
Abstract
Background
A school is a learning environment that contributes to the construction of personal values, beliefs, habits and lifestyles, provide convenient settings for the implementation of drug use prevention programs targeting adolescents, who are the population group at highest risk of initiating drug use. The objective of the present study was to investigate the prevalence of factors associated with implementing drug use prevention programs in Brazilian public and private middle and high urban schools.
Methods
The present population-based cross-sectional survey was conducted with a probability sample of 1151 school administrators stratified by the 5 Brazilian administrative divisions, in 2014. A close-ended, self-reported online questionnaire was used. Logistic regression analysis was used to identify factors associated with implementing drug use prevention programs in schools.
Results
A total of 51.1% of the schools had adopted drug use prevention programs. The factors associated with program implementation were as follows: belonging to the public school network; having a library; development of activities targeting sexuality; development of “Health at School Program” activities; offering extracurricular activities; and having an administrator that participated in training courses on drugs.
Conclusions
The adoption of drug use prevention practices in Brazilian schools may be expanded with greater orchestration of schools through specialized training of administrators and teachers, expansion of the School Health Program and concomitant development of the schools’ structural and curricular attributes.
Similar content being viewed by others


Background
School-based prevention programs for adolescent drug use have been developed and implemented in several countries [1]. A school is a learning environment that contributes to the construction of personal values, beliefs, habits and lifestyles at a time when adolescents are more susceptible to reflect on such issues, and this can directly affect the social production of health [2]. From this perspective, schools provide convenient settings for the implementation of drug use prevention programs targeting adolescents, who are the population group at highest risk of initiating drug use [3].
Preventive interventions implemented at the beginning of and throughout adolescence have the potential to reduce the rates of drug use and associated problems in adulthood [4, 5]. This has been demonstrated by efficacy and effectiveness studies of school-based prevention programs in the last decades [6,7,8]. Economic evaluation analyses of the implementation of such programs indicate that school-based preventive interventions produce a savings of US$ 38 for every dollar invested [9].
Studies investigating the presence of preventive programs in schools and their characteristics as well as those seeking to identify possible facilitators and barriers to program implementation are not common but contribute to decision-making that facilitates the future introduction of preventive programs in the school curriculum [5]. In some developed countries, studies on the prevalence of factors associated with the implementation of drug use prevention programs in schools are much more developed than those in Latin American countries such as Brazil. The current discussions in developed countries extend the paradigm by focusing on the level of scientific evidence of school-based programs. For example, some studies were conducted in the United States to establish the prevalence of evidence-based drug prevention programs in schools [10,11,12,13] and to investigate the factors associated with the adoption of programs based on scientific evidence of efficacy or effectiveness [14]. The results showed that less than half of American schools (47%) had an evidence-based drug use prevention program, while in the past decade, most of the schools chose to adopt programs with no established efficacy or effectiveness [12]. Regarding the factors associated with the adoption of a curricular program with scientific evidence of efficacy or effectiveness in American schools, it was found that the larger time dedicated by the leaders in the activities for drug abuse prevention in their schools [15] and the availability of financial resources seem to be associated with the decision to implement programs in schools [16]. Another factor associated with the implementation of programs in schools is the assistance that schools receive from government agencies and the supply of informational materials on prevention [14].
Brazil is a country with continental dimensions and is currently one of the most unequal societies, as shown by a Gini index (calculation used to measure social inequality) of 0.5. Approximately 97.4% of the population aged 6 to 14 years old and 87.7% of the population aged 15 to 19 years old attend school, representing almost universal schooling coverage of children and younger adolescents [17]. In a population-based epidemiological survey conducted with more than 50,000 students aged 10 to 19 years of age from 27 Brazilian state capitals, 60.5% of the sample reported having consumed alcohol at some point in their lives, while 25.5% reported having used illegal drugs and 16.9% reported having used tobacco, thus pointing to a severe social and public health problem within the school environment [18]. While drug use by Brazilian students in the past 30 years has been well documented [18], little is known about the implementation of drug use prevention programs in the country. There is no governmental or scientific information about the existence of these programs in Brazilian schools or even worse, to date this topic has not been studied in developing countries.
Public policies have been formulated in Brazil to target the health of students, including the “Health at School Program” (Programa Saúde na Escola – PSE). The aim of the PSE is to contribute to the integral education of public school students through promoting healthy eating, a culture of peace and humans rights, prevention and reduction of alcohol, drug, and tobacco use and sexual health. However, there are no reports of the implementation of such actions and their characteristics in Brazilian schools [17, 19].
Considering the need to assess the magnitude of the implementation of school-based drug use prevention programs in Brazil, the present study investigated the prevalence of factors associated with the implementation of such programs in public and private middle (grades 6 to 9) and high (grades 10 to 12) schools.
This study examined the demographic characteristics of schools, school structure and curriculum activities. That starting point was the hypothesis that these factors influence the decision making for implementing prevention of drug use in Brazilian schools programs.
Methods
The present population-based cross-sectional survey was conducted with a probability sample of private and public school administrators from the South, Southeast, North, Northeast and Central-West regions, which are the 5 Brazilian administrative divisions according to the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística – IBGE) [20]. For the purposes of the present study, principals, pedagogical supervisors and prevention program coordinators were considered school administrators.
Participants
The study sample was composed of private and public school administrators chosen through random selection, using the lottery method, of schools stratified per administrative division. That means that the sample was self-weighted, considering that participants and replacements were kept proportional according to the sampling universe of each region and school network. Only middle and high schools in urban areas were considered. Schools from rural areas were not included due to the possible lack of internet connection. The National Register of Basic Education Schools, 2012 School Census, was provided by the National Institute for Educational Studies and Research (Instituto Nacional de Estudos e Pesquisas Educacionais - INEP). Thus, the sample universe included 52,065 schools.
The sample size was calculated based on the finite sample universe (n = 52,065), a confidence level of 95%, an absolute error of 3% and a response distribution of 50% (as there were no previous data on the prevalence of prevention programs in Brazilian schools); thus, the required sample was 1046 schools.
Considering potential losses that are common in studies in which data are collected via the Internet [21, 22], the number of participating schools was increased to 2090 to ensure that the minimum estimated sample size would be met despite losses and replacements.
The sample of school administrators was chosen because studies have shown that school leaders, principals and pedagogical coordinators are the main decision-makers regarding the adoption of a drug prevention program [16, 23].
Instrument and variables
A self-report closed-ended questionnaire was answered anonymously over the Internet. The questionnaire included 45 questions that evaluated respondent’s characteristics; school characteristics; health education at school; respondent’s training in drug issues; and processes of decision-making relative to the adoption of drug use prevention programs. Some questions were taken from the questionnaire used in American schools as described by [24], while others were specifically developed to investigate the characteristics of the Brazilian programs; the comprehensibility of these questions was assessed in the pilot study.
The variables related to school structure were extracted from the National Register of Basic Education Schools, 2012 School Census database, which are official governmental data provided by the INEP.
Outcome variable
The outcome variable was “having a drug use prevention program incorporated into the everyday school routine and in the annual school program” (yes/no).
Explanatory variables
The explanatory variables were divided across the following 5 domains: respondent’s demographic data, school demographic data, school structure, curriculum activities performed at the school and organizational factors related to decision-making regarding the adoption of drug use prevention programs.
The respondent demographic variables considered were as follows: gender (male or female); age (categorized in the following ranges: 20–29, 30–39, 40–49, 50–59 and 60–69 years of age); educational level (secondary school, incomplete higher education, complete higher education, graduate education – master/doctoral degree); position (principal, pedagogical supervisor, prevention program coordinator, other); and length of time at the present position, at the school and in education (in years).
The school characteristics were evaluated based on the following variables: school network (public or private), region (Southeast, South, Northeast, North or Center-West), location (capital or interior of the state) and school size (small ≤800 students, medium = 801 to 1600 students, large > 1600 students).
The school structure was analyzed based on whether it had the following (yes/no): computer laboratory, science laboratory, reading room and library.
The curriculum activities were evaluated based on the following binary variables (yes/no): the school develops activities targeting topics related to health, sexuality, eating habits, PSE activities and extracurricular activities, and the school tests new curricula, programs, innovative teaching practices and respondents participate in courses on drugs.
Procedures
The data were collected during the 2014 school year after a pilot study was performed in 2013 with 263 private and public school administrators from São Paulo [25].
All administrators were invited to participate in the study via e-mails sent to the school’s e-mail address using SurveyMonkey software, which sent all messages at once. If no response was received after 4 e-mails, the potential participants were called by telephone and invited to participate in the study, and any questions they had were answered. A total of 1555 telephone calls were made.
Data analysis
In the descriptive analysis, the qualitative variables were summarized as absolute frequencies, percentages and 95% confidence intervals (CI). The data corresponding to numerical variables are expressed as the median and interquartile range. The chi-square test was used in the initial comparison of categorical variables. Logistic regression models were fit to identify the factors associated with the implementation of drug use prevention programs, with the outcome variable being having a prevention program. Explanatory variables related to the respondents’ demographic data, school demographic data, school structure and curriculum activities were analyzed.
The variables were first analyzed separately using univariate logistic regression models. Next, a logistic regression model was fitted. The first model included all variables with p < 0.20 on univariate analysis. Variables without statistical significance were excluded in each domain until the final model, which included only statistically significant variables. The significance level for the hypothesis tests and the final model was set to 5%. The goodness of fit of the final regression model was assessed by use of the Hosmer-Lemeshow test. The results are expressed as the odds ratio (OR) with the corresponding 95% CI. All analyses were performed in Stata 13.
Results
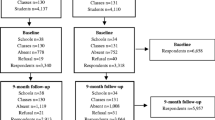
A total of 2090 schools were invited to participate, but 514 did not respond to the invitation. Among the 1576 schools that responded to the invitation, 211 (13,4%) refused to participate. Of the 1151 valid questionnaires, 1136 administrators responded to the outcome question and were included in the analysis (Fig. 1). Table 1 describes respondent characteristics. Most of the participants were school principals, female, and 40 to 49 years of age and had a high educational level. The length of work at the current school varied from less than one to 42 years (median = 8 years). More than half of the respondents had at least 20 years of experience in education and had worked in their current position for more than 4 years.

Flowchart representing the sample of Brazilian schools that participated in the study
A total of 51.1% (95% CI: 48.1–54.0) of schools had incorporated drug use prevention activities into the everyday school routine and pedagogical plan. The demographic and structural characteristics and curriculum activities of the schools, stratified by the presence or absence of drug use prevention programs, are presented in Table 2. Schools from all 5 Brazilian regions participated in the study, though public schools, small schools and schools located in the interior of the states predominated. Most schools had computer laboratories (63.6%), while less than half had a library, science laboratory or reading room. The curriculum of activities performed at the schools included activities regarding student health. The data indicated a high prevalence of activities targeting health, sexuality and eating habits.
Table 3 describes the factors associated with the implementation of drug use prevention programs. The data suggest that public schools, compared with private schools, had 38% greater odds of having a drug use prevention program (OR = 1.38; 95% CI 1.00–1.91). The Northeastern region exhibited the lowest odds of having a prevention program compared to the Southeastern region, which is the region with the largest population (OR = 0.35; 95% CI 0.24; 0.49). The schools’ physical structure was also associated with the presence of prevention programs. Schools with libraries had twice the odds of having a prevention program as those without libraries (OR = 1.73; 95% CI 1.28; 2.35). Conducting activities targeting sexuality (OR = 2,34; 95% CI 1.43; 3.81), offering extracurricular activities (OR = 2.00; 95% CI 1.48; 2.64), performing PSE-oriented activities (OR = 1.98; 95% CI 1.48; 2.69) and having administrators who had attended training courses on drugs (OR = 1.97; 95% CI 1.50; 2.58) were positively associated with the presence of drug use prevention programs.
The Hosmer–Lemeshow goodness-of-fit test p value for the adoption of a drug use prevention program in the school at the final logistic model (Table 3) was 0.420, indicating that the model was adequately adjusted.
Discussion
The present study showed that half of the schools participating in the study utilize a drug use prevention program as part of the school curriculum. The factors associated with implementing drug use prevention programs in schools included the type of school network; Brazilian administrative division; presence of a library in the school; performance of activities targeting sexuality; availability of extracurricular activities (“outside school hours”); performance of PSE-oriented activities; and having administrators who had attended training courses on drugs.
Few international studies have assessed the prevalence of drug use prevention programs that are included as a part of the middle and high school curriculum. The United States, where three-fourths of schools include these programs in the curriculum, has a greater prevalence of such programs than Brazil. This prevalence is the result of political effort, investment and scientific dissemination, which in addition to stimulating the adoption of prevention programs in schools, also contribute to improving the quality of program implementation [12, 26]. Thus, identifying the factors associated with the implementation of drug use prevention programs is fundamental to producing knowledge that increases the prevalence of program implementation. With accurate understanding of the factors that favor the adoption of drug use prevention programs in schools, government and school administrators can formulate guidelines and provide resources to increase the availability of such programs in schools; this implementation is likely to reduce the use of alcohol, tobacco and other drugs among school-attending adolescents [27, 28]. However, studies on the prevalence of factors associated with the implementation of prevention programs do not report program quality and effectiveness; other types of studies are needed for this purpose. This proviso is important because the implementation of a prevention program does not necessarily mean that drug use will effectively be reduced. However, it indicates that the school community is investing effort toward that goal.
The greater participation of public schools in the present study is in accordance with the distribution of public schools in Brazil, as currently 73% of schools are public [29].
In addition, our data showed that public schools, compared with private schools, implemented drug use prevention programs more often. Nevertheless, there is evidence that wealthier adolescents are at high risk for alcohol and drug use in Brazil [30]. The latest Brazilian national survey, which was conducted among 50,890 students at public and private schools from all 27 state capitals, found a greater proportion of students in private schools who used drugs [18]. Data on the prevalence of drug use among students should be effectively disseminated to the administrators of private schools to help dispel the myth that the prevalence of drug use among students from the higher social classes is low, and it may also draw attention to this problem in private schools [14]. It is possible that administrators in wealthier schools may not perceive the need for implementing drug abuse prevention activities [31].
Another factor associated with the demographic characteristic of the school is the region of Brazil that the school is located. Schools in the Northeastern region were less likely to have a prevention program compared to the Southeast region, which is the region with the highest population. Thus, the present study evidences inequalities, among the regions of the country, in relation to the preventive actions to the use of drugs in the Brazilian schools and indicates the need of more significant investment in governmental actions that reach the schools of the country as a whole. Similar findings were identified in another study evaluating school settings in Brazil [32].
Schools’ physical structure also seems to be associated with the implementation of prevention programs. Schools with libraries were more likely to adopt drug use prevention programs than schools without libraries. This finding can suggests that the administrators of such schools are concerned with integral education and thus promote the development of reading habits by students and facilitate their access to information. Information was shown to be protective against drug use [33], and consequently, depending on their collections, school libraries may contribute to the education of students regarding drug use.
Some aspects of the school curriculum were also associated with the adoption of prevention programs. For example, adherence to the federal government’s PSE almost doubled the odds of implementing a drug use prevention program. Within the context of the PSE, schools, aided by healthcare professionals, develop health promotion activities including the encouragement of healthy eating and physical activity and the prevention of drug use [19]. Some evidence indicates that implementing the PSE effectively favors the development of activities for drug use prevention. However, the PSE only operates in public schools, and thus, there is a need to extend its coverage to private schools. In contrast, 28.8% of the schools under PSE orientation have not yet adopted drug use prevention programs, which goes against PSE guidelines and points to the need to supervise what schools offer to their students.
Development of activities for sex education was associated with adoption of drug use prevention programs, suggesting that these schools target more than one high-risk behavior and likely integrate information on drug use with information on sexual behavior. This is relevant because some scientific evidence indicates that high-risk sexual behavior among adolescents is associated with binge drinking (defined as drinking more than five alcoholic drinks on one occasion) and the use of illegal drugs [34]. In addition, because drug use is associated with other high-risk behaviors, the efficacy of programs that integrate these topics is usually greater than that of programs that focus on drug use alone [34, 35].
Regarding the activities available at the schools, one of the main findings of the present study is that drug use prevention programs were more frequently adopted in schools that offered extracurricular activities compared to those that did not. According to a study conducted with 2903 Polish adolescents aged 13 and 14 years old, participation in sports and religious and artistic activities was protective against alcohol consumption [36]. Researchers suggest that this protection derives from the fact that extracurricular activities fill students’ free time and allow them to learn social roles and develop skills that contribute to their positive development [36,37,38], and they may complement the possible protective effects of school-based prevention programs.
Attending training courses was associated with the implementation of prevention programs in schools. In Brazil, the National Secretariat on Drug Policies (Secretaria Nacional de Políticas sobre Drogas - SENAD), at the Ministry of Justice, provides free training courses for education professionals on drug use prevention in schools [39]. In our current study, we found that schools whose administrators participated in drug training courses tended to implement prevention programs more frequently. The training received in such courses by administrators may have alerted to the need to adopt prevention programs or it could be that people who felt strongly about drug education and prevention took a course in that topic and helped implement their school’s inclusion of prevention activities. Alternatively, they may have taken a position at a school that already had implemented prevention activities and then took a course in this topic to help them understand it.
The present study had some limitations. First, data collection through the Internet resulted in a low participation rate among the school principals (approximately 65.3%), and non-participating schools differed from those of participating schools on Brazilian Region and type of school. There was larger losses in North and Central-West region of the country and among private schools. Additionally, there might have been some degree of information bias due to the use of a self-reported questionnaire that could be subjectively interpreted by each respondent. Furthermore, as the study was cross-sectional, we could not infer causality between the associated factors and program implementation because the temporal relationship between them could not be identified.
Finally, the present study was not designed to evaluate the quality of the implemented prevention programs but rather to quantify their presence in a probability sample of Brazilian schools. Thus, future studies should be specifically designed to assess the efficacy and effectiveness of these programs. The results may serve to orient public policies favoring the implementation of preventive programs in developing countries such as Brazil.
Based on the data presented here, we recommend some actions that may contribute to the implementation of future programs in a system-perspective, such as: Production and dissemination of scientific knowledge that may stimulate the adoption of new programs in the country; Favorable political and legislative structure for the implementation of drug prevention programs in the school context; Law enforcement of preventive policies; Training in prevention of drug use by health and education professionals; Commitment of the leaders in relation to the practice of prevention to the use of drugs in the schools; Investment in infrastructure and resources throughout the country; Expansion of public policies for private schooling; Government actions consistent with partnerships with researchers in the area of prevention, to assist in decision making for implementation of a drug prevention program.
Conclusion
The results of the present study suggest that adoption of drug use prevention measures by schools can increase given greater orchestration of the schools through the specialized training of administrators and teachers and the promotion of consistent collaboration between the health and education sectors. This could be encouraged by increasing schools’ participation in programs such as the PSE, with concomitant development of their structural and curricular aspects.
There are several lessons that can be learned from the present study, specially to empower directors and stakeholders who plan to implement a program to prevent drug use in their school or school district. The influence of the school administration on adoption of drug prevention programs was evident in this study. Schools whose administrators/directors had participated in training courses on drugs tend to implement prevention programs more frequently on their schools, suggesting the need to expand the public distribution of such programs in Brazil and in countries with similar educational structure. Besides, some aspects of the school curriculum have been associated with the adoption of prevention programs, such as the concurrent implementation of sexual education activities, availability of extracurricular activities (“outside school hours”) and conducting activities developed by the governmental School Health Program.
Abbreviations
- CAPES:
-
Brazilian Federal Agency for Support and Evaluation of Higher Education
- CI:
-
Confidence Interval
- CNPq:
-
National Council of Scientific and Technological Development
- IBGE:
-
Brazilian Institute of Geography and Statistics
- INEP:
-
National Institute for Educational Studies and Research
- OR:
-
Odds ratio
- PSE:
-
Health at School Program
- SENAD:
-
National Secretariat on Drug Policies
References
Griffin KW, Botvin GJ. Evidence-based interventions for preventing substance use disorders in adolescents. Child Adolesc Psychiatr Clin N Am. 2010;19:505–26.
Aerts D, Alves GG, La Salvia MW, Abegg C. Health promotion: convergence between the principles of health surveillance and socially responsible schools. Cad Saude Publica. 2004;20:1020–8.
Caria MP, Faggiano F, Bellocco R, Galanti MR, Group E-DS. Classroom characteristics and implementation of a substance use prevention curriculum in European countries. Eur J Pub Health. 2013;23:1088–93.
Spoth R, Trudeau L, Redmond C, Shin C. Replication RCT of early universal prevention effects on young adult substance misuse. J Consult Clin Psychol. 2014;82:949–63.
Hopfer S, Davis D, Kam JA, Shin Y, Elek E, Hecht ML. A review of elementary school-based substance use prevention programs: identifying program attributes. J Drug Educ. 2010;40:11–36.
Agabio R, Trincas G, Floris F, Mura G, Sancassiani F, Angermeyer MC. A systematic review of school-based alcohol and other drug prevention programs. Clin Pract Epidemiol Ment Health. 2015;11:102–12.
Foxcroft DR, Tsertsvadze A. Universal alcohol misuse prevention programmes for children and adolescents: Cochrane systematic reviews. Perspect Public Health. 2012;132:128–34.
Catalano RF, Fagan AA, Gavin LE, et al. Worldwide application of prevention science in adolescent health. Lancet. 2012;379:1653–64.
Botvin GJ, Griffin KW. Life skills training: preventing substance misuse by enhancing individual and social competence. New Dir Youth Dev. 2014;2014:57–65.
Ringwalt C, Hanley S, Vincus AA, Ennett ST, Rohrbach LA, Bowling JM. The prevalence of effective substance use prevention curricula in the nation's high schools. J Prim Prev. 2008;29:479–88.
Hanley SM, Ringwalt C, Ennett ST, et al. The prevalence of evidence-based substance use prevention curricula in the nation's elementary schools. J Drug Educ. 2010;40:51–60.
Ringwalt C, Vincus AA, Hanley S, Ennett ST, Bowling JM, Haws S. The prevalence of evidence-based drug use prevention curricula in U.S. middle schools in 2008. Prev Sci. 2011;12:63–9.
Kumar R, O'Malley PM, Johnston LD, Laetz VB. Alcohol, tobacco, and other drug use prevention programs in U.S. schools: a descriptive summary. Prev Sci. 2013;14(6):581–92.
Rohrbach LA, Ringwalt CL, Ennett ST, Vincus AA. Factors associated with adoption of evidence-based substance use prevention curricula in US school districts. Health Educ Res. 2005;20(5):514–26.
Rohrbach LA, Grana R, Sussman S, Valente TW. TYPE II Translation transporting prevention interventions from research to real-world settings. Eval Health Prof. 2006;29:302–33.
Little MA, Pokhrel P, Sussman S, Rohrbach LA. The process of adoption of evidence-based tobacco use prevention programs in California schools. Prev Sci. 2015;16:80–9.
Instituto Brasileiro de Geografia e Estatística - IBGE. Pesquisa Nacional de Saúde do Escolar 2012. Rio de Janeiro: IBGE; 2013.
Carlini E, Noto A, Sanchez Z, Carlini C, Locatelli D, Amato T. VI Levantamento Nacional sobre o Consumo de Drogas Psicotrópicas entre Estudantes do Ensino Fundamental e Médio das Redes Pública e Privada de Ensino nas 27 Capitais Brasileiras. São Paulo: SENAD - Secretaria Nacional de Políticas sobre Drogas; 2010.
Brasil. Decreto n°. 6.286, de 5 de dezembro de 2007: Institui o Programa Saúde na Escola-PSE, e dá outras providências. Diário Oficial da União 2007. https://www.planalto.gov.br/ccivil_03/_ato2007-2010/2007/decreto/d6286.htm. Accessed 02 Mar 2018.
Instituto Brasileiro de Geografia e Estatística - IBGE. Divisão em Regiões. https://ww2.ibge.gov.br/english/geociencias/geografia/default_div_int.shtm?c=1. Accessed 02 Mar 2018.
Granello DH, Wheaton JE. Online data collection: strategies for research. Journal of Counseling & Development. 2004;82:387–93.
Andrews D, Nonnecke B, Preece J. Electronic survey methodology: a case study in reaching hard-to-involve internet users. International journal of human-computer interaction. 2003;16:185–210.
Ringwalt C, Ennett ST, Vincus AA, Rohrbach LA, Simons-Rudolph A. Who’s calling the shots? Decision-makers and the adoption of effective school-based substance use prevention curricula. J Drug Educ. 2004;34:19–31.
Ringwalt CL, Ennett S, Vincus A, Thorne J, Rohrbach LA, Simons-Rudolph A. The prevalence of effective substance use prevention curricula in U.S. middle schools. Prev Sci. 2002;3:257–65.
Pereira AP, Paes Â, Sanchez ZM. Factors associated with the implementation of programs for drug abuse prevention in schools. Rev Saude Publica. 2016;50:44.
Bruckner TA, Domina T, Hwang JK, Gerlinger J, Carpenter C, Wakefield S. State-level education standards for substance use prevention programs in schools: a systematic content analysis. J Adolesc Health. 2014;54:467–73.
Little MA, Sussman S, Sun P, Rohrbach LA. The effects of implementation Fidelity in the towards no drug abuse dissemination trial. Health Educ (Lond). 2013;113
Moreira FG, Silveira DX, Andreoli SB. Knowledge and attitudes related to drug abuse and prevention displayed by public school educators. Rev Bras Psiquiatr. 2009;31:95–100.
Instituto Nacional de Estudos e Pesquisas Educacionais Anísio Teixeira Censo Escolar da Educação Básica. Censo escolar da educação básica 2013. Brasília: INEP; 2013. p. 2014.
Sanchez ZM, Locatelli DP, Noto AR, Martins SS. Binge drinking among Brazilian students: a gradient of association with socioeconomic status in five geo-economics regions. Drug Alcohol Depend. 2013;127:87–93.
Humensky JL. Are adolescents with high socioeconomic status more likely to engage in alcohol and illicit drug use in early adulthood? Subst Abuse Treat Prev Policy. 2010;5:19.
Horta RL, Andersen CS, Pinto RO, et al. Health promotion in school environment in Brazil. Rev Saude Publica. 2017;51:27.
ZvdM S, LGd O, Ribeiro LA, Nappo SA. The role of information as a preventive measure to the drug use among young people at risk. Ciência & Saúde Coletiva. 2010;15:699–708.
Sanchez ZM, Nappo SA, Cruz JI, Carlini EA, Carlini CM, Martins SS. Sexual behavior among high school students in Brazil: alcohol consumption and legal and illegal drug use associated with unprotected sex. Clinics (Sao Paulo). 2013;68:489–94.
Jackson C, Geddes R, Haw S, Frank J. Interventions to prevent substance use and risky sexual behaviour in young people: a systematic review. Addiction. 2012;107:733–47.
Habib EL, Zimmerman MA, Ostaszewski K. International note: prevailing with extracurricular activities in an alcohol-dominated environment: sex differences in resilience among middle school youth. J Adolesc. 2014;37:901–4.
Elder C, Leaver-Dunn D, Wang MQ, Nagy S, Green L. Organized group activity as a protective factor against adolescent substance use. Am J Health Behav. 2000;24:108–13.
Modecki KL, Barber BL, Eccles JS. Binge drinking trajectories across adolescence: for early maturing youth, extra-curricular activities are protective. J Adolesc Health. 2014;54(1):61–6.
Sudbrack MFO, Cestari DM. O modelo sistêmico e da educação para a saúde na prevenção da drogadição no contexto da escola: proposta do Projeto Piloto SENAD/MEC e UNB. In: Proceedings of the 1th Simpósio Internacional do Adolescente; 2005.
Acknowledgements
We thank all the school administrators involved on the study and the study funding agencies.
Funding
The present study was funded by the CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico/National Council of Scientific and Technological Development) grant no. 472991/2012–4 (research support grant for Dr. Sanchez) and CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior/Brazilian Federal Agency for Support and Evaluation of Higher Education) which provided Ana Pereira’s doctoral fellowship. The open access fee was funded by TED 89-2014, from the Brazilian Ministry of Health.
Availability of data and materials
The dataset generated during the current study is available from the corresponding author upon request.
Author information
Authors and Affiliations
Contributions
APDP was responsible for data collection, data analysis and manuscript writing. ZMS was responsible for the conception and design of the study and for the revision of the manuscript. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained from all individual participants included in the study.
The participants, after accessing the link available in the message, were sent to a screen with a complete informed consent and, after reading it, chose to click on “accept” or “not accept”. Participants who agreed to participate were directed to the screen of the questionnaire. The consent form and ethical research procedures were approved by the Ethics Committee of Universidade Federal de São Paulo (no. 250.091).
Consent for publication
Not applicable.
Competing interests
Dr. Sanchez is an Associated Editor at BMC Public Health.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Pereira, A.P.D., Sanchez, Z.M. Drug use prevention: factors associated with program implementation in Brazilian urban schools. BMC Public Health 18, 334 (2018). https://doi.org/10.1186/s12889-018-5242-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-018-5242-y