including a recent study that demonstrated 52% uptake of venue-based HIV testing when it was offered to MSM and TW at bars, clubs, and public parks in Lima [5].
Despite the limitations to its generalizability, the online administration of our survey allowed it to be conducted in a completely anonymous fashion. This significantly reduced the likelihood of social desirability bias and is an important strength of the study. While anonymous participation can also, in theory, enable a single person to complete more than one survey, there was no incentive to do so and completion of the survey was relatively time-intensive (~ 10-15 min on average). Therefore, duplicate survey responses or other spurious results related to external incentives are unlikely.
In summary, our results support the suggestion that SOPVs play an important role in MSM sexual networks in Perú. This may be particularly pronounced compared to settings where young adults tend to leave the family home at a younger age, or where stigma is a less prominent driver of sexual decision-making. Both SOPV attendance and the use of online platforms to meet sex partners appear to be highly prevalent behaviors among MSM in Lima. Furthermore, our findings indicate that MSM who attend SOPVs may be at particularly high risk for HIV/STI transmission, underscoring an opportunity to work with SOPVs to develop interventions that will expand access to testing, treatment, and prevention services. Although access to PrEP is relatively limited at present time in Perú, as it becomes more available partnerships with SOPVs could be leveraged to promote linkage to PrEP providers or even facilitate medication distribution. Importantly, our results suggest SOPV-based interventions would be accepted by most MSM in Lima who frequent these venues. Overall, these findings have important public health implications and suggest that SOPVs in Lima are suitable sites for targeted HIV testing and prevention interventions.
Conclusions
Among MSM in Lima, SOPV attendance appears to be common and SOPV attendees may be at higher risk for HIV transmission compared to MSM in general. SOPV-based outreach may be an acceptable strategy to deliver sexual health interventions in this community, and SOPVs may be ideal points of contact where MSM in high-risk sexual networks – including those who meet partners online – could be reached for HIV testing. Our findings support further development of targeted SOPV-based interventions as a way to increase access to HIV testing, treatment, and prevention services for MSM in Perú.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MSM:
-
Men who have sex with men
- SOPV:
-
Sex-on-premise venue
- TW:
-
Transgender women
- WHO:
-
World Health Organization
- ART:
-
Antiretroviral treatment
- PrEP:
-
Pre-exposure prophylaxis
- STI:
-
Sexually transmitted infection
- HIC:
-
High-income country
- LMIC:
-
Low/middle-income country
- PR:
-
Prevalence ratio
- CI:
-
Confidence interval
- IQR:
-
Interquartile range
- U=U:
-
Undetectable equals untransmissible
References
Sidibe M. UNAIDS Data. Program HIV/AIDS. 2018;2018:1–376.
Silva-Santisteban A, Raymond HF, Salazar X, Villayzan J, Leon S, McFarland W, et al. Understanding the HIV/AIDS epidemic in transgender women of Lima, Peru: results from a Sero-epidemiologic study using respondent driven sampling. AIDS Behav. 2012;16(4):872–81.
Passaro RC, Haley CA, Sanchez H, Vermund SH, Kipp AM. High HIV prevalence and the internet as a source of HIV-related service information at a community-based organization in Peru: a cross-sectional study of men who have sex with men. BMC Public Health. 2016;16(1):871.
Lama JR, Brezak A, Dobbins JG, Sanchez H, Cabello R, Rios J, et al. Design strategy of the sabes study: diagnosis and treatment of early HIV infection among men who have sex with men and transgender women in Lima, Peru, 2013-2017. Am J Epidemiol. 2018;187(8):1577–85.
Allan-Blitz L-T, Herrera MC, Calvo GM, Vargas SK, Caceres CF, Klausner JD, et al. Venue-based HIV-testing: an effective screening strategy for high-risk populations in Lima. Peru AIDS Behav. 2019;23(4):813–9.
Castillo R, Konda KA, Leon SR, Silva-Santisteban A, Salazar X, Klausner JD, et al. HIV and sexually transmitted infection incidence and associated risk factors among high-risk MSM and male-to-female transgender women in Lima, Peru. J Acquir Immune Defic Syndr. 2015;69(5):567–75.
Villaran M, Brezak A, Ahmed S, Ulrich A, Duerr A, Herbeck J, et al. A study of potential HIV transmission hotspots among men who have sex with men and transgender women in Lima, Peru. J Int AIDS Soc. 2016;19(Supplement 5):98–9.
Ministerio de Salud del Peru. Situación epidemiológica del VIH-Sida en el Perú. Bol VIH Mens del Cent Nac Epidemiol Prevención y Control Enfermedades. 2018.
Vargas V. The new HIV/AIDS program in Peru: The role of prioritizing and budgeting for results. Washington, DC: World Bank Group; 2015.
World Health Organization. Guideline on When To Start Antiretroviral Therapy and on Pre-Exposure Prophylaxis for HIV. 2015.
Brazier E, Maruri F, Duda SN, Tymejczyk O, Wester CW, Somi G, et al. Implementation of “treat-all” at adult HIV care and treatment sites in the global IeDEA consortium: results from the site assessment survey. J Int AIDS Soc. 2019;22(7):e25331.
World Health Organzation. Treat All: Policy Adoption and Implementation Status in Countries. HIV Treatment and Care Fact Sheet. 2017.
AIDS Vaccine Advocacy Coalition (AVAC). PrEPWatch. Available from: https://www.prepwatch.org/country/peru/. [cited 2020 Feb 12].
Skarbinski J, Rosenberg E, Paz-Bailey G, Hall HI, Rose CE, Viall AH, et al. Human immunodeficiency virus transmission at each step of the care continuum in the United States. JAMA Intern Med. 2015;175(4):588–96.
Frieden TR, Foti KE, Mermin J. Applying public health principles to the HIV epidemic — how are we doing? Malina D, editor. N Engl J Med. 2015;373(23):2281–7.
Dimitrov D, Wood D, Ulrich A, Swan DA, Adamson B, Lama JR, et al. Projected effectiveness of HIV detection during early infection and rapid ART initiation among MSM and transgender women in Peru: a modeling study. Infect Dis Model. 2019;4:73–82.
Goodreau SM, Carnegie NB, Vittinghoff E, Lama JR, Sanchez J. What drives the US and Peruvian HIV epidemics in men who have sex with men (MSM)? PLoS One. 2012;7(11):50522.
Chow JY, Konda KA, Borquez A, Caballero P, Silva-Santisteban A, Klausner JD, et al. Peru’s HIV care continuum among men who have sex with men and transgender women: opportunities to optimize treatment and prevention. Int J STD AIDS. 2016;27(12):1039–48.
UNAIDS. Ending AIDS Progress Towards the 90-90-90 Targets. Global AIDS Update. 2017.
Lee SW, Deiss RG, Segura ER, Clark JL, Lake JE, Konda KA, et al. A cross-sectional study of low HIV testing frequency and high-risk behaviour among men who have sex with men and transgender women in Lima. Peru BMC Public Health. 2015;15(1):408.
Blas MM, Alva IE, Cabello R, Carcamo C, Kurth AE. Risk Behaviors and Reasons for not Getting Tested for HIV among Men Who Have Sex with Men: An Online Survey in Peru. Thorne C, editor. PLoS One. 2011;6(11):e27334.
Rich KM, Huamaní JV, Kiani SN, Cabello R, Elish P, Arce JF, et al. Correlates of viral suppression among HIV-infected men who have sex with men and transgender women in Lima, Peru. AIDS Care. 2018;30(11):1341–50.
Krueger EA, Chiu CCJ, Menacho LA, Young SD. HIV testing among social media-using Peruvian men who have sex with men: correlates and social context. AIDS Care. 2016;28(10):1301–5.
Sharma M, Ying R, Tarr G, Barnabas R. Systematic review and meta-analysis of community and facility-based HIV testing to address linkage to care gaps in sub-Saharan Africa. Nature. 2015;528(7580):S77–85.
Raj A, Yore J, Urada L, Triplett DP, Vaida F, Smith LR. Multi-site evaluation of community-based efforts to improve engagement in HIV care among populations disproportionately affected by HIV in the United States. AIDS Patient Care STDs. 2018;32(11):438–49.
Suthar AB, Ford N, Bachanas PJ, Wong VJ, Rajan JS, Saltzman AK, et al. Towards Universal Voluntary HIV Testing and Counselling: A Systematic Review and Meta-Analysis of Community-Based Approaches. Sansom SL, editor. PLoS Med. 2013;10(8):e1001496.
Smith LV, Rudy ET, Javanbakht M, Uniyal A, Sy LS, Horton T, et al. Client satisfaction with rapid HIV testing: comparison between an urban sexually transmitted disease clinic and a community-based testing center. AIDS Patient Care STDs. 2006;20(10):693–700.
Campbell CK, Lippman SA, Moss N, Lightfoot M. Strategies to increase HIV testing among MSM: a synthesis of the literature. AIDS Behav. 2018;22(8):2387–412.
Lipsitz MC, Segura ER, Castro JL, Smith E, Medrano C, Clark JL, et al. Bringing testing to the people – benefits of mobile unit HIV/syphilis testing in Lima, Peru, 2007–2009. Int J STD AIDS. 2014;25(5):325–31.
AIDS Council of new South Wales. Sex on premises venue code of practice 2015.
Frank K. Rethinking risk, culture, and intervention in collective sex environments. Arch Sex Behav. 2019;48(1):3–30.
Lyons A, Smith AMA, Grierson JW, Von Doussa H. Australian mens sexual practices in saunas, sex clubs and other male sex on premises venues. Sex Health. 2010;7(2):186–92.
Grov C, Hirshfield S, Remien RH, Humberstone M, Chiasson MA. Exploring the venue’s role in risky sexual behavior among gay and bisexual men: An event-level analysis from a national online survey in the U.S. Arch Sex Behav. 2013;42:291–302.
Grov C. HIV risk and substance use in men who have sex with men surveyed in bathhouses, bars/clubs, and on Craigslist.org: venue of recruitment matters. AIDS Behav. 2012;16(4):807–17.
Meunier É, Siegel K. Sex club/party attendance and STI among men who have sex with men: Results from an online survey in New York City. Sex Transm Infect. 2019;95:584–7.
Binson D, Woods WJ, Pollack L, Paul J, Stall R, Catania JA. Differential HIV risk in bathhouses and public cruising areas. Am J Public Health. 2001;91(9):1482–6.
Lister NA, Smith A, Tabrizi S, Hayes P, Medland NA, Garland S, et al. Screening for Neisseria gonorrhoeae and chlamydia trachomatis in men who have sex with men at male-only saunas. Sex Transm Dis. 2003;30(12):886–9.
Spielberg F, Branson BM, Goldbaum GM, Kurth A, Wood RW. Designing an HIV counseling and testing program for bathhouses. J Homosex. 2003;44(3–4):203–20.
Woods WJ, Lippman SA, Agnew E, Carroll S, Binson D. Bathhouse distribution of HIV self-testing kits reaches diverse, high-risk population. AIDS Care. 2016;28:111–3.
Debattista J, Dwyer J, Anderson R, Rowling D, Patten J, Mortlock M. Screening for syphilis among men who have sex with men in various clinical settings. Sex Transm Infect. 2004;80(6):505–8.
Ko N-Y, Lee H-C, Hung C-C, Chang J-L, Lee N-Y, Chang C-M, et al. Effects of structural intervention on increasing condom availability and reducing risky sexual behaviours in gay bathhouse attendees. AIDS Care. 2009;21(12):1499–507.
Huebner DM, Binson D, Woods WJ, Dilworth SE, Neilands TB, Grinstead O. Bathhouse-based voluntary counseling and testing is feasible and shows preliminary evidence of effectiveness. J Acquir Immune Defic Syndr. 2006;43(2):239–46.
Daskalakis D, Silvera R, Bernstein K, Stein D, Hagerty R, Hutt R, et al. Implementation of HIV testing at 2 new York City bathhouses: from pilot to clinical service. Clin Infect Dis. 2009;48(11):1609–16.
Birrell F, Staunton S, Debattista J, Roudenko N, Rutkin W, Davis C. Pilot of non-invasive (oralfluid) testing for HIV within a community setting. Sex Health. 2010;7:11–6.
Woods WJ, Euren J, Pollack LM, Binson D. HIV prevention in gay bathhouses and sex clubs across the United States. J Acquir Immune Defic Syndr. 2010;55(SUPPL. 2):88–90.
Woods WJ, Sheon N, Morris JA, Binson D. Gay bathhouse HIV prevention: the use of staff monitoring of patron sexual behavior. Sex Res Soc Policy. 2013;10(2):77–86.
Debattista J. Health promotion within a sex on premises venue: notes from the field. Int J STD AIDS. 2015;26(14):1017–21.
Krishnan A, Ferro EG, Weikum D, Vagenas P, Lama JR, Sanchez J, et al. Communication technology use and mHealth acceptance among HIV-infected men who have sex with men in Peru: implications for HIV prevention and treatment. AIDS Care. 2015;27(3):273–82.
Chow JY, Konda KA, Calvo GM, Klausner JD, Caceres CF. Demographics, behaviors, and sexual health characteristics of high risk men who have sex with men and transgender women who use social media to meet sex Partners in Lima. Peru Sex Transm Dis. 2017;44(3):143–8.
Cáceres C, Cueto M, Palomino N. Sexual and Reproductive Rights Policies in Peru: Unveiling False Paradoxes. In: Parker R, Petchesky R, Sember R, editors. SexPolitics - Reports from the Front Lines. Sexuality Policy Watch; 2008. p. 127–66.
Maiorana A, Kegeles S, Salazar X, Konda K, Silva-Santisteban A, Cáceres C. ‘Proyecto Orgullo’, an HIV prevention, empowerment and community mobilisation intervention for gay men and transgender women in Callao/Lima, Peru. Glob Public Health. 2016;11(7–8):1076–92.
Garcia J, Amaya Perez-Brumer G, Robinson C, Clark JL. “And Then Break the Cliché”: Understanding and Addressing HIV Vulnerability Through Development of an HIV Prevention Telenovela With Men Who Have Sex With Men and Transwomen in Lima, Peru. Arch Sex Behav. 2018;3:1995–2005.
Cáceres CF, Aggleton P, Galea JT. Sexual diversity, social inclusion and HIV/AIDS. AIDS. 2008;22(Suppl 2):S45.
REDCap. Available from: https://www.project-redcap.org/. [cited 2019 Nov 30].
Long JE, Ulrich A, White E, Dasgupta S, Cabello R, Sanchez H, et al. Characterizing Men Who Have Sex with Transgender Women in Lima, Peru: Sexual Behavior and Partnership Profiles. AIDS Behav. 2020;24(3):914–24.
OANDA Currency Converter. Available from: https://www1.oanda.com/currency/converter/. [cited 2018 Nov 26].
Torres TS, Konda KA, Hamid Vega-Ramirez E, Elorreaga OA, Diaz-Sosa D, Hoagland B, et al. Factors associated with willingness to use pre-exposure prophylaxis in Brazil, Mexico, and Peru: Web-based survey among men who have sex with men. JMIR Public Heal Surveill. 2019;21(6).
Beymer MR, Weiss RE, Bolan RK, Rudy ET, Bourque LB, Rodriguez JP, et al. Sex on demand: geosocial networking phone apps and risk of sexually transmitted infections among a cross-sectional sample of men who have sex with men in Los Angeles county. Sex Transm Infect. 2014;90(7):567–72.
Devost MA, Beymer MR, Weiss RE, Shover CL, Bolan RK. App-based sexual partner seeking and sexually transmitted infection outcomes: a cross-sectional study of HIV-negative men who have sex with men attending a sexually transmitted infection Clinic in Los Angeles, California. Sex Transm Dis. 2018;45(6):394–9.
Wang H, Zhang L, Zhou Y, Wang K, Zhang X, Wu J, et al. The use of geosocial networking smartphone applications and the risk of sexually transmitted infections among men who have sex with men: A systematic review and meta-analysis 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Public Health. 2018;18(1).
Acknowledgements
We wish to acknowledge the study participants who shared their experiences, time, and effort in order to make this work possible. In addition, we are grateful for the technical support of the REDCap administrative teams at the University of Washington Institute of Translational Health Sciences and the Fred Hutchinson Cancer Research Center.
Funding
This research was supported by a 2018 CFAR International Pilot Award from the University of Washington / Fred Hutch Center for AIDS Research (NIH AI027757); in addition, AL received support as a post-doctoral fellow under the University of Washington STD/AIDS Research Training Grant (NIH T32 AI07140). We also acknowledge funding support related to the use of REDCap to carry out this study (UL1 TR002319, KL2 TR002317, and TL1 TR002318 from NCATS/NIH). None of the funding bodies supporting this research had any role in the study design, data collection, analysis, or interpretation of results.
Author information
Authors and Affiliations
Contributions
AL, HS, JH, RC, and AD all made substantial contributions to the conception and study design for this work. In addition, AL obtained funding, drafted all study materials (including the survey instrument, consent form, and documents for bioethics review), developed and maintained the online survey in REDCap, performed all data analysis, interpreted the results, and drafted the manuscript; HS contributed substantially to development of the survey instrument and documents for bioethics review, led recruitment efforts, and provided substantive interpretation of the results; JH contributed substantially to the acquisition of data and interpretation of results; RC contributed substantially to the acquisition of data and interpretation of results; and AD contributed substantially to the development of study materials and interpretation of data, and provided substantive revision of the manuscript. All authors read and approved the final manuscript submitted for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research underwent full review and was approved by the Vía Libre Comité Institucional de Bioética (3876 [2018a]) and the University of Washington Institutional Review Board (STUDY00005823). All study participants provided informed consent and attested to their eligibility in the form of an electronic signature prior to their participation.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
(AdditionalFile1.pdf): Annotated Survey Instrument. Full-length Spanish-language text of survey instrument used in the study, including transitional text and instructional notes used to guide participants, as well as annotations indicating branching logic; all items are in the same order as they appeared to participants taking the actual online survey in REDCap.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lankowski, A., Sánchez, H., Hidalgo, J. et al. Sex-on-premise venues, associated risk behaviors, and attitudes toward venue-based HIV testing among men who have sex with men in Lima, Perú. BMC Public Health 20, 521 (2020). https://doi.org/10.1186/s12889-020-08604-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-020-08604-w