
Abstract
Background
Sufficient evidence associate body shape to detrimental lifestyle diseases including the metabolic syndrome (MetS). The prevalence of the MetS, as well as effects of the MetS and body shape on body composition, insulin-like growth factor-1 (IGF-1), C-reactive protein (CRP) and sex hormone parameters were investigated in a female farm worker population in the Western Cape.
Methods
Women between the ages of 20–60 years were classified according to the International Diabetes Federation’s definition of the MetS. Assessments included body shape (android/gynoid), blood pressure, anthropometric, bioelectrical impedance analyses and blood analyses for fasting glucose and insulin, lipid profile, IGF-1, CRP, and sex hormone parameters.
Results
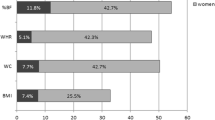
The prevalence of the MetS was 52%, with abdominal obesity 68.8%, hypertension 66.4% and low high density lipoprotein-cholesterol (HDL-c) levels (64.1%) being the more prevalent MetS risk factors. The MetS, irrespective of body shape, was found to be associated with body mass index (p < 0.01), fat mass (%) (p < 0.01), waist circumference (p < 0.001), HDL-c (p < 0.001), systolic blood pressure (p < 0.05) and diastolic blood pressure (p < 0.01). No significant differences were observed for IGF-1, CRP and sex hormone parameters.
Conclusion
The prevalence of the MetS and its individual risk factors were found to be significantly high in this female farm worker population. Additionally, the study showed that the MetS, body shape and/or both could predict differences in body composition, physiological and biochemical parameters in women.
Similar content being viewed by others


Background
Following, and adapting to a westernized lifestyle (unhealthy eating habits, dietary changes and decreased physical activity) has significantly increased in both developed and developing countries globally [1]. This in turn has contributed to an increase in the incidence of obesity and various lifestyle related-diseases [2].
The metabolic syndrome (MetS), regarded as a major risk factor for chronic diseases of lifestyle, consists of a cluster of metabolic, physiological and biochemical risk factors, independently associated with cardiovascular disease, and diabetes mellitus [3]. The main constituents of the MetS include; abdominal obesity, dyslipidaemia, increased arterial blood pressure (systolic and diastolic), insulin resistance (IR) and impaired blood glucose homeostasis, dependent on the MetS definition used [3, 4]. However, due to the complexity of the MetS, there is still no unifying definition, which clearly defines the MetS and its diagnostic criteria [4].
The MetS has been extensively studied in various populations with evidence pointing toward a high prevalence globally, including South Africa [5,6,7,8,9]. There also appears to be sufficient evidence indicating that women present with a higher risk compared to men [7, 8]. More specifically, there is an increase in the prevalence of android body shape observed amongst women, exacerbating the global prevalence of the MetS and its individual components [10].
Body composition, i.e. increased body mass (BM), obesity and android body shape; have been associated with an increased risk for developing metabolic-related diseases, especially in women [10, 11]. An android body shape (apple shape), refers to adipose tissue present in the abdominal compartment, and is characterized with an increase in visceral adipose tissue (VAT), which is normally associated with a worsened metabolic risk factor profile (IR, hypertension, dyslipidaemia and inflammation). The gynoid body shape (pear shape) is mostly associated with adipose tissue distributed around the gluteo-femoral region of the body; however, its relationship with disease risk is still debateable [12, 13].
Generally, adipose tissue seems to be involved in the pathophysiology of the MetS, where it plays a role in sex hormone production, as well as providing a source of low-grade inflammation and hence involved in the development of IR [13, 14]. The MetS is characterised by a deregulated adipokine profile (increased interleukin-6 and C-reactive protein (CRP)), which in turn leads to chronic low-grade inflammation [14, 15]. Since adipokines has such diverse functions, a dysregulation in the synthesis of these adipokines and their actions in relation to obesity, have been linked to the MetS [16]. Furthermore, the MetS is also characterised by excessive androgen (decreased sex hormone binding globulin (SHBG) and increased testosterone) synthesis via the increased conversion of oestrogens and androgenic precursors in adipose tissue [17]. It has furthermore been hypothesised that the MetS is also associated with increased insulin-like growth factor-1 (IGF-1) synthesis, which can exacerbate the development of the individual MetS risk components [18]. The role of the MetS as a single entity and/or its components in inflammation, sex hormones and growth factors however still needs to be elucidated, since no single component can explain the complexity of the MetS pathophysiology.
Despite this, no MetS prevalence data exist for women in a farm working environment as well as the individual components in the Western Cape region of South Africa. Therefore, determining the prevalence of the MetS in this specific population as well as region of South Africa, will partly enable us to describe, understand and resolve associations of the MetS, and provide significant insights into the extent of the MetS in the Western Cape. The primary aim was to first describe the prevalence of the MetS in this female farm worker population, and then to classify these women based on their body shape, body composition, as well as selected biochemical parameters.
Methods
Study design, ethical considerations and recruitment
Ethical approval was obtained from the Human Research Ethics Committee of Stellenbosch University (protocol number N13/04/052). A cross-sectional, baseline descriptive study design was followed between March until July 2015.
Farming communities were identified, after which farm workers from three different wine estates including, Villiera at the Owethu Clinic (Stellenbosch), Neethlingshoff (Stellenbosch), and Solms-Delta Wine Estate (Franschhoek), were invited to attend information sessions regarding the specific research project. Farm workers could volunteer to participate, where after visitations were scheduled for each volunteer on different days during the week. At each scheduled visitation, the researcher verbally explained to the participant what was expected of them during the data collection process, and that there would be a time investment of approximately 30 min. Participants were given sufficient time to thoroughly read through the participant information leaflet and consent form, after which they were free to ask any questions. After reading through the informed consent form, written informed consent was obtained from all volunteering participants based on inclusion criteria. Participants were informed that they could withdraw at any time point, and were assured of their anonymity and confidentiality within the study.
Body composition assessments
Body mass was measured using a Seca 634 automatic scale (Seca, United Kingdom, Birmingham, England) to the nearest 0.01 kg. Height was measured using a portable, standard stadiometer (Leicester™; Leicester, England), assuming the correct anatomical stance, to the nearest 0.1 cm. The body mass index (BMI) (kg/m2) was calculated using these base measurements. Waist circumference and hip circumference were assessed to the nearest 0.1 cm using a Lufkin tape measure (Lufkin, USA). Waist-to-hip ratio (WHR) was subsequently calculated using these measures.
Bio-electrical impedance analysis (BIA) measurements were performed using the multi-frequency Bioscan 920 II analyser (Maltron 920, UK), to assess fat mass (%) and muscle mass (kg).
Body shape was estimated using the WHR ratio as well as visual inspection of the volunteers standing in the anatomical position as being either android or gynoid. We excluded n = 7 due to inability to align calculated WHR with the visual presentation of the body shape.
Study population
For this part of the study population, volunteering apparently healthy women between the ages of 20–60 years were included. Inclusion criteria included volunteers had to be, (i) women between the ages of 20–60 years old, (ii) residing in the Western Cape Province (Winelands region), (iii) all included women had to have all parameters for this part of the study measured, and (iv) must have been able to provide informed consent. Those who were excluded were either younger, or older than 20–60 years, not usual residents from the WestCape Province, pregnant or lactating at the time of data 132#?>collection, or excluded due to missing parameters as a result of technical issues.
Selection of participants
The total number of successfully recruited volunteering participants (which initially included both men and women) were n = 191. From this sample, a sub-sample was drawn in which n = 63 were excluded; n = 42 men for this particular part of the study, n = 2 women who had withdrawn consent due to time constraints, n = 7 women due to the inability to classify their body shape, and n = 12 due to technical errors in data collection for the BIA measurements.
Stratified sub-sampling and metabolic syndrome classification
Of the remaining n = 128 women, the group was subsequently classified using International Diabetes Federation (IDF) criteria as having the MetS. This definition includes the compulsory elevated waist circumference (WC) (≥ 80 cm for women), plus any two of the following components: (i) elevated blood pressure (systolic blood pressure (SBP) ≥ 130 mmHg, and diastolic blood pressure (DBP) ≥ 85 mmHg), (ii) elevated fasting blood glucose (FBG) (≥ 5.6 mmol/L), (iii) low high density lipoprotein-cholesterol (HDL-c) (< 1.3 mmol/L for women) or elevated triglycerides (TG) (≥ 1.7 mmol/L) [19]. Applying this classification, a total of n = 66 women were classified as having the MetS, while n = 62 participants were classified into a non-MetS group.
Female participants within these two respective groups were further classified according to body shape (gynoid or android), to render the four respective groups: MetS with gynoid body shape (MetSG) (n = 29), MetS with android body shape (MetSA) (n = 37), non-MetS with gynoid body shape (NMetSG) (n = 50), and non-MetS with android body shape (NMetSA) (n = 12).
Due to logistical reasons and time constraints, only n = 80 could be included for data and laboratory analyses. This sub-sample was randomly selected from the total n = 128, however, for the NMetSA group all were included. The n = 80 women were randomly allocated to the specific subgroups as follows: MetSG (n = 23), MetSA (n = 23), NMetSG (n = 22) and NMetSA (n = 12).
Blood pressure
Blood pressure was measured in duplicate on the right arm, using a calibrated aneroid sphygmomanometer (Erka Perfect Aneroid 48, Germany), and stethoscope (Littmann 3 M stethoscope, USA) with an appropriate sized cuff after a stabilising period of ten minutes in a sitting position.
Blood sampling and analysis
Plasma blood glucose, serum insulin and a full blood lipid profile were assessed through the chemical PathCare laboratories (Stellenbosch) to assist in classify women as having the MetS or not. Female serum testosterone, sex hormone binding globulin (SHBG) and free androgen index (FAI) were also assessed. Highly sensitive enzyme linked immunosorbent assay (ELISA) kits were used to quantify CRP (CRP human simple set ELISA kit®, Abcam, UK) [20], and IGF-1 concentration (IGF-1 human ELISA kit®, Abcam, UK) [21]. Serum samples were diluted 25,000 times for CRP, and 20 times for IGF-1. The optical densities of all participant samples were measured using an EL800 universal microplate reader (Bio-tek Instruments, South Africa) at 450 nm, within 15 min after the stop solution was added.
Statistical analysis
All data was analysed using Statistica Software version 12 (StatSoft, Inc., USA). Significance was accepted at p < 0.05. All normally distributed results are reported as means and 95% confidence intervals (CI), and not normally distributed results as medians and interquartile ranges (IQR). For normally distributed data, student t-tests were performed to determine the difference in variables between two groups. Factorial analysis of variance (ANOVA) with Bonferonni post hoc test was done to establish significance between the four respective groups. The Mann-Whitney U test was employed to determine the difference in variables between two groups, and a one-way Kruskal-Wallis ANOVA was performed to determine the difference in variables between all the study groups, for data that was not normally distributed.
Results
Prevalence
From the total sample (n = 128 women), n = 66 women were identified with the MetS (52%), while n = 62 did not present with the MetS (48%). For all the women in this study (n = 128), the most prevalent individual risk factor was a high WC (68.8%, n = 88), followed by elevated blood pressure (BP) (66.4%, n = 85), and low HDL-c levels (64.1%, n = 82), with approximately 26.6% presenting with elevated TG levels (n = 34), and 25.8% with elevated FBG (n = 33).
Anthropometric characteristics
In the subsample (n = 80), women in the MetS group were significantly older (40.1 (8.9–13.5) vs 32.2 (6.4–10.4) years, p = 0.00056), and also displayed a significantly higher BM, BMI, WC, WHR, and fat mass (%) (p < 0.001 for all, except WHR: p = 0.02), compared to the non-MetS counterparts (Table 1). With reference to BMI (Fig. 1), approximately two thirds of the MetS population were classified as obese (67.0%), and 31.0% as overweight, (Fig. 1a). In the non-MetS group, 47.0% of the females were overweight and 21.0% were obese (Fig. 1b).

Distribution of women in (a) the MetS and (b) the non-MetS groups according to the respective BMI categories. MetS-metabolic syndrome, non-MetS-non-metabolic syndrome
Biochemical blood parameters
In the subsample (n = 80), women with the MetS revealed significantly higher fasting insulin (p = 0.02), and FAI (p = 0.03), while SHBG were significantly lower compared to their non-MetS counterparts (p = 0.0083) (Table 2). All other parameters were found to be not significantly different (Table 2).
When considering the association of both metabolic status and body shape on various blood-specific parameters compared between the four respective groups, no significant differences were reported for CRP, IGF-1, female testosterone, or SHBG (Fig. 2a-d). However, even though no significance was observed, women with the MetS (irrespective of body shape) displayed at least a 1.5 fold higher CRP level (Fig. 2a), compared to their non-MetS group. Women in both the non-MetS groups displayed a 1.7 fold higher SHBG level compared to their MetS counterparts (Fig. 2d).

Blood analyses for (a) CRP, (b) IGF-1, (c) female Testosterone and (d) SHBG for the different body shape and metabolic status groups. The dotted lines represent normal cut-off criteria [37]. CRP-C-reactive protein, IGF-1-insulin-like growth factor-1, MetS-metabolic syndrome, Non-MetS-non-metabolic syndrome, SHBG-Sex hormone binding globulin, T-female testosterone
Differences between respective groups according to both metabolic syndrome and body shape
For a more thorough investigation into the association of metabolic status and body shape, various anthropometric, BIA and blood-specific parameters were compared between the four respective groups (n = 80): MetSA, MetSG, NMetSA and NMetSG.
Body composition
Women in both MetS groups (irrespective of body shape) (Fig. 3a and b) showed significantly higher BM and BMI compared to the non-MetS groups (p < 0.01), whereas women in the NMetSA group showed a significantly higher WHR compared to those from the NMetSG group (p = 0.0003) (Fig. 3c). A significantly higher fat mass (%) (Fig. 3e) was observed in the MetSG group compared to the NMetSG group (p = 0.003). No differences were observed for muscle mass between any groups (Fig. 3d).

Body composition measurements for (a) BM, (b) BMI, (c) WHR, (d) Muscle mass, and (e) Fat mass (%). The dotted lines represent normal cut-off criteria [38]. BM-Body mass, BMI-Body mass index, MetS-metabolic syndrome, non-MetS-non-metabolic syndrome, WC-waist circumference, WHR-waist-hip-ratio
MetS risk factor measurements
Women in the MetSG group displayed a significantly larger WC compared to the NMetSG counterparts (p = 0.000002) (Fig. 4a), while the WC for the NMetSA group was significantly larger than that of the NMetSG group (p = 0.000007) (Fig. 4a). No significant differences were observed for FBG between any groups (Fig. 4b). The women in the MetSG group furthermore showed both a significantly lower HDL-c and elevated TG levels compared to the women in the NMetSG group (p = 0.000008 for HDL-c, and p = 0.03 for TG) (Fig. 4c and d). No other significant differences were observed for HDL-c, but TG levels were also significantly higher in the MetSA group vs the NMetSA group (p = 0.04) (Fig. 4c and d). The MetS groups displayed significant higher SBP and DBP vs the non-MetS groups, irrespective of body shape (Fig. 4e and f).

MetS risk factors according to IDF criteria for (a) WC, (b) FBG, (c) HDL-c, (d) TG, (e) SBP, and (f) DBP. The dotted lines represent IDF cut-off criteria (IDF, 2006). DBP-diastolic blood pressure, FBG-fasting blood glucose, HDL-c- high density lipoprotein-cholesterol, MetS-metabolic syndrome, non-MetS-non-metabolic syndrome, SBP-systolic blood pressure, TG- triglyceride, WC- waist circumference
Discussion
Prevalence
More than 50% of the women in the current study (total population) were categorized with the MetS, which is considerably higher than what was previously reported by international [5, 8, 9], as well as other South African studies [6, 7]. Our results confirmed data reported in a local South African-based study [22], where it was shown that the prevalence (IDF criteria) of the MetS in a Capetonian urban black women population to be even higher (67.8%), however, the current population was specifically from farm working communities. The current study also reports that abdominal obesity (measured by WC) (68.8%), elevated blood pressure (66.4%) and decreased HDL-c (64.1%) were the most prevalent MetS risk factors, which is comparable to other South African studies [6, 7].
Studies have further proposed that abdominal obesity might be responsible; either independently, or through the induction of insulin resistance (via inflammatory mediators released from adipose tissue), to contribute to both the development of systemic hypertension and dyslipidaemia [6, 7, 16]. Since our population presented with an increased WC and overall higher prevalence of overweight, and obesity, this notion could also be plausible in this study. Obesity thus poses a major health problem in South African farm working women and may even predispose individuals to develop the MetS if it overlaps with other MetS risk factors. Since limited evidence exist with regards to the prevalence of the MetS, as well as its individual components in this study population as well as specific region, this study enabled us to partly describe and gain insight on the extent of the MetS in the Western Cape amongst women from farm working communities. It also allowed us to make substantial contributions regarding initiatives required to counter-act the rising prevalence of the MetS by increasing the awareness of the importance metabolic health in terms of health implications. Appropriate and cultural sensitive interventions are currently being developed to help address these public health issues.
Additionally, we determined if metabolic dysfunction and body fat distribution could predict differences in body composition, physiological and various blood (inflammatory, growth factor and steroid sex hormones) parameters to help identify the underlying pathophysiology, and/or associations.
Body composition
We reported significantly higher BM, BMI, WC, WHR and fat mass (%) in the MetS groups compared to their non-MetS counterparts, which is well supported by others [23, 24]. During a chronic positive energy state, adipose tissue stores excess energy in the form of TG in adipocytes, this adipose tissue becomes dysfunctional (hyperplasia/hypertrophy) and eventually leads to an increase in fat mass [16]. A change in fat free mass may lead to changes in insulin sensitivity and glucose disposal, which contribute towards the development of the MetS and its components [25], which further exacerbate metabolic dysfunction.
Physiological and blood parameters
Women in the MetS group showed significantly higher fasting insulin and FAI, while SHBG were significantly lower. Studies have suggested that the altered sex hormone profile may be ascribed to obesity and IR/hyperinsulinemia, which in turn can decrease oestrogen production and increase FAI by directly decreasing SHBG levels [17, 26, 27]. This might be a plausible explanation for our population, since the fasting insulin levels were also significantly higher in the MetS group.
Metabolic syndrome showed associations on certain body compositional and MetS risk factor measurements in women with either gynoid or android body shapes
Evidence suggests that body shape, rather than total adiposity, potentially show strong clinical significance in the development of the MetS [10]. The android body shape is characterized by the presence of large abdominal fat deposits [12], whereas anthropometric indices (WC and WHR) increase as a result of an increase in VAT and subcutaneous adipose tissue [13]. These body composition changes, especially those associated with VAT, can therefore also increase the risk to for the MetS [10].
In the current study, the MetS showed a relationship on certain body compositional and MetS risk factors measurements in both body shape groups (android and gynoid). These discrepancies may be due to the following: firstly, our study had a relatively small sample size, which could have affected the statistical power, therefore did not reveal differences. Secondly, women in both the android and gynoid groups had relatively high BMIs, and we speculate that this could have accounted for the lack of differences in body compositional and blood parameters as seen in this study.
IGF-1 axis: Metabolic syndrome and body shape combined does not predict differences in IGF-1
Adipose tissue distribution seems to play a role in the pathophysiology of the MetS through a correlation on growth factor levels [18]. Evidence on IGF-1 in relation to metabolic diseases is still controversial, i.e. low levels of IGF-1 have been suggested to have beneficial effects on glucose homeostasis and may also sensitise insulin actions, thereby decreasing metabolic disease risk [28]. Friedrich et al. (2013) showed that participants with the MetS had significantly higher IGF-1 levels vs healthy age-matched controls [18], whereas no significant differences were observed for IGF-1 between any of the respective groups in the current study, which is in agreement with the findings of Kabir et al. (2010) [29]. This suggests that although free IGF-1 may change due to adiposity, total IGF-1 remains within the reference range [30], and therefore remain unchanged. In addition, the observation of “no difference” includes the variability of IGF-1 levels found in this sample population. It should also be noted that IGF-1 levels are sensitive to age, gender, ethnic background, as well as degree of obesity [28].
Inflammation: Metabolic syndrome and body shape does not predict differences in CRP
Adipose tissue distribution is also proposed to have a primary role in the pathophysiology of the MetS by affecting inflammatory mediators [32,33,34]. The MetS is characterized by a deregulated inflammatory profile, leading to a persistent low-grade inflammatory state [15]. An increase in pro-inflammatory markers in obesity [31], android body shape [32] and the MetS [15] have been well documented. One proposed mechanism states that an increase in adipose tissue, as a result of adipose tissue dysfunction and adipokine deregulation, can lead to an increase in interleukin-6 synthesis. This regulates hepatic CRP-synthesis and thereby increases CRP levels [33]. Seeing that these adipokines have such diverse functions, a dysregulation in the synthesis of these adipokines and their actions, in relation to obesity, have been linked to the MetS and its individual components [31, 32].
The current study contradicts this evidence, since we did not report any association between MetS, or body shape, on CRP levels, even though clear differences were observed for other body compositional measures of obesity. It is plausible that similar reasons could be at play for the no differences observed in IGF-1. Although no significance was observed, we did however observe the mean CRP levels in the MetS groups to be greater than 10 mg/L. This concentration is indicative of an underlying systemic infection and/or low-grade inflammation. Evidence shows that CRP levels greater than 10 mg/L in obesity have been documented and may be associated with overweight/obesity [34]. Thus, the increased CRP levels in the MetS group could be attributed to either being overweight/obese, an underlying systemic infection, or both; however, more research is needed to clarify these results.
Sex hormone profile: Both metabolic syndrome and body shape does not predict variances in female T and SHBG
The MetS is characterized by an altered sex hormone profile, i.e. an increase in androgen concentration, increased female testosterone, FAI and decrease in SHBG [17, 26]. Androgen surplus has been associated with an increase in VAT and an android body shape, which increases the risk to develop the MetS [10, 17].
As a result of obesity, and its association with hyperinsulinemia, female testosterone can increase with a concomitant decrease in SHBG by having an effect on hepatic synthesis of SHBG [27]. However, no differences were observed for female testosterone, SHBG, as well as FAI. Since, hyperinsulinemia/hyperglycaemia has been shown to affect the sex hormone profile [35], the no differences observed for insulin and glucose; might explain the “no differences” observed for all the sex hormone parameters measured. Other confounding factors could include age, menopausal status, obesity, ovarian failure, polycystic ovarian syndrome, as well as the small sample size [36].
This current study provides significant contributions towards existing literature. To our knowledge, this is the first study to assess the prevalence of the MetS and its individual risk factors in a female farm working population in South Africa. It furthermore emphasized the problem of obesity in this gender specific South African farm working population, and the pathophysiology of the MetS in relation to adiposity and its distribution by including several factors (metabolic, growth and inflammatory factors, as well as sex hormone parameters), and measures of adiposity.
Although the current study has enabled us a better understanding of the MetS, the study was limited by the following: (i) the cross-sectional nature of the study hindered us to generalize our findings to the total population, or elucidate a causal relationship; (ii) CRP is a non-specific marker of inflammation; and (iii) the WC cut-off values used are not South-African specific. Lastly, we do acknowledge that each sub-group should at least consisted of n = 30 participants per group, to obtain a power of 80%, according to post-hoc sample size analysis. For future investigation we propose to include both pro- and anti-inflammatory markers, i.e. interleukin-6, interleukin-10 and TNF-alpha, combined with a full white blood cell count to rule out acute or chronic infections. We propose to include factors that could have confounded the sex hormone parameters including menstrual phase, age, menopausal status and parity.
Conclusion
The prevalence of the MetS and its individual risk factors were found to be considerably high in this female farm worker population. Women with the MetS displayed a significantly exacerbated body composition and sex hormone profile. In addition, the MetS and body shape combined showed a relationship with certain body composition, physiological, as well as biochemical blood parameters, which in turn could exacerbate metabolic dysfunction. Although the effect of both metabolic status and body shape on inflammation, growth factors and sex hormone levels remains inconclusive, women need to recognize the burden of obesity and its associated metabolic dysfunction, and should be motivated to make changes regarding their metabolic health. Interventions should therefore be employed that are focused on metabolic health, which focusses specifically on exercise and nutrition in order to address the current status of the MetS in a culturally sensitive South African setting.
Abbreviations
- ANOVA:
-
Analysis of variance
- BEER:
-
Bio-electrical impedance analysis
- BM:
-
Body mass
- BMI:
-
Body mass index
- CANSA:
-
Cancer Association of South Africa
- CI:
-
Confidence intervals
- CRP:
-
C-reactive protein
- DBP:
-
Diastolic blood pressure
- ELISA:
-
Enzyme-linked immunosorbent assay
- DO:
-
Free androgen index
- FBG:
-
Fasting blood glucose
- HDL-c:
-
High-density lipoprotein-cholesterol
- IDF:
-
International Diabetes Federation
- IGF-1:
-
Insulin-like growth factor-1
- IQR:
-
Interquartile range
- IR:
-
Insulin resistance
- MetS:
-
Metabolic syndrome
- MetSA:
-
Metabolic syndrome android group
- MetSG:
-
Metabolic syndrome gynoid group
- NMetS:
-
Non-metabolic syndrome group
- NMetSA:
-
Non-Metabolic syndrome android group
- NMetSG:
-
Non-Metabolic syndrome gynoid group
- NRF:
-
National Research Foundation
- SBP:
-
Systolic blood pressure
- SEM:
-
Standard error of the mean
- SHBG:
-
Sex hormone binding globulin
- TG:
-
Triglycerides
- VAT:
-
Visceral adipose tissue
- vs:
-
Versus
- WC:
-
Waist circumference
- WHR:
-
Waist-hip-ratio
References
Oggioni C, Lara J, Wells JC, Soroka K, Siervo M. Shifts in population dietary patterns and physical inactivity as determinants of global trends in the prevalence of diabetes: an ecological analysis. Nutr Metab Cardiovasc Dis. 2014;24:1105–11.
World Health Organization. Global status report on non-communicable diseases. 2014. http://apps.who.int/iris/bitstream/10665/148114/1/9789241564854_eng.pdf?ua=1. Accessed 20 Aug 2015.
Kaur J. A comprehensive review on metabolic syndrome. Cardiol Res Pract. 2014. https://doi.org/10.1155/2014/943162.
Kassi E, Pervanidou P, Kaltsas G, Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med. 2011. https://doi.org/10.1186/1741-7015-9-48.
Bhanushali CJ, Kumar K, Wutoh AK, Karavatas S, Habib MJ, Daniel M, et al. Association between lifestyle factors and metabolic syndrome among African Americans in the United States. J Nutr Metab. 2013. https://doi.org/10.1155/2013/516475.
Motala AA, Esterhuizen T, Pirie FJ, Omar MA. The prevalence of metabolic syndrome and determination of the optimal waist circumference cut-off points in a rural south African community. Diabetes Care. 2011;34:1032–7.
Peer N, Lombard C, Steyn K, Levitt N. High prevalence of metabolic syndrome in the black population of cape town: the cardiovascular risk in black south Africans (CRIBSA) study. Eur J Prev Cardiol. 2015;22:1036–42.
Prasad DS, Kabir Z, Dash AK, Das BC. Prevalence and risk factors for metabolic syndrome in Asian Indians: a community study from urban eastern India. J Cardiovasc Dis Res. 2012;3:204–11.
Tran A, Gelaye B, Girma B, Lemma S, Berhane Y, Bekele T, et al. Prevalence of metabolic syndrome among working adults in Ethiopia. Int J Hypertens. 2011. https://doi.org/10.4061/2011/193719.
Momesso DP, Bussade I, Lima GA, Fonseca LP, Russo LA, Kupfer R. Body composition, metabolic syndrome and insulin resistance in type 1 diabetes mellitus. Arq Bras Endocrinol Metabol. 2011;55:189–93.
Wiklund P, Toss F, Weinehall L, Hallmans G, Franks PW, Nordström A, et al. Abdominal and gynoid fat mass are associated with cardiovascular risk factors in men and women. J Clin Endocrinol Metab. 2008;93:4360–6.
Okosun IS, Seale JP, Lyn R. Commingling effect of gynoid and android fat patterns on cardio metabolic dysregulation in normal weight American adults. Nutr Diabetes. 2015. https://doi.org/10.1038/nutd.2015.5.
Suba Z. Circulatory estrogen level protects against breast cancer in obese women. Recent Pat Anticancer Drug Discov. 2012;8:154–67.
Cefalu WT. Inflammation, insulin resistance, and type 2 diabetes: back to the future? Diabetes. 2009;58:307–8.
den Engelsen C, Koekkoek PS, Gorter KJ, van den Donk M, Salomé PL, Rutten GE. High-sensitivity C-reactive protein to detect metabolic syndrome in a centrally obese population: a cross-sectional analysis. Cardiovasc Diabetol. 2012. https://doi.org/10.1186/1475-2840-11-25.
Zhao D, Liu H. Adipose tissue dysfunction and the pathogenesis of metabolic syndrome. World J Hypertens. 2013;3:18–26.
Weinberg ME, Manson JE, Buring JE, Cook NR, Seely EW, Ridker PM, et al. Low sex hormone-binding globulin is associated with the metabolic syndrome in postmenopausal women. Metabolism. 2006;55:1473–80.
Friedrich N, Nauck M, Schipf S, Völzke H, Brabant G, Wallaschofski H. Cross-sectional and longitudinal associations between insulin-like growth factor I and metabolic syndrome: a general population study in German adults. Diabetes Metab Res Rev. 2013;29:452–62.
IDF Clinical Guidelines Task Force. Global guideline for type 2 diabetes: recommendations for standard, comprehensive, and minimal care. Diabet Med. 2006;23:579–93.
Abcam. C-Reactive Protein (CRP) Human SimpleStep ELISA Kit. http://www.abcam.com/ps/products/181/ab181416/documents/ab181416%20C%20Reactive%20Protein%20(CRP)_27%20Apr%2015%20(website).pdf. Accessed 10 Jun 2015.
Abcam. IGF1 human ELISA kit. http://www.abcam.com/ps/products/100/ab100545/documents/ab100545%20IGF1%20Human%20ELISA_Kit%20v8%20(website).pdf. Accessed 10 June 2015.
Erasmus RT, Soita DJ, Hassan MS, Blanco-Blanco E, Vergotine Z, Kengne AP, et al. High prevalence of diabetes mellitus and metabolic syndrome in a south African coloured population: baseline data of a study in Bellville, cape town. S Afr Med J. 2012;102:841–4.
Liu P, Ma F, Lou H, Liu Y. The utility of fat mass index vs. body mass index and percentage of body fat in the screening of metabolic syndrome. BMC Public Health. 2013. https://doi.org/10.1186/1471-2458-13-629.
Park BS, Yoon JS. Relative skeletal muscle mass is associated with development of metabolic syndrome. Diabetes & Metab J. 2013;37:458–64.
Zhang P, Peterson M, Su GL, Wang SC. Visceral adiposity is negatively associated with bone density and muscle attenuation. Am J Clin Nutr. 2015;101:337–43.
Ziaei S, Mohseni H. Correlation between hormonal statuses and metabolic syndrome in postmenopausal women. J Family & Reprod Health. 2013;7:63–6.
Simó R, Sáez-López C, Barbosa-Desongles A, Hernández C, Selva DM. Novel insights in SHBG regulation and clinical implications. Trends Endocrinol Metab. 2015;26:376–83.
Gram IT, Norat T, Rinaldi S, Dossus L, Lukanova A, Téhard B, et al. Body mass index, waist circumference and waist-hip ratio and serum levels of IGF-I and IGFBP-3 in European women. Int J Obes. 2006;30:1623–31.
Kabir G, Hossain M, Faruque O, Hassana N, Hassana Z, Nahara Q, et al. Association of serum free IGF-1 and IGFBP-1 with insulin sensitivity in impaired glucose tolerance (IGT). Int J Diabetes Mellit. 2013;2:144–7.
Renehan AG, Frystyk J, Flyvbjerg A. Obesity and cancer risk: the role of the insulin-IGF axis. Trends Endocrinol Metab. 2006;17:328–36.
Kao TW, Lu IS, Liao KC, Lai HY, Loh CH, Kuo HK. Associations between body mass index and serum levels of C-reactive protein. S Afr Med J. 2009;99:326–30.
Schmidt FM, Weschenfelder J, Sander C, Minkwitz J, Thormann J, Chittka T, et al. Inflammatory cytokines in general and central obesity and modulating effects of physical activity. PLoS One. 2015. https://doi.org/10.1371/journal.pone.0121971.
Choi J, Joseph L, Pilote L. Obesity and C-reactive protein in various populations: a systematic review and meta-analysis. Obes Rev. 2013;14:232–44.
Ishii S, Karlamangla AS, Bote M, Irwin MR, Jacobs Jr DR, Cho HJ, et al. Gender, obesity and repeated elevation of C-reactive protein: data from the CARDIA cohort. PLoS One. 2012. https://doi.org/10.1371/journal.pone.0036062.
Hammond GL, Wu TS, Simard M. Evolving utility of sex hormone-binding globulin measurements in clinical medicine. Curr Opin Endocrinol Diabetes Obes. 2012;19:183–9.
Wallace IR, McKinley MC, Bell PM, Hunter SJ. Sex hormone binding globulin and insulin resistance. Clin Endocrinol. 2013;78:321–9.
Kozakowski J, Zgliczyński W. Body composition, glucose metabolism markers and serum androgens-association in women with polycystic ovary syndrome. Endokrynol Pol. 2013;64:94–100.
World Health Organization: Waist circumference and waist–hip ratio. Report of a WHO Expert Consultation. 2008. http://apps.who.int/iris/bitstream/10665/44583/1/9789241501491_eng.pdf. Accessed 10 Feb 2015.
Acknowledgements
The authors wish to thank all participants of the study, as well as all farm managers for granting access to the premises in order to execute this study. We would specifically like to thank Sr Samantha Adams and Sr Nina de Jager from the Owethu Clinic, Mr. Byron Langenhoven from the Pebbles Health Program at the Villiera wine estate for the direct link between the EpiMetS Research Group and the volunteers. We would also like to thank Sr Anna Wium at Neethlingshoff wine estate, and the Solms-Delta Wine Estate trust manager, Mrs. Charlotte van Zyl, health care worker, Magdalene Davids and social worker Charnè Abrahams.
Funding
Work in this laboratory is supported by grants from the Cancer Association of South Africa (CANSA) and the National Research Foundation (NRF) of South Africa. Funding bodies had no role in the study design, data collection, data analysis, interpretation of data and manuscript preparation.
Availability of data and materials
Datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
The principle investigator, TN, was responsible for the protocol development and funding application. Both TN and MK supervised postgraduate students. IM performed and analysed all participant data and was also responsible for all data interpretation. IM wrote the first draft of the manuscript. Both TN and MK contributed to critical revision of the manuscript. IM, MK and TN contributed equally to the preparation and practicability of this study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Human Research Ethics Committee of Stellenbosch University (protocol number N13/04/052), and this study was conducted to meet the standards of the Declaration of Helsinki. Written informed consent was obtained from all volunteering participants based on inclusion criteria. Participants were informed that they could withdraw at any time point, and were assured of their anonymity and confidentiality within the study.
Consent for publication
No individual’ data were used; only group data were reported, thus not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Mentoor, I., Kruger, M. & Nell, T. Metabolic syndrome and body shape predict differences in health parameters in farm working women. BMC Public Health 18, 453 (2018). https://doi.org/10.1186/s12889-018-5378-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-018-5378-9