
Abstract
Background
Health literacy (HL) is defined as necessary competencies to make well-informed decisions. As patients’ decision making is a key element of patient-centered health care, insight in patients’ HL might help healthcare professionals to organize their care accordingly. This is particularly true for people in a vulnerable situation, potentially with limited HL, who are, for instance, at greater risk of having limited access to care [1, 2].
As HL correlates with education, instruments should allow inclusion of low literate people. To that end, the relatively new instrument, HLS-EU-Q47, was subjected to a comprehensibility test, its shorter version, HLS-EU-Q16, was not. Therefore, the goal of this study was to examine feasibility of HLS-EU-Q16 (in Dutch) for use in a population of people with low literacy.
Methods
Purposive sampling of adults with low (yearly) income (< €16,965.47) and limited education (maximum high school), with Dutch language proficiency. Exclusion criteria were: psychiatric, neurodegenerative diseases or impairments. To determine suitability (length, comprehension and layout) participants were randomly distributed either HLS-EU-Q16 or a modified version and were interviewed directly afterwards by one researcher. To determine feasibility a qualitative approach was chosen: cognitive interviews were carried out using the verbal probing technique.
Results
Thirteen participants completed HLS-EU-Q16 (n = 7) or the modified version (n = 6). Questions about ‘disease prevention’ or ‘appraisal’ of information are frequently reported to be incomprehensible. Difficulties are attributed to vocabulary, sentence structure and the decision process (abstraction, distinguishing ‘appraising’ from ‘applying’ information, indecisive on the appropriate response).
Conclusions
HLS-EU-Q16 is a suitable instrument to determine HL in people with limited literacy. However, to facilitate the use and interpretation, some questions would benefit from minor adjustments: by simplifying wording or providing explanatory, contextual information.
Similar content being viewed by others


Background
As health care is increasingly becoming more patient-centered, patients are, sometimes reluctantly, expected to assume more responsibility for their care process. To allow them to take up this responsibility, it is important that they have the necessary competencies to take well-informed decisions [3, 4]. In addition to reading and numerical skills applied in a medical context, this also involves more complex and interconnected abilities, such as acting upon written health information, communicating needs to health professionals, understanding health instructions, applying them correctly to their personal situations, and taking action if needed [5].
These competencies are contained in the concept of health literacy (HL), which can be defined as a person’s knowledge, motivation and competencies to access, understand, appraise, and apply health information in order to make judgments and take decisions concerning health [6]. The importance of HL for health care services and systems is recognized worldwide, and its reach is increasing: while originally the concept was mainly used within health care services, in recent years it is also gaining grounds in public health [3, 7]. A growing number of studies show that people with low HL not only have a lower adherence to medication, poor self-care and worse treatment outcomes, but are also less likely to engage in health promoting behaviour, participate in screening programs, or make use of preventive services [8,9,10,11].
Over the past years, a range of HL measurement tools have been developed, which vary in their approach, design, and purpose [7, 12]. Some tools focus on HL related to specific conditions, such as diabetes, cardiovascular disease, cancer, oral health, or mental health, or on specific population groups, while others are more generic. Some have been developed for the purpose of screening functional HL problems in clinical settings, and are consequently short and easy to use, while others provide an in-depth assessment of HL and its dimensions at population level, using a broader approach [12]. Examples of the first kind of tools are the Rapid Estimate of Adult Literacy in Medicine (REALM) [13, 14], the Newest Vital Sign (NVS) [15], and the Short Assessment of Health Literacy (SAHL) [16]. Examples of the second kind are the Critical Health Competence Test (CHC) [17], the Swiss Health Literacy Survey [13, 18], the Health Literacy Management Scale (HeLMS) [19] and the Health Literacy Questionnaire (HLQ) [20] .
A relatively new measure, which can be used both for screening and for a more in-depth investigation of HL, is the European Health Literacy Survey (HLS-EU-Q). A consortium of European organisations developed this instrument guided by a conceptual model of HL derived from a systematic literature review [7]. The original tool (HLS-EU-Q47) consists of 47 items addressing self-reported difficulties in accessing, understanding, appraising and applying information in tasks concerning decision-making in health care, disease prevention, and health promotion, and was designed for face-to-face or telephone interviewing [21]. A short form (HLS-EU-Q16), comprising 16 of the 47 items, was developed for quicker screening of HL, either through interview or via self-report (pen and paper or online) [22]. Its validation was done via Rasch modelling (1-parametric dichotomous model) and item selection on the basis of content and face validity (item relevance) [22,23,24]. Although no statements regarding sub-dimensions of HL are allowed, HLS-EU-Q16 is a good approximation of the 47-item version, with a high correlation (r = .82) with the general HL score of the HLS-EU-Q47, and a 75.8% concurrent classification of respondents as having insufficient, limited and sufficient HL. HLS-EU-Q16 has been used in several countries, including Belgium [25], the Netherlands [16, 26] and Germany [27, 28].
A major advantage of short self-report measures of health literacy such as HLS-EU-Q16 is that they are relatively easy to administer, both in a clinical setting and at population level, while allowing a comparison with other (patient or general) populations. Some scholars have also used online versions of the tool [25], which is particularly useful for population research involving large samples. However, the downside is that completing a self-report questionnaire requires a certain level of literacy from the respondents. Research by Van der Heide et al. using the HLS-EU-Q47 revealed that limited HL is frequently reported in those with lower levels of education [21, 29]. To allow the inclusion of low literate persons in the survey, the original HLS-EU-Q47 underwent a comprehensibility test for all languages involved, but a similar test was not performed on the short self-report version [21]. Given the difference between a computer-assisted interview and a self-report questionnaire, it is important to ascertain that HLS-EU-Q16 can also reach and detect people with low literacy, as an instrument that is judged to be comprehensive and easy to execute enhances the participation of people and the quality of the measurement.
The aim of this study was to examine the suitability of HLS-EU-Q16 for use in a population of people with low literacy in vulnerable conditions. As this group of people can be expected to have limited health literacy, it is of paramount importance to measure their health literacy adequately. The validation of HLS-EU-Q16 will not be discussed in this research, as it is documented elsewhere.
Methods
To verify the suitability of HLS-EU-Q16 with low literate persons, a feasibility study was performed using a qualitative approach. In this study, the comprehensibility of HLS-EU-Q16 (in Dutch) and of a modified version of the instrument was tested with a group of people with potentially low (health) literacy on account of their education level.
Development of a modified version: HLS-EU-Q16-EZ
To develop a modified version of HLS-EU-Q16, one researcher (HS) examined HLS-EU-Q16 on sentence structure and language. Level 'B1' as defined in the Common European Framework of Reference for Languages was used as a reference, because documents of this level are supposed to be understood by 95% of the population speaking that language [30]. This preliminary analysis was carried out in an intuitive manner, using http://www.zoekeenvoudigewoorden.nl to look up words on B1-level and http://www.accessibility.nl/kennisbank/tools/leesniveau-tool to verify sentence structures. Subsequently, an expert organization on accessible communication (non-profit organization 'Wablieft vzw') was tasked to independently develop an alternative version of the questionnaire, called HLS-EU-Q16-EZ. Questions assessed as too complex (use of jargon or difficult words, subordinate clauses) according to expert organization’s opinion, were rewritten in lay-language and everyday speech. Moreover, the expert organization was instructed to only modify if necessary and, if adjustments were made, to rewrite them with a maximum resemblance to the original formulation.
Selection
Purposive sampling was used to select participants for the study. Inclusion criteria were: being aged between 18 and 70 years, a low level of education (preferably primary school, highest being high school because of the compulsory schooling in Belgium until the age of 18) and low income (defined as a gross family income in the previous year ≤16,965.47 euro for the applicant, raised with 3140.77 per person living on the same address; or receiving a specific reimbursement designated for people who are considered to be in a ‘vulnerable’ position). To illustrate, low income requirements in 2014 were set at maximum 16,743.70 euro in the previous year for the applicant (and 3099.72 per additional person), while an average gross income then amounted 46,197 euro [31,32,33]. To participate, being able to read and understand Dutch was a language requirement, although it was not necessary to be a native speaker. Exclusion criteria were: having a psychiatric and/or neurodegenerative disorders (e.g., Alzheimer’s, Parkinson, ...); (being formally recognized as) having physical, intellectual or sensory impairment(s); or not being able to interact with the researcher. To recruit people eligible for participation, 11 organizations working with people in a vulnerable position were contacted, which is a methodology similar to the ones used in previous research with vulnerable groups [34, 35]. The number of eligible participants was difficult to determine beforehand: recruitment was scheduled on informal gatherings with fluctuating number of people showing up. Saturation in participants’ opinions was pursuit, rather than a predetermined sample size, as a consequence of challenging recruitment.
Data collection
To determine the suitability of HLS-EU-Q16, cognitive interviews about the questionnaire were performed by one researcher using the Verbal Probing technique [36]. The suitability of the questionnaire was operationalized as participants’ opinion about: the length of the questionnaire and questions; comprehension of questions and language; clarity of instructions; the response process; the layout of the questionnaire and any other remarks not directly addressed by the researcher.
Participants randomly received either HLS-EU-Q16 or HLS-EU-Q16-EZ, dividing them in two groups. To avoid stigmatization, everybody who was present at the meeting when the interviews were scheduled to be held, could complete the questionnaires that had been randomly distributed to the group, but only those meeting the inclusion criteria were interviewed directly afterwards. The purpose of the study was explained, participants were assured of the anonymity of the study and of the fact that they would not be judged, which stimulated them to give their honest opinion about the questionnaire. Information was gathered through a semi-structured interview, carried out by the same researcher. Interviews were audio-taped to facilitate analysis afterwards. Interviews were ended because of data saturation.
Cognitive interview
Exemplary probing questions to assess comprehension, were: “What does [term] mean to you?” “Can you explain [question] in your own words?”, “Was that [question] easy or hard to answer?”. When questions or words were unclear, the corresponding question of the other version was presented (Appendix 1). To determine the layout of the questionnaire, participants were asked to choose the most preferred one out of six exemplary layouts (Additional file 1).
Statistical analysis
Out of interest and in order to determine over- or underestimation of health literacy levels, non-responses and health literacy scores were statistically analyzed. HL-scores were calculated by coding responses “very easy” and “easy” as 1; “difficult” and “very difficult” as 0, subsequently summing them, which results in a score between 0 and 16, categorized as inadequate (<9), limited (9–12) or sufficient (13–16) health literacy [7, 23]. Sociodemographic characteristics (gender, age, level of education, income) were determined. Data analysis was performed using SPSS 22.0.
Results
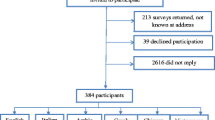
A total of 13 participants from three organizations were included in the study which took place from October 2015 until December 2015. Three respondents eligible for participation did not consent to interviewing and were excluded. Nine people were excluded from the study because they did not meet inclusion criteria. The characteristics of the participants are shown in Table 1. The majority of participants was female. Respondents’ age was on average 59 years old with SD 8.
Informal test on HLS-EU-Q16
To construct a questionnaire on B1-level, at least 12 items would have needed to be revised based on vocabulary and/or sentence structure (Q1, Q4 – Q13, Q16).
Cognitive interview
Difficulties in completing the questionnaires (HLS-EU-Q16 = A; HLS-EU-Q16-EZ = B) as reported by participants in the interviews, are summarized in Table 2. Words that were unclear in A-version were ‘preventive’ (Dutch ‘preventief’) (Q10), ‘mental wellbeing’ (Dutch ‘geestelijk welzijn’) (Q13), ‘to judge’ (Dutch ‘beoordelen’) (Q5 and Q11) and ‘media’ (Q12).
Comprehension
Despite vocabulary and sentence structure being unclear, participants reported difficulties related to their decision processes: being confused about which answer option corresponded to their thoughts on the question. Overall, problems related to comprehension can be categorized as:
-
1° Comprehension problems due to
-
vocabulary and
-
sentence structure
-
-
2° Decision process, often abstraction problems:
-
Referencing to general practitioner
-
Not relating to questions about the media
-
Different interpretations of preventive examinations: confusion if question is restricted to cancer screening
-
Difficulties distinguishing between 'appraising' or 'applying' - questions
-
Unclear distinction between questions
-
-
3° Irrelevance of questions
The least understood in both questionnaires are questions 5, 10 and 11. Questions 1, 3 and 6 were perceived as more comprehensible in the B-version.
Length, response process and layout
All respondents were satisfied with the length of the questionnaires. Few remarks were made with regard to the response process (“Answer options should not be ‘rather’ (Dutch ‘tamelijk’) easy or difficult, but ‘less’ (Dutch: ‘minder’) or ‘not quite’ (Dutch ‘niet zo’)” questionnaire A, respondent 8) and layout (“Important and/or repetitive sentences should be typed bold. I want space to write remarks and there should be more spacing between questions.” q uestionnaire A, respondent 6). With regard to layout, the majority of participants agreed that the questionnaire had to be structured, with borders separating different questions and spacing between them. Important (parts of) sentences, like the repetitive basic question, should be typed in bold. Some participants preferred being able to write down comments supplementary to each question. When presented with 6 exemplary layouts (Additional file 1) two groups of respondents can be distinguished: one that preferred examples 1 and 6, and the other preferring examples 2 and 5. Presumably, the former are similar because of spacing, the latter because of the only difference being the (lack of) boarding. There is a slight preference for empty boxes to check (example 1), instead of a repetition of each answer option (examples 2, 5 and 6). Almost all participants preferred repetitive questions or important parts of the question being typed bold.
Missing responses
Non-responses were analyzed quantitatively. In Table 3 missing responses are illustrated. The sum of non-responses generated in the group completing the HLS-EU-Q16 was higher (n = 17) than the number of total non-responses for those who filled out the HLS-EU-Q16-EZ (n = 10). Incomplete questionnaires were generated by 7 of 13 participants, of which four filled out the HLS-EU-Q16; one participant completed only half of HLS-EU-Q16.
Discussion
When developing questionnaires to measure HL, it is important to consider respondents’ level of education. Therefore, feasibility of a HL-instrument (HLS-EU-Q16) was examined in people with low literacy. The objective was to determine how respondents experienced length, comprehension and layout (overall: ‘suitability’) of this instrument. In this feasibility assessment, a variety of factors (difficulty of a text, layout...) can be addressed. Moreover, this is a subjective approach, as opposed to – in literature sometimes contested – readability tests in which texts are quantitatively assessed [37]. Moreover, interviewing the intended users of the questionnaire is helpful to gather in-depth information [38].
The results of this study indicate that HLS-EU-Q16 is a questionnaire suitable to determine the level of HL in a population of people of low literacy on account of their lower income and education. Overall, the questions of the instrument are well understood. Moreover, cognitive interviews regarding participants’ opinion about the questionnaire revealed that less items of HLS-EU-Q16 were perceived to be difficult or required a revision than suggested by the researcher’s informal test on B1-level for documents. Based on presented findings it can be concluded that changing the vocabulary is insufficient to improve the suitability of HLS-EU-Q16.
Reported difficulties
When referring to the initial framework of HLS-EU questionnaire [3], questions often reported to be less comprehensive were those about ‘disease prevention’ (domain) or ‘appraisal’ of information (competency). Indifferent of domain or competency, all questions referring to a potential role of the media in health care seemed hard to relate to. Referring to one’s general practitioner as a source of health information was an apparent and frequently mentioned response. This statement was most often accompanied by the comment that respondents had difficulties deciding how to respond. Indirectly, these findings revealed the trust in general practitioners and consequently their crucial position in health care, particularly for vulnerable groups (people with low levels of income and education) [39,40,41].
Questions the least understood in both questionnaires resulted in high number of non-responses. Although reliability of HL-scores is irrelevant because of the research design, non-responses illustrated limited comprehension of HLS-EU-Q16. However, respondents reporting incomprehension of this instrument most often answered at least half of the items. Hampered comprehension of questions could be attributed to converging difficulties: vocabulary that was perceived as difficult (‘to judge’ (Dutch ‘beoordelen); ‘media’), abstraction, as well as participants being indecisive on the appropriate response.
Some difficulties persisted even when HSL-EU-Q16-EZ (the modified questionnaire) was presented to participants. Because data collection with HLS-EU-Q16 was not carried out face-to-face, as opposed to HLS-EU-Q47 in which Computer Assisted Personal Interviewing (CAPI) was used, people of low literacy groups could benefit from a minor adjusted HLS-EU-Q16 [21]. To resolve both comprehension and decision process problems, some questions would benefit from an additional explanation. Providing extra information in short, explanatory sentences can bypass problems concerning the meaning of words. Moreover, it may rule out confusion amongst respondents by giving more context and making it easier for people of low literacy groups to respond. The suggestion for contextual information is made based on reports of confounding questions: some questions were perceived as too similar, leaving respondents confused about their objective. To situate questions, providing information with regard to the ‘competencies’ to which questions are referring to (for instance, distinguishing questions about ‘appraising’ from those about ‘applying’) could facilitate interpretation. In conclusion, it is advisable to add information similar to the information that would be provided by the interviewer when collecting data based on CAPI (HLS-EU-Q47). Although occurring rarely, questions can truly be irrelevant because of very specific situations: for instance, someone who needs to rely on health care professionals’ (or informal caregivers’) decision because of their medical condition, might find some questions irrelevant; someone with no or limited access to 'the media'. In these rare cases, people would benefit from an additional category to report accordingly; adversely, it increases the likelihood of non-responses. When the questionnaire would be used with forced answering (electronically), benefits and disadvantages of an extra category should be outweighed.
The following changes might improve the understanding of the questions: basic instructions can allude on how questions should be interpreted, guidance on answering options can be provided in case people would feel to only ‘rely on their general practitioner or other (non-)medically trained people’; questions can be broken down into different components, so it can be avoided that people find the portrayed situation in a part of the question irrelevant to them; the meaning of terminology might be explained through an example, for instance of a preventive examination, or questions might be put into a different, more clarifying order (per domain or competency surveyed) [42]. These suggestions should be implemented cautiously, avoiding narrowing the questionnaire to specific health-related topics. However, some additional information might increase comprehensibility and potentially response rate.
Implications
In this research, the focus was on HLS-EU-Q16 (in Dutch). Because HLS-EU questionnaires are available in different languages, but not all of them were tested on ‘cultural applicability’, it would be helpful to determine feasibility of HLS-EU questionnaire beforehand, preferably by surveying or interviewing the intended users [7, 38, 43]. Evaluating the questionnaire’s suitability and eventually readjusting it, might be particularly useful if questionnaires are intended to be used in a paper-pen version, without assistance from a researcher [44]. Because assessing feasibility is subjective, adjustments made in correspondence with respondents’ feedback are specific for those interviewees and therefore not generalizable.
Strengths and limitations
A strength of this study is the insight that was gained with regard to the cognitive process of respondents when completing HLS-EU-Q16. Moreover, this study was specifically targeting a population considered to be vulnerable because of low levels of education and income. To the best of our knowledge, this was the first study targeting this population to examine feasibility of a questionnaire. Similar studies have been carried out in a peadiatric setting or targeting vulnerable groups, such as refugees. [43, 45]. The research of Wångdahl et al. examining HL in refugees, indicated sufficient language proficiency – preferably respondents’ mother tongue – and modification of questions or answering options to be contributing to questionnaires’ accessibility. In their research, HLS-EU-Q16 (in Swedish) was modified based on data collected through cognitive interviews [43].
The main limitations of this study are related to the vulnerable character of the population. Recruitment was challenging: an unusual, yet inclusive approach was used to reach eligible participants in order to avoid stigmatization. Moreover, reaching people of younger age meeting the education requirement seemed even more challenging, which was to be expected given the compulsory education until the age of 18 years old in Belgium. Despite efforts to reach this population, it still resulted in relatively small sample size, but as testing suitability is a qualitative approach, it is not based on representative samples. Data saturation was reached when 13 participants were interviewed, a sample regarded as sufficient [46].
Although a test-retest design would have allowed to generate interesting data, reproducibility was not feasible. Participants seemed to find it difficult to distinguish between answering the 16 questions and answering on the feasibility of these questions (interviewer’s asking about how the questionnaire was perceived often resulted in respondents reporting about their answers). Asking them to participate in a second, similar survey would probably lead to more confusion.
Interviews were conducted using the Verbal Probing technique: the researcher attempted to minimize the use of ‘leading’-probes to reduce bias. However, as the purpose of this interview was to analyze comprehension of questions, an example or clarifying sentence was provided, with the intent to get insight in the difficulties reported by participants and potential solutions, but never from the start. Ideally, the interview would have been conducted during the completion of the questionnaire. However, the time between completing the questionnaire and the interview was minimalized to 1 h maximum. A final limitation is that this research was carried out with paper-based questionnaires only. The findings presented in this study are not necessarily transferable to the same instrument in a web-based version. Working with digital surveys requires a specific set of skills: these were not taken into account in this research.
Future research
Based on reported difficulties, an altered HLS-EU-Q16 can be developed to determine HL in people with low literacy. Based on the findings of this research, some people with potential limited HL might benefit from some questions being formulated more clearly, for instance by adapting wording or by providing contextual information to facilitate interpretation [42]. Moreover, a complementary, modified questionnaire could be provided or it might be useful to determine HL through interviews as opposed to surveying with pen and paper [47].
Conclusion
Determining HL in people with limited literacy based on HLS-EU-Q16 is feasible. However, to facilitate the use and interpretation, some questions would benefit from minor adjustments: by simplifying wording or providing explanatory, contextual information.
References
Médecins du monde - Doctors of the World in Europe. Access to health care for vulnerable groups in the European Union in 2012. An overview of the condition of persons excluded from healthcare systems in the EU. 2012.
Sørensen K, Peilikan JM, Röthlin F, Ganahl K, Slonska Z, Doyle G, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Pub Health. 2015;25:1053–8.
Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health [Internet]. BioMed Central Ltd; 2012 [cited 2014 Jul 17];12:80. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3292515&tool=pmcentrez&rendertype=abstract.
Institute of Medicine. Health literacy: a prescription to end confusion. Washington DC: National Academies Press; 2004.
Nutbeam D. Advancing health literacy : a global challenge for the 21st century. Health Promot Int. 2000;15:183–4.
Kickbush I. Health literacy: the solid facts. Kickbusch, I. (ed) et al. Health literacy: the solid facts. Copenhagen: World Health Organization (WHO), Regional Office for Europe.; 2013.
Sørensen K, Van den Broucke S, Pelikan JM, Fullam J, Doyle G, Slonska Z, et al. Measuring health literacy in populations: illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health [Internet]. 2013 [cited 2014 May 12];13:948. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4016258&tool=pmcentrez&rendertype=abstract.
Kaufman H, Skipper B, Small L, Terry T, McGrew M. Effect of literacy on breast-feeding outcomes. South Med J. 2001;94:293–6.
Dolan NC, Ferreira MR, Davis TC, Fitzgibbon ML, Rademaker A, Liu D, et al. Colorectal cancer screening knowledge, attitudes, and beliefs among Veterans : does literacy make a Difference ? J Clin Oncol. 2014;22:2617–22.
Lindau ST, Tomori C, Lyons T, Langseth L, Bennett CL, Garcia P. The association of health literacy with cervical cancer prevention knowledge and health behaviors in a multiethnic cohort of women. Am. J. Obstet. Gynecol. [Internet]. 2002 [cited 2014 Aug 27];186:938–43. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0002937802456876.
Scott TL, Gazmararian JA, Williams MV, Baker DW. Health literacy and preventive health care use among Medicare enrollees in a managed care organization. Med Care. 2002;40:395–404.
Health Literacy Tool Shed. A database of health literacy measures. [Internet]. Available from: https://healthliteracy.bu.edu/. Accessed 12 May 2017.
Davis T, Long S, Jackson R, Mayeaux E, George R, Murphy P, et al. Rapid estimate of adult literacy in medicine: a shortened screening instrument. Fam Med. 1993;25:391–5.
Davis TC, Gazmararian J, Kennen EM. Approaches to improving health Literacy : lessons from the field. Joural Heal Commun. 2006;11:551–4.
Weiss BD, Mays MZ, Martz W, Castro KM, DeWalt DA, Pignone MP, et al. Quick assessment of literacy in primary care: the newest vital sign. Ann Fam Med. 2005;3:514–22. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1466931&tool=pmcentrez&rendertype=abstract.
Pander Maat H, Essink-Bot M-L, Leenaars KE, Fransen MP. A short assessment of health literacy (SAHL) in the Netherlands. BMC Public Health. 2014;14:990. Available from: http://www.biomedcentral.com/1471-2458/14/990.
Steckelberg A, Hülfenhaus C, Kasper J, Rost J, Mühlhauser I. How to measure critical health competences : development and validation of the critical health competence test (CHC test). Adv Heal Sci Educ theory Pract. 2009;14:11–22.
Wang J, Thombs BD, Schmid MR. The Swiss Health Literacy Survey: development and psychometric properties of a multidimensional instrument to assess competencies for health. Health Expect. 2014 [cited 2014 Sep 24];17:396–417. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22390287.
Jordan JE, Buchbinder R, Briggs AM, Elsworth GR, Busija L, Batterham R, et al. The health literacy management scale (HeLMS): a measure of an individual’s capacity to seek, understand and use health information within the healthcare setting. Patient Educ. Couns. [Internet]. Elsevier Ireland Ltd; 2013 [cited 2014 Aug 14];91:228–35. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23419326.
Osborne RH, Batterham RW, Elsworth GR, Hawkins M, Buchbinder R. The grounded psychometric development and initial validation of the health literacy questionnaire ( HLQ ). BMC Public Health. 2013;13:658.
Pelikan JM, Röthlin F, Ganahl K. Comparative report of health literacy in eight EU member states. The European health literacy survey HLS-EU. [Internet]. 2012. Available from: http://ec.europa.eu/chafea/documents/news/Comparative_report_on_health_literacy_in_eight_EU_member_states.pdf. Accessed 12 May 2017.
The HLS-EU Consortium 2012. Measurement of health literacy in Europe: HLS-EU-Q47; HLS-EU-Q16; and HLS-EU-Q86. Health Literacy Project 2009–2012 [Internet]. 2012. Available from: http://www.forumitesss.com/wp-content/uploads/2015/02/HLS-EU-Q-tools-and-introduction-2.pdf. Accessed 12 May 2017.
Röthlin F, Pelikan J, Ganahl K. Die Gesundheitskompetenz Jugendlichen in Österreich [Internet]. 2013. Available from: http://lbihpr.lbg.ac.at.w8.netz-werk.com/sites/files/lbihpr/attachments/hljugend_bericht.pdf. Accessed 12 May 2017.
Pelikan JM, Röthlin F, Ganahl K. Measuring comprehensive health literacy in general populations : validation of instrument, indices and scales of the HLS-EU study. 6 th Annu. Heal. Lit. Res. Conf. [Internet]. 2014. p. 54. Available from: http://www.bumc.bu.edu/healthliteracyconference/files/2014/06/Pelikan-et-al-HARC-2014-fin.pdf. Accessed 12 May 2017.
Van den Broucke S, Renwart A. La litteratie en sante en belgique: un mediateur des inegalites sociales et des comportements de sante [Internet]. 2014. Available from: http://alfresco.uclouvain.be/alfresco/service/guest/streamDownload/workspace/SpacesStore/b6374a8a-76d3-44b5-b888-3fc0c0c05fe5/Litt%C3%A9ratie%20en%20sant%C3%A9%20en%20Belgique.pdf?guest=true. Accessed 12 May 2017.
Fransen MP, Leenaars KEF, Rowlands G, Weiss BD, Maat HP, Essink-Bot M-L. International application of health literacy measures: Adaptation and validation of the newest vital sign in The Netherlands. Patient Educ. Couns. [Internet]. Elsevier Ireland Ltd; 2014;97:403–9. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0738399114003668.
Tiller D, Herzog B, Kluttig A, Haerting J. Health literacy in an urban elderly East-German population – results from the population-based CARLA study. BMC Public Health [Internet]. BMC Public Health; 2015;883. Available from: http://dx.doi.org/10.1186/s12889-015-2210-7.
Halbach SM, Enders A, Kowalski C, Pförtner T, Pfaff H, Wesselmann S, et al. Health literacy and fear of cancer progression in elderly women newly diagnosed with breast cancer — A longitudinal analysis. Patient Educ. Couns. [Internet]. Elsevier Ireland Ltd; 2015; Available from: http://dx.doi.org/10.1016/j.pec.2015.12.012.
van der Heide I, Rademakers J, Schipper M, Droomers M, Sørensen K, Uiters E. Health literacy of Dutch adults: a cross sectional survey. BMC Public Health. 2013;13:179. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3599856&tool=pmcentrez&rendertype=abstract.
Bureau Taal. Eenvoudig Nederlands [Internet]. [cited 2015 Dec 1]. Available from: http://www.bureautaal.nl/eenvoudig-nederlands-26.
RijksInstituut Ziekte- en Invaliditeitsverzekering. Grensbedragen inkomsten Verhoogde Tegemoetkoming [Internet]. 2015. Available from: http://www.inami.fgov.be/nl/themas/kost-terugbetaling/financiele-toegankelijkheid/Paginas/verhoogde-tegemoetkoming-grensbedragen-inkomsten.aspx#.VnsX__krLIW. Accessed 12 May 2017.
OECD. Stat OECD [Internet]. Available from: http://stats.oecd.org/viewhtml.aspx?datasetcode=FIXINCLSA&lang=en. Accessed 12 May 2017.
Organization for Economic Co-operation and Development. Annex: taxing wages. Methodology and limitations. 2015.
De Smet A, Poppe A, Hermans K, Willems S, Verlinde E, DeMaeseneer J, et al. KANS: Theoretische achtergronden en onderzoeksopzet. 2011.
Poppe A, De Smet A, Verlinde E, Hermans K, Willems S, Van Audenhove C, et al. KANS Cijferrapport Beschrijvende analyse van de gegevens uit de eerste bevraging. 2012.
Willis GB. Cognitive interviewing: a tool for improving questionnaire design. Thousand Oaks: Sage; 2005.
Doak L, Doak C, Root J. Teaching patients with low literacy skills. Philadelphia: Lippincott Williams & Wilkins; 1996.
Neuhauser L, Paul K. Readability, comprehension and usability. In: Fischhauf B, Brewer N, Downs J, editors. Commun. Risks benefits an evidence-based User’s Guid. Silver Spring: US Department of Health and Human Services; 2011. p. 129–49.
Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83:457–502.
Starfield B. Primary care: an increasingly important contributor to effectiveness, equity, and efficiency of health services. SESPAS report 2012. Gac Sanit. 2012;26:20–6.
Shi L, Starfield B, Politzer R, Regan J. Primary care, self-rated health, and reductions in social disparities in health. Health Serv Res. 2002;37:529–50.
Foddy W. Constructing questions for interviews and questionnaires: Theory and practice in social research. Cambridge: Cambridge university press; 1994.
Wångdahl J, Lytsy P, Mårtensson L, Westerling R. Health literacy among refugees in Sweden - a cross-sectional study. BMC Public Health. 2014;14:1030. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4195944&tool=pmcentrez&rendertype=abstract.
Johnson A, Sandford J. Written and verbal information versus verbal information only for patients being discharged from acute hospital settings to home : systematic review. Health Educ Res. 2005;20:423–9.
Tomlinson D, Isitt JJ, Barron RL, Doyle J, Judd P, Gassas A, et al. Determining the understandability and acceptability of an oral mucositis daily questionnaire. J Pediatr Oncol Nurs. 2008;25:107–11.
Nielsen J. Designing web usability: the practice of simplicity. Indianapolis: New Riders Publishing; 2000.
Meppelink CS, Smit EG, Buurman BM, van Weert JCM. Should we be afraid of simple messages? The effects of text difficulty and illustrations in people with low or high health literacy. Health Commun. 2015;30:1181–9.
Acknowledgements
Not applicable.
Funding
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Authors’ contributions
HS had substantial contributions to conception and design, acquisition of data, analysis and interpretation of data. SVDB had substantial contributions to design and interpretation of data. HS, NC, BA and SVDB drafted and revised manuscript critically for important intellectual content. All authors read and approved the final manuscript. They agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Authors’ information
HS: MSc.; Faculty of Medicine and Life Sciences, Hasselt University, Hasselt, Belgium;
NC: MD, PhD, MBA; Faculty of Medicine and Life Sciences, Hasselt University, Hasselt, Belgium;
BA: MD, PhD; Academic Center for General Practice, KU Leuven – University of Leuven, Leuven, Belgium;
SVDB: PhD; Psychological Sciences Research Institute, Université catholique de Louvain, Louvain-la-Neuve, Belgium.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
All participants were approached for consent to publish anonymized quotes from their interview.
Ethics approval and consent to participate
The study was approved by the ethics committee of Hasselt University. Moreover, a signed informed consent was prerequisite to be eligible for participation.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional files
Additional file 1:
Exemplary layout. (PDF 146 kb).
Appendix 1
Appendix 1
Semi-structured interview
At the start of the interview
People are reassured to give their own opinion and that they will never be judged because there are no correct or false answers.
The interview is audio-taped: recordings will only be used for the purpose of data-analysis. Anonymity is ensured.
Questions
-
1° How did you find the questionnaire ?
-
In your opinion, what was the questionnaire about?
-
What did you think about:
-
◦ the number of questions?
-
◦ the layout of the questionnaire?
-
◦ the introduction at the beginning of the questionnaire
-
-
There is no mentioning on how to mark your answers, what was your opinion on this topic?
-
Which improvements would you suggest?
-
-
2° How did you find the questions ?
-
What was your opinion on the length of the questions?
-
Was it clear to you what every question was on about?
-
◦ When not clear: which question(s) was(were) not clear?
Interviewer provides same question from other version of questionnaire: Is this question [other version of questionnaire] clearer than the original question?
-
-
Can you explain [question] in your own words?
-
-
3° How did you find the vocabulary ?
-
Did you understand all the words used in the questionnaire?
-
Were there any words that were not clear to you?
-
What does the [term] mean to you?
-
-
4° How did you find the answering options ?
-
Was that [question] easy or hard to answer?
-
If the question was clear to you, was it clear to you which answering option corresponded with you answer?
-
In your opinion, was it easy or hard to respond in this manner, with the given answering options?
-
Would you have preferred a mentioning on how answering options should be marked?
-
-
5° Exemplary layouts
The interviewer distributes exemplary layouts and explains the differences between them: Which one of these layouts would you prefer and why?
-
6° Suggestions and other remarks
Do you have any final remarks or suggestions? There might be something that hasn’t been mentioned in the interview and that you would like to add because it is important to you in order to improve the questionnaire?
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Storms, H., Claes, N., Aertgeerts, B. et al. Measuring health literacy among low literate people: an exploratory feasibility study with the HLS-EU questionnaire. BMC Public Health 17, 475 (2017). https://doi.org/10.1186/s12889-017-4391-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-017-4391-8