
Abstract
Background
Spinal epidural hematoma without significant trauma is a rare condition with potentially severe outcome. This case report and systematic review of the literature illustrates the clinical presentation, risk factors, evaluation, treatment and outcomes of spinal epidural hematoma without significant trauma in children.
Case presentation
We report one case of a 7-year-old girl who developed a neck pain after minor cervical sprain. MRI showed a right posterior epidural hematoma extending from C2/3 to T1. The hematoma was surgically evacuated, and the histopathology showed an arteriovenous malformation. Postoperative MRI showed complete evacuation of the hematoma and no residual vascular malformation. We report a second ASE with idiopathic spinal epidural hematoma of a 4½-year-old boy presenting with neck pain. MRI showed a right-sided latero-posterior subacute spinal epidural hematoma at C3–C5. Owing to the absence of any neurological deficit, the patient was treated conservatively. MRI at 3 months showed complete resolution of the hematoma.
Conclusions
Spinal epidural hematoma without significant trauma in children is a rare condition. It may present with unspecific symptoms. Screening for bleeding diathesis is warranted and neuroradiologic follow-up is essential to rule out vascular malformation. Whereas most children have a favorable outcome, some do not recover, and neurological follow-up is required.
Similar content being viewed by others


Background
Spinal epidural hematoma (SEH) without significant trauma is rare in children. In the literature, the term “spontaneous spinal epidural hematoma” was used to describe SEH without clear traumatic etiology. Since this term, however, covers cases of idiopathic SEH, bleeding due to coagulopathy or vascular malformations and hemorrhages after minor trauma, it was recommended to avoid the terminology [1]. In the present article we therefore use the term “SEH without significant trauma”. The condition is mostly observed in adults with a bimodal distribution with peak prevalence in the 2nd and 6th decades of life with an estimated incidence of 0.1 per 100,000 patients per year [1,2,3,4]. A recent review revealed that spinal epidural hematomas occur in all age categories and are by far the most common type of spinal haematoma [3]. Most cases manifest with acute onset pain at the level of the hematoma and sensorimotor deficit with or without bladder and/or intestinal disturbances [3]. Various etiologies, such as coagulation disorders and vascular malformations have been described [3,4,5,6,7,8,9].
The clinical presentation of SEH without significant trauma in children is often nonspecific, including irritability, pain, torticollis, and neurological deficit [10,11,12,13,14,15]. In some cases, minimal cervical trauma precedes SEH [16, 17]. The nonspecific presentation in children may lead to delayed diagnosis and treatment. Early surgical decompression likely leads to good outcomes [18, 19]. Although surgery seems to be preferred to conservative treatment in adults, some factors are important in determining the choice of treatment: preoperative neurological status, coagulopathy and the length of SEH contribute to poor postoperative functional recovery. Literature on SEH without significant trauma in children is scarce [6, 9, 11,12,13, 20,21,22,23,24,25,26,27,28,29,30]. We report on two pediatric cases.
Case presentation
Case 1
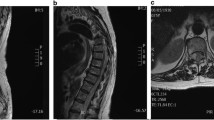
A 7-year-old girl without other health problems presented to the pediatric emergency department with a 10-h history of neck pain following a benign neck flexion-extension movement associated with a cracking noise. The past medical history was unremarkable. There was no a priori history of non-accidental trauma. Clinical examination revealed contractions of the para-spinal cervical muscles with no neurological deficit. Despite oral analgesia, the pain gradually increased. At the child’s second visit, no new clinical abnormalities were noted. Twenty-four hours after presentation, she developed progressive weakness of both arms and legs and paresthesia of the right hand. Bladder or sphincter dysfunction was not reported. Magnetic resonance imaging (MRI) of the spine showed hyper acute right posterior epidural hematoma extending from C2/3 to T1, leading to spinal cord compression (see Fig. 1a-c). The extensive hematologic work-up demonstrated no coagulation abnormalities. She underwent emergency right-sided C4–6 hemi-laminectomy with evacuation of the underlying hematoma. Conventional spinal and cerebral angiography was performed 2 days after evacuation of the hematoma and showed no evidence of a vascular malformation. After evacuation of the hematoma, the patient’s neurological status gradually improved, and no sensorimotor deficit was present 3 weeks postoperatively. Histopathology of the site of operation showed irregularly shaped vessel collections of venous and arterial type consistent with an arteriovenous malformation. Postoperative MRI showed complete evacuation of the hematoma and no residual vascular malformation. At 2-year follow-up, the child was neurologically intact with no clinical signs of spinal instability.

MRI scans of case 1 and case 2. In case 1 (a–c) a hyperacute epidural hemorrhage was revealed (T1w isointense signal (1b) and T2w slightly hyperintense signal (1a)). In case 2 (d–f) a subacute hemorrhage was found (T1w hyperintense (2b), and T2w iso- to slightly hyperintense signal (2a)). Arrows: epidural hemorrhage, arrowheads: spinal cord.
Case 2
A 4½-year-old boy without other health problems was referred to the pediatric emergency department with a 5-day history of progressive neck pain. No history of prior trauma was reported (also not for a non-accidental trauma), and the past medical history was unremarkable. He was discharged home with oral analgesia. Persistent pain, neck stiffness, and torticollis lead to a second visit 5 days later. Physical examination on admission showed an alert child with marked torticollis, pain-induced limitation of neck movements and tenderness on palpation of the neck muscles. Neurological examination was otherwise normal. Emergency computed tomography (CT) and MRI of the spine revealed a right-sided latero-posterior subacute spinal epidural hematoma at C3–C5, exerting a mass effect on the spinal cord (see Fig. 1d-f). No vascular malformation was visible. MRI of the brain was normal. Conventional angiography was not performed. A coagulation profile revealed decreased Von Willebrand factor (VWF) levels with an antigen level of 42% and activity of 29% (normal ranges are above 50%), with an otherwise normal factor VIII level at 85% and a platelet count of 307 G/L. Owing to the absence of any neurological deficit, the patient was treated conservatively with good pain control achieved with paracetamol and morphine. Morphine was stopped after 1 week with no pain recurrence. Neck stiffness improved spontaneously. MRI at 1 week showed a decrease in the size of the hematoma. VWF level improved spontaneously, with no need for substitution. Three weeks after presentation, the child was completely asymptomatic. MRI at 3 months showed complete resolution of the hematoma. The VWF values remained within the normal range (antigen at 74% and activity at 59%). The suspicion of von Willebrand disease could be ruled out.
Discussion and conclusion
SEH without significant trauma in children is rare. Literature on this condition is scarce and restricted to case reports, case series and narrative reviews. In order to describe clinical manifestation, risk factors and etiology, treatment options, and outcomes after SEH without significant trauma in children we present two illustrative cases. In addition, we performed a systematic literature review using PubMed (from 1950), Cochrane Library (from 1994), National Institute for Health and Care Excellence Evidence (NICE evidence: from 1999), and the Excerpta Medica Database (Embase: from 1947). The date of the last search was 24 February 2017. The following search terms were used: “spontaneous spinal epidural hematoma”, “spinal epidural hematoma”, “spontaneous spinal epidural bleeding”, and “spinal epidural bleeding”. Additional publications were identified from reference lists of selected articles. We included original studies, case reports, and case series written in English, German, French, and Spanish. Congress abstracts were not included. Only articles reporting on patients aged younger than 18 years diagnosed with SEH without significant trauma were included. Articles reporting cases of traumatic spinal epidural hematoma were excluded. Extracted data included age, symptoms and clinical findings at presentation, sex, neuroimaging studies, location of SSEH, type and timing of treatment, risk factors and etiology, and neurological findings at clinical follow-up. Furthermore, the neurological findings described at presentation and follow-up were graded using the American Spinal Injury Association (ASIA) Impairment Scale according to the International Standards for Neurological Classification of Spinal Cord Injury [31], which is a 5-level scale for assessing motor impairment in individuals with spinal cord injury.
We identified 153 cases of children with SSEH. The search results, including the stepwise elimination process, are illustrated in Fig. 2. The details of these case reports are available in tabular form as (Additional file 1).

Process for selecting articles for the literature review
Of the 153 cases included in the final selection, 99 were boys (99/149, 66.5%) and 50 were girls (50/149, 33.5%) with a median age of 7 years (IQR [interquartile range] 20–156 months). The male to female ratio was 6.5:3.5. For 4/153 cases (2.6%), sex was not reported. Table 1 summarizes clinical signs and symptoms at presentation (time point when symptoms occurred) and at diagnosis (time point when diagnosis was made), localization, etiology, contributing factors and treatment. The retrospective ASIA impairment score at diagnosis and at last follow-up is shown in Table 2 and in Fig. 3.

American Spinal Injury Association (ASIA) Impairment Scale at diagnosis and at last follow-up. Bar graph demonstrating the relationship of the ASIA Impairment Scale at diagnosis and at follow-up of children with SSEH
SEH without significant trauma in children may manifest with local pain before any progressive neurological deficit due to spinal cord compression is evident. The classical triad is severe localized spinal pain, radicular pain, and sensorimotor deficit. In contrast to adults [4], manifestation of SEH without significant trauma in children is less specific. The present review confirmed that children below 2 years present mainly with irritability (84%). The diagnosis of SEH without significant trauma in children, especially in toddlers, is challenging. Appropriate treatment may be delayed. This can potentially lead to long-term residual neurological deficits. We found a median delay between presentation and diagnosis was 3.7 days, and median delay between presentation and treatment of 5.6 days. We consider that in children presenting with unspecific symptoms, such as irritability and torticollis, clinical awareness and urgent neuroradiologic evaluation with full spine MRI is essential to rule out SEH. Whereas, in the older publications, myelography and CT was the imaging method of choice, a considerable increase of MRI-related diagnosis of SEH without significant trauma over the past 15 years was evident. The review findings suggest that with increasing availability of imaging facilities (CT, MRI), the number of publications on SSEH cases has increased and patients seem to be treated earlier. However, the no conclusion can be drawn regarding time-trends of treatments and prognosis of the condition.
Trivial spine trauma (minimal effort, sports, neck sprain, fall from own height) preceded the SEH in 20% of all cases. In 55% of the children with cervical SEH, minor spinal trauma preceded the bleeding. Vascular malformation (diagnosed by MR-angiography, during operative evacuation of the hematoma or from histopathology) was found as the cause of SEH in 14%. Arteriovenous malformation was the most frequently reported type of vascular malformation. MRI is considered the gold standard for the diagnosis of SEH and the first choice in the diagnostic work-up. As MRI may not always rule out vascular malformations, a conventional spinal angiogram is essential in negative cases. The use of spinal angiograms was only reported in a few instances. Vascular malformations may be underdiagnosed in children with SEH without significant trauma, especially in cases with preceding minor trauma. In our first case, there was no evidence of vascular malformation in MRI and conventional angiography, but histopathological signs of an arteriovenous malformation were found in evacuated material. We assume that the vascular malformation was compacted due to the space occupying effect of the hematoma. Hence, the rupture of a pre-existing arteriovenous malformation triggered by minor trauma is the most likely diagnosis in case 1. Like Sivakumaran, King, Bodi, Chandler and Walsh [32] we recommend performing a conventional spinal angiogram in all patients who have SEH without significant trauma but no evidence of a coagulation disorder. A coagulation disorder was found in 28% of the cases reviewed and hemophilia A was the most frequent abnormality. Although the severity of hemophilia was mostly not specified, we assume that most patients with SEH without significant trauma were diagnosed with mild forms and SEH was the first manifestation of the coagulation disorder. Children with coagulation disorders diagnosed with SEH without significant trauma were younger than those who had SEH without coagulation disorder (54 months [IQR 10–84] vs 96 months [IQR 24–168]). None of the children was reported to be under treatment with platelet aggregation inhibitors or anticoagulants. Whether a combination of bleeding diathesis and vascular pathologies increases the risk for SEH in children remains unknown. Nevertheless, coagulation studies and a thorough neuroradiologic work-up are essential in all children with SEH without significant trauma.
Before surgical decompression, factor replacement is the most important treatment for SEH due to coagulation disorders, depending on the severity of the disorder, to guarantee adequate hemostasis and to prevent hematoma progression and further neurological aggravation. We found that median treatment delay was shorter in patients with coagulation disorder (4 days compared to 10 days). We assume that the clinicians’ alertness to SEH in patients with bleeding diathesis is greater, leading to a prompter diagnosis. In general, SEH represents a surgical emergency. However, case 2 illustrates that not all cases with SEH without significant trauma in children require a surgical approach. In the literature review 36 of 151 patients did not undergo surgery, because of factor replacement for hemophilia (27 cases), rapid resolution of symptoms (4 cases), or no neurological deficit (5 cases). In cases (such as in our case 2) with long hematoma (less compressive) and in stable patients with minimal neurological deficit, or in cases with early resolution of the hematoma, conservative management may be considered [3, 14, 15, 20, 33]. The exact mechanism of blood clot dissolution in case 2 remains unclear. Various mechanisms - such as redistribution of bleeding, or absorption of the clot by proliferation of endothelial cells or dural supportive tissue - may be responsible.
Two percent of the patients with SEH described in the literature died. We found that 65.5% of the surviving patients of children (aged under 18 years) with SEH without significant trauma recovered completely (see Table 2) – in contrast to the lower overall complete resolution rate of 40% previously reported for all age categories (0–90 years) [4]. However, spinal cord compression within the context of SEH may lead to residual neurological deficits with considerable life-long morbidity in children, and even to death. In particular, children with more severe impairment at presentation seem to be more likely to have more severe long-term impairment, including bladder or sphincter dysfunction. Figure 3 shows the relationship between the ASIA impairment scale scores at last follow-up and at diagnosis (see Fig. 3). Long-term neurological follow-up, including bladder-function monitoring and neuroimaging is necessary, even for children who are asymptomatic at hospital discharge.
To conclude, literature regarding SEH without significant trauma in children is scarce and restricted to case reports and case series. There is a lack of higher-level evidence. Children with SEH without significant trauma often present with unspecific symptoms, such as irritability. This may delay diagnosis and timely initiation of treatment, especially in young children and infants. After a trivial cervical trauma and increasing local pain, clinicians can be falsely reassured and diagnose a trivial torticollis, like in our case. Any progressive cervico-thoracic pain, even after trivial traumas, should alert clinicians. The most common contributory factors are bleeding diathesis and vascular malformation. Therefore, coagulation studies are essential in every child with SEH without significant trauma. MRI is the neuroradiologic procedure of choice in these children. However, as MRI may not rule out vascular malformation, conventional angiography should be considered for this purpose.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- ASIA:
-
American Spinal Injury Association
- CT:
-
Computed tomography
- IQR:
-
Interquartile range
- MRI:
-
Magnetic resonance imaging
- SEH:
-
Spinal epidural hematoma
- VWF:
-
Von Willebrand factor
References
Domenicucci M, et al. Spinal epidural hematomas: personal experience and literature review of more than 1000 cases. J Neurosurg Spine. 2017;27(2):198–208.
Groen RJM, August M, van Alphen H. Operative treatment of spontaneous spinal epidural hematomas: A study of the Factors Determining Postoperative Outcome. Neurosurgery. 1996;39(3):494–509.
Groen RJM. Non-operative treatment of spontaneous spinal epidural hematomas: a review of the literature and a comparison with operative cases. Acta Neurochir. 2004;146:103–10.
Kreppel D, Antoniadis G, Seeling W. Spinal hematoma : a literature survey with meta-analysis of 613 patients. Neurosurg Rev. 2003;26:1–49.
Azumagawa K, Yamamoto S, Tanaka K, Sakanaka H, Teraura H, Takahashi K, et al. Non-operative Treated Spontaneous Spinal Epidural Hematoma in a 12-year-old boy. Pediatr Emerg Care. 2012;28(2):167–9.
Cakir E, Karaarslan G, Usul H, Baykal S, Kuzeyli K, Mungan L, et al. Clinical course of spontaneous spinal epidural haematoma mimicking Guillain-Barré syndrome in a child: a case report and literature review. Dev Med Child Neurol. 2004;46:838–42.
Chrétiennot-Bara C, Guët A, Balzamo E, Noseda G, Torchet MF, Rothshild C, et al. Hématome épidural chez l’enfant hémophile: difficultés diagnostiques. Arch Pediatr. 2001;8:828–33.
Dauch WA. Spinale Epidural-hämatome bei Kindern und Jugendlichen. Neurochirurgia. 1986;29:83–9.
Caldarelli M, Di Rocco C, La Marca F. Spontaneous Spinal Epidural Hematoma in Toddlers : Description of Two Cases and Review of the Literature. Surg Neurol. 1994;41:325–9.
Chang CW, Lin LH, Liao HT, Hung KL, Hwan JS. Spontaneous Spinal Epidural Hematoma in a 5-year-old Girl: Case Reports. Acta Paediatr Taiwan. 2002;43(6):345–7.
Patel H, Boaz JC, Phillips JP, Garg BP. Spontaneous Spinal Epidural Hematoma in Children. Pediatr Neurol. 1998;19(4):302–7.
Patel H, Garg BP. Increasing Irritability With Sudden Onset of Flaccid Weakness. Semin Pediatr Neurol. 1996;3(3):192–7.
Khursheed N, Makhdoomi R, Tanki H, Wani A. Spinal Epidural Hematomas in Fast Bowlers: Report of Two Unusual Cases. Pediatr Neurosurg. 2013;49:303–6.
Agha BS, Tehan C, Perno J. Torticollis, Not Always the Usual Suspects. Pediatr Emerg Care. 2011;27(1):32–3.
Jumani DB, Littlewood R, Iyer A, Fellows G, Healy A, Abernethy L, et al. Spontaneous spinal epidural haematoma mimicking meningitis in a 2-year-old child – a case report and literature review. Childs Nerv Syst. 2013;29:1795–8.
Van Heesewijk JPM, Casparie JWBM. Acute spontaneous spinal epidural haematoma in a child : case report. Eur Radiol. 2000;10:1874–6.
Vallee B, Besson G, Gaudin J, Person H, Le Fur JM, Le Guyader J. Spontaneous spinal epidural hematoma in a 22-month-old girl. Case report. J Neurosurg. 1982;56:135–8.
Liao CC, Lee ST, Hsu WC, Chen LR, Lui TN, Lee SH. Experience in the surgical management of spontaneous spinal epidural hematoma. J Neurosurg Spine. 2004;100(1):38–45.
Liao CC, Hsieh PC, Lin TK, Lin CL, Lo YL, Lee SC. Surgical treatment of spontaneous spinal epidural hematoma: a 5-year experience. J Neurosurg Spine. 2009;11:480–6.
Soundappan SVS, Darwish B, Chaseling R. Traumatic Spinal Epidural Hematoma-Unusual Cause of Torticollis in a Child. Pediatr Emerg Care. 2005;21(12):847–9.
Schoonjans AN, De Dooy J, Kenis S, Menovsky T, Verhulst S, Hellinckx J, et al. Spontaneous spinal epidural hematoma in infancy : Review of the literature and the seventh case report. Eur J Paediatr Neurol. 2013;17:537–42.
Lim JJ, Yoon SH, Cho KH, Kim SH. Spontaneous Spinal Epidural Hematoma in an Infant : A Case Report and Review of the Literature. J Korean Neurosurg. 2008;44:84–7.
Jackson FE. Spontaneous Spinal Epidural Hematoma Coincident with Whooping Cough. Case report Journal Neurosurgery. 1963;20:715–7.
Jackson R. Case of spinal apoplexy. Lancet. 1869;3:5–6.
Poonai N, Rieder MJ, Ranger A. Spontaneous Spinal Epidural Hematoma in an 11-Month-Old Girl. Pediatr Neurosurg. 2007;43:121–4.
Min S, Duan Y, Zhang L. Chronic spontaneous cervicothoracic epidural hematoma in a 8-month-old infant. Ann Saudi Med. 2011;31(3):301–4.
Arya R, Jain P, Kumar A, Gulati S. Spontaneous Spinal Epidural Hematoma in an Infant. J Child Neurol. 2012;27(12):1577–9.
Mayer JA. Extradural Spinal Hemorrhage. Case Report. Can Med Assoc J. 1963;89:1034–7.
Lepintre J, Despres P. Rendu, Seringe P. Hématome intra-rachidien extra-dural de siège cervical. Ann Pédiatr. 1969;16:723–7.
Tewari MK, Tripathi LN, Mathuriya SN, Khandelwal N, Kak VK. Spontaneous spinal extradural hematoma in children: Report of three cases and review of the literature. Childs Nerv Syst. 1992;8:53–5.
Kirshblum SC, Waring W, Biering-Sorensen F, Burns SP, Johansen M, Schmidt-Read M, et al. Reference for the 2011 revision of the international standards for neurological classification of spinal cord injury. Acad Spinal Cord Inj Professionals. 2011;34(6):547–54.
Sivakumaran R, King A, Bodi I, Chandler CL, Walsh DC. Spontaneous epidural spinal haematoma in children caused by vascular malformations. Eur Spine J. 2016;25:614–8.
Rajz G, Cohen JE, Harnof S, Knoller N, Goren O, Shoshan Y, et al. Spontaneous spinal epidural hematoma: The importance of preoperative neurological status and rapid intervention. J Clin Neurosci. 2015;22:123–8.
Acknowledgments
We would like to thank Dr. Mahmoud Messerer for his scientific input and Susan Kaplan for the language editing.
Funding
No funding for the article.
Author information
Authors and Affiliations
Contributions
ACL, BL and SG contributed to the drafting of the manuscript, acquisition of data and analyzing of the data. ACL contributed to performing the database searching and evaluation of the included articles. ACL, BL and SG contributed to the drafting of the manuscript, acquisition of data and analyzing of the data. MR contributed to the drafting of the manuscript. MR, MS, CTU, RM, RKV contributed to designing of the study, interpretation the data and final approval of the version to be published. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the parents of both patients for publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Alphabetical list of authors of articles included in the review and summary of study design and findings.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Carlhan-Ledermann, A., Laubscher, B., Steinlin, M. et al. Spinal epidural hematoma without significant trauma in children: two case reports and review of the literature. BMC Pediatr 20, 77 (2020). https://doi.org/10.1186/s12887-020-1957-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-020-1957-x