
Abstract
Background
Preventive quality measures for the foster care population are largely untested.
The objective of the study is to identify healthcare quality measures for young children and adolescents in foster care and to test whether the data required to calculate these measures can be feasibly extracted and interpreted within an electronic health records or within the Statewide Automated Child Welfare Information System.
Methods
The AAP Recommendations for Preventive Pediatric Health Care served as the guideline for determining quality measures. Quality measures related to well child visits, developmental screenings, immunizations, trauma-related care, BMI measurements, sexually transmitted infections and depression were defined. Retrospective chart reviews were performed on a cohort of children in foster care from a single large pediatric institution and related county. Data available in the Ohio Statewide Automated Child Welfare Information System was compared to the same population studied in the electronic health record review. Quality measures were calculated as observed (received) to expected (recommended) ratios (O/E ratios) to describe the actual quantity of recommended health care that was received by individual children.
Results
Electronic health records and the Statewide Automated Child Welfare Information System data frequently lacked important information on foster care youth essential for calculating the measures. Although electronic health records were rich in encounter specific clinical data, they often lacked custodial information such as the dates of entry into and exit from foster care. In contrast, Statewide Automated Child Welfare Information System included robust data on custodial arrangements, but lacked detailed medical information. Despite these limitations, several quality measures were devised that attempted to accommodate these limitations.
Conclusions
In this feasibility testing, neither the electronic health records at a single institution nor the county level Statewide Automated Child Welfare Information System was able to independently serve as a reliable source of data for health care quality measures for foster care youth. However, the ability to leverage both sources by matching them at an individual level may provide the complement of data necessary to assess the quality of healthcare.
Similar content being viewed by others


Background
Demands for information on the quality of pediatric preventive care have spurred investment in the development of quality measures designed to access the current state of children’s health care and ultimately define areas for improvement [1]. Specific quality measures for the foster care population, though, are largely untested [2, 3], even though youth entering foster care have greater physical, developmental, and mental health needs than their peers in the general population [4, 5]. Although children in foster care are known to have higher rates of social and medical morbidity, guidelines for the care of foster children are rarely adhered to in routine practice and may be difficult to measure [6,7,8,9,10]. One of the most important ways to improve care and reduce poor long term health outcomes is through the development and testing of reliable quality measures for these high risk youth. To date, measurement has largely been dependent on labor-intensive chart reviews. Two other possible sources of quality data that might be extracted electronically exist for foster care children [11]. A clinical electronic health record (EHR) has potential to provide comprehensive and detailed patient-level data with electronic extraction on a large population. In addition, the Statewide Automated Child Welfare Information System (SACWIS) is a database used by protective services agencies to hold the official case records of children in care. Many states hold health data in their SACWIS records.
In order for these datasets to be useful, each of them would have to contain sufficient detail on health services to compare them against recommended guidelines, entry and exit dates for foster care to calculate eligibility, and demographic data for stratification. The primary objectives of this study were to identify quality measures, such as the appropriate number of well care visits, vaccinations and developmental screening for young children (ages 0–3) and adolescents (ages 12–18) in foster care and test whether the data required to calculate these measures can be feasibly interpreted within an EHR or within SACWIS. These two age groups were chosen because of the diversity of well care measures available for testing in both groups.
Methods
This work was performed as part of the Children’s Health Insurance Program Reauthorization Act (CHIPRA) Pediatric Quality Measures Program (PQMP), specifically as part of the National Collaborative for Innovation in Quality Measurement (NCINQ). Our approach considered three time periods of child welfare engagement: (1) entry into foster care, (2) ongoing foster care, and (3) foster home change or exit. [12,13,14,15,16,17,18,19,20,21,22,23,24] We gathered input from a national advisory panel representing foster care alumni, national policy makers, state child welfare and Medicaid officials, health plan staff, and academic researchers.
Retrospective chart reviews were performed at Nationwide Children’s Hospital (NCH). For the study of children aged 0 to 3 years, we abstracted data from the time period of January 1, 2007- February 28, 2013 from children who met inclusion criteria: 1) In foster care (not including kinship care) within Franklin County, Ohio, and 2) at least one comprehensive well-care visit at a primary care physician (PCP) clinic or foster care specialty clinic at NCH. For the study of children aged 12–18 years, we abstracted data from the time period of January 1, 2009- October 31, 2013 with the same criteria. All extracted data was for care that occurred while the child was in foster care. We defined foster care as full-time care provided by an approved foster care family or group home and excluded any care provided by kin or close family friends (Table 1).
Chart reviews were performed by two staff members familiar with EHR data abstraction (Epic Systems Corporation, Wisconsin). An instruction document outlining the data elements and their common locations was created and used by both reviewers. Inter-rater reliability analyses were performed on the first 41 reviewed records of children within each age group to ensure reproducibility between data abstractors with excellent reproducibility [25, 26]. Study data were managed using REDCap data tool [27]. This study was approved by the NCH Institutional Review Board.
Because exact entry and exit dates for out of home care were often missing from EHRs, entry and exit dates were calculated in three different ways depending on the availability of data: 1) exact entry or exit dates were recorded whenever available, 2) the midpoint of an available date range (dates between health care visits wherein a child was documented to have entered/exited foster care) was used for entry or exit dates, and finally 3) the first well-care visit (or other documented healthcare encounter for adolescents) after entry was considered the entry date and the last well-care visit (or other documented healthcare encounter for adolescents) was considered the exit date when an exact date or date range was unavailable.
SACWIS is a “comprehensive automated case management tool that supports foster care and adoptions assistance case management practice.” [28] This system is intended to hold the official case record of all children currently or previously in out-of-home care in a state. Not all states use SACWIS, and there is substantial heterogeneity across states in the contents of SACWIS [28]. This study used data available in the Franklin County, Ohio SACWIS system in order to reflect the same population studied in the EHR review. A data extract from SACWIS was sent to the investigators containing the records of all children who were in custody during the study period and met inclusion criteria. Inclusion criteria were identical to those used for the EHR review, with the one exception that documentation of a well-care visit was not required. To determine whether data from the EHR and SACWIS could be reliably combined for analyses, we performed matching, using social security numbers when these were available in both the EHR and in SACWIS. As social security numbers were unavailable in one or both databases for approximately 70% of patients, when this number was unavailable we also considered records to be from the same child if they matched on all four of the following criteria: last name, first name, date of birth, and gender. A last name in the EHR was considered to match a last name in SACWIS if the first four characters were identical. Both the primary name and alias listed in SACWIS were considered. A first name in the EHR was considered to match a first name in SACWIS if the first four characters, either with or without symbols, were identical. Again, both the primary name and alias listed in SACWIS were considered.
Continuous variables were described with medians and interquartile ranges (IQR) as none were normally distributed. Categorical variables were described using frequencies and percentages. Quality measures were calculated in either the entire young child or the entire adolescent study cohort. We chose to review a sample of 400 EHRs for both the young child and adolescent EHR studies. The medical record numbers of all included children were sorted randomly such that the children whose charts were reviewed were a random sample of all children who could have been included.
In order to provide the most flexible information on the feasibility of obtaining the proposed quality measures from our data sources, two methods were used to calculate the proposed quality measures: proportions and observed-to-expected ratios. Most quality measures of pediatric healthcare focus on the former. Unfortunately, calculations of such often require steady denominators with fixed lengths of follow-up such as the number of children screened over the number of children eligible who were tracked for a full year. Because foster children cycle in and out of care, the denominator calculations may be ineffective in describing this unstable population.
Several quality measures were calculated as observed (received) to expected (recommended) ratios (O/E ratios) to better describe the actual quantity of recommended health care that was received by individual children, whereas the proportion measures indicate the percentage of children in the study cohort that received all recommended care. Weighted mean O/E ratios were calculated wherein each child’s individual O/E ratio was weighted by his or her total time spent in foster care during the study period. This weighting was performed because it enabled children who spent more time in foster care to contribute more to the calculated O/E measures. We used the AAP Recommendations for Preventive Pediatric Health Care as the guideline for determining the expected, or recommended, number of well-care visits and developmental screenings in the young children and the recommended number of well-care visits, BMI measurements, drug use assessments, alcohol use assessments, sexually transmitted infection screenings, and depression screenings in the adolescents [24]. For each measure, an individual O/E ratio was calculated for each child and then a weighted average of these individual O/E ratios was calculated to provide an appropriate average O/E for the entire cohort.
Continuous variables were described with medians and interquartile ranges (IQR). Categorical variables were described using frequencies and percentages. We also attempted to extract data on the same types of health care encounters that were examined in the chart reviews. SAS version 9.3 (SAS Institute Inc., NC) was used to analyze all data.
Results
Study of EHR data of children age 0–3 years
A total of 400 charts were reviewed. Twenty-five children were excluded from analyses because they did not meet inclusion criteria; 8 were without any well-care visits and 17 entered foster care prior to January 1, 2007. This left 375 patients to be included in analyses (Table 2). Overall, the median duration of time spent in foster care during the study period of 9.2 months (IQR 3.0–17.9) (Table 2). Around 76% of children had exact dates of entry but only 44.8% of children had both exact entry and exact exit dates recorded in their EHR. A quarter of the study population lacked documentation in their EHR of the reason for their first entry into foster care.
Table 3 illustrates the performance of the proposed health care quality measures for young children within our EHR. Among 341 children in the study cohort with an exact date or date range of initial entry into foster care, we observed that 78.6% received a well-care visit within 30 days of entry. Over 79% of all children included in this study received the appropriate number of lead screenings, and 100% with traumatic brain injury (TBI) had a developmental screening within 3 months of their diagnosis. More than half of all children in foster care received the appropriate number of well-care visits (59.2%) and developmental screenings (57.9%) during foster care, and 83% received all of the recommended diphtheria, tetanus, pertussis vaccine (TDap), inactivated poliomyelitis (IPV), Haemophilus Influenzae Type b (HiB), and hepatitis b (HepB) vaccinations by age 1. Over 70% of children received the appropriate number of recommended vaccinations by age 2. Only about 1 in 5 children suspected of physical abuse received a follow-up skeletal survey after one was initially performed, and only 3.2% of transitions from foster home to foster home showed any evidence of a care coordination letter. Data from children who had exact dates of entry and exit revealed similar results for all quality measures (data not shown).
O/E ratios were calculated for the well-child visit and developmental screening measures (Table 3). On average, children received 90% of their recommended well care visits while in foster care and 94% of their recommended developmental screenings while in foster care. These O/E measures, for the reasons already discussed, are higher than their analogous proportion measures.
SACWIS data of children age 0–3 years
A total of 1887 children age 0–3 years with records in SACWIS met our inclusion criteria. (Table 2) Demographic, entry and exit characteristics were similar between the EHR and SACWIS study cohorts, but one key difference between data sources is the consistent documentation of entry and exit dates in SACWIS (100% in SACWIS vs. 44.8% in the EHRs). In addition, SACWIS contains a greater amount of detail regarding foster care history compared to data from the EHR. Unfortunately, SACWIS contains far less detail on the health care provided to children in foster care than EHRs. After reviewing the SACWIS records of a matched sample of the EHR study cohort, it was found that SACWIS was not a viable resource for medical data (data not shown).In addition, only approximately 50% (198/375) of patients with EHR data could be matched across the two data sources.
EHR data of adolescents
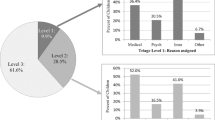
A total of 401 charts were reviewed. Two were excluded because they did not have any well-care visits while in foster care during the study period. This left 399 patients. Table 4 depicts the demographic and entry and exit related characteristics of both the EHR and SACWIS study populations. Overall, the median duration of time spent in foster care during the study period was 10.1 months (IQR 2.5–21.0) (Table 4). Almost 75% of children had exact dates of entry but only 21.8% of children had both exact entry and exact exit dates recorded in their EHR. The most frequently cited reason for first entry into foster care was a child’s behavior problem (30.3%). However, almost 40% lacked documentation in their EHR of the reason for their first entry into foster care.
Table 5 illustrates the performance of the proposed adolescent health care quality measures within our EHR. More than 3/4ths received the appropriate number of annual well-care visits and recommended TdaP and Meningococcal vaccinations. However, less than 1 in 10 girls had documentation in their EHR of having received a full 3-dose course of the human papillomavirus (HPV) vaccine. Over 90% of adolescents had documentation of an annual BMI. Over 75% had documentation of annual drug use assessments, but only 33.8% had documentation of annual alcohol use assessments. Less than half of adolescents were screened annually for both chlamydia and gonorrhea, and less than 25% were screened annually for depression.
O/E ratios were calculated for all of the same events for which proportion measures were calculated, with the exception of the immunization measures (Table 5). On average, adolescents received 96% of their recommended well care visits while in foster care. On average, they received 89% of the recommended number of drug use assessments for the time they spent in foster care, but the rates of screening for alcohol use, sexually transmitted infections, and depression were considerably lower.
SACWIS data of adolescents
A total of 3674 adolescents aged 12–18 years with records in SACWIS met our inclusion criteria (Table 4). Demographic, entry and exit characteristics were similar between the EHR and SACWIS study cohorts, though the proportion of adolescents with undocumented reasons for entry into and exit from foster care in their EHR makes it challenging to compare these characteristics between cohorts. SACWIS contains minimal detail on the health care provided to children in foster care when compared to EHRs.
Discussion
Documentation of data important to the tracking and optimization of the health care of children and adolescents in foster care is frequently incomplete and difficult to find in either EHRs or SACWIS in our patient population. However, despite their limitations, EHRs and SACWIS can be useful data sources for the calculation of some important measures of quality of care in the foster care population, and would be even more useful if certain important data elements were more consistently available and easily extractable from each database. Alternatively, individual level matching across platforms may allow for the optimal methods by which to assess these measures.
Manual review to calculate our proposed foster care quality measures was laborious. The majority of information was located in free text fields and scanned documents rather than structured fields. Many important data elements, specifically the reasons for initial entry into foster case and the entry and exit dates from foster care, were often missing, and this lack of documentation proved to be limiting factors in data abstraction. The accuracy of nearly all of our proposed health care quality measures is contingent upon this critical information. Similar issues were identified for SACWIS data. While demographics and entry and exit characteristics were found in discrete fields, all other information of interest to this study was located in free text fields. This required study investigators to visually examine text notes. Even after this task was performed, it was found that the quantity of information and detail on medical care in SACWIS was far less than from the EHRs.
Identifying the best method to calculate the proposed quality measures revealed the complexity of EHR data abstraction and quality measure development for children in foster care. For example, the Healthcare Effectiveness Data and Information Set (HEDIS) Well-Child Visit measure at 15 months of age would have minimal utility in the foster care population as it requires continuous enrollment for 12 months prior to age 15 months as an inclusion criteria [29]. The O/E ratios examined in this study seemed to be a viable option for the calculation of quality of care measures in the foster care population, primarily because every child can be included in the calculation of these measures regardless of their length of stay or number of episodes in foster care. In addition, children who spend more time in foster care appropriately contribute more to these measures than children who spend less time in foster care. The results in Tables 3 and 5 indicate that select quality measures appear better when calculated using O/E ratios rather than proportions, namely because all health care events contribute to the O/E measures whereas with the proportion measures, a child is counted in the numerator only if the ideal number of events of interest occurred. Admittedly however, the greater mathematical complexity of the weighted average O/E measures, compared to simple proportions, may limit their widespread use.
Considering the challenges we encountered in this study, modification of current EHRs, the use of another data source, or combination of data sources may improve the feasibility of foster care quality measures. An ideal EHR format specific to children was recently proposed [30]. The format provides specific elements and requirements that could be added to current EHRs to enhance the care of children, especially those enrolled in Medicaid and in the care of child welfare [30]. These recommendations include system capacity to store and display 1) whether the child has ever been in out-of home care 2) information about the dates of the out-of-home care and 3) information on the child’s history of abuse or neglect. In addition, the SACWIS data system used by child welfare agencies could also be useful. Although its current use varies by state, it is intended to be a comprehensive database that supports the efforts of case workers to assist children in out of home care [28]. The availability of exact dates of entry into foster care and exit from foster care in SACWIS and the availability of accurate data on health care received in the EHR could, together in a combined database, enable the calculation of more accurate health care quality measures than those presented here. However, a higher match rate than we found would be necessary to make such a combined database useful.
Conclusion
Extraction of data to test foster care quality measures is not currently feasible in a single institution EHR, even though we conducted this study at a large, free-standing children’s hospital with a longstanding commitment to electronic health records, nor is it feasible in a metropolitan county’s SACWIS data. Most proposed quality measures tested did not achieve high adherence as recommended by current guidelines, but it is difficult to tell to what extent missing data elements such as entry and exit dates contributed to these results. Because the quality of information is important to improve patient care, testing foster care quality measures in SACWIS or an augmented EHR that utilizes the children’s EHR format may be a better alternative, and subsequently may yield more reliable results [31].
Abbreviations
- BMI:
-
Body mass index
- CHIPRA:
-
Children’s Health Insurance Program Reauthorization Act
- EHR:
-
Electronic health record
- HEDIS:
-
Healthcare effectiveness data and information set
- HepB:
-
Hepatitis b vaccine
- HiB:
-
Haemophilus Influenzae Type b vaccine
- HPV:
-
Human papillomavirus
- IPV:
-
Inactivated Poliomyelitis vaccine
- IQR:
-
Interquartile ranges
- NCH:
-
Nationwide Children’s Hospital
- NCINQ:
-
National Collaborative for Innovation in Quality Measurement
- O/E ratios:
-
Observed to expected ratios
- PCP:
-
Primary care physician
- PQMP:
-
Pediatric Quality Measures Program
- SACWIS:
-
Statewide Automated Child Welfare Information System
- TBI:
-
Traumatic brain injury
- TdaP:
-
Tetanus,Diphtheria, Pertussis vaccine
References
Mangione-Smith R, McGlynn EA. Assessing the quality of healthcare provided to children. Health Serv Res. 1998;33(4 Pt 2):1059–90.
Beal AC, Co JP, Dougherty D, et al. Quality measures for children's health care. Pediatrics. 2004;113(1 Pt 2):199–209.
Centers for Medicare and Medicaid. Children's Health Insurance Program Reauthorization Act (CHIPRA). Childrens Health Insurance Program CHIP https://www.medicaid.gov/medicaid/quality-of-care/performance-measurement/child-core-set/index.html. Accessed 4 Jan 2013.
Chernoff R, Combs-Orme T, Risley-Curtiss C, Heisler A. Assessing the health status of children entering foster care. Pediatrics. 1994;93(4):594–601.
Steele JS, Buchi KF. Medical and mental health of children entering the utah foster care system. Pediatrics. 2008;122(3):e703–9.
U.S. Government Accountability Office. Foster Care: Health needs of many young children are unknown and unmet. 1995; http://www.gao.gov/products/HEHS-95-114. Accessed 3 Jan 2013.
Ritchie B. "Children's use of health care services while in Foster Care: common themes" memorandum to Susan Orr, associate commissioner for the Children's Bureau, Administration for Childen and Families, and Dennis G. Smith, director of Centers for Medicare and Medicaid Services. OEI-07-00-00645 ed. Washington, DC: U.S. Department of Health and Human Services, Office of the Inspector General; 2005.
Levinson DR. Most Medicaid children in nine states are not receiving all required preventive screening services. OEI-05-08-00520 ed. Washington, DC: U.S. Department of Health and Human Services, Office of Inspector General; 2010.
Leslie LK, Hurlburt MS, Landsverk J, Rolls JA, Wood PA, Kelleher KJ. Comprehensive assessments for children entering foster care: a national perspective. Pediatrics. 2003;112(1 Pt 1):134–42.
Hakim RB, Bye BV. Effectiveness of compliance with pediatric preventive care guidelines among Medicaid beneficiaries. Pediatrics. 2001;108(1):90–7.
Lewandowski RE, Acri MC, Hoagwood KE, et al. Evidence for the Management of Adolescent Depression. Pediatrics. 2013;132(4):e996–e1009.
American Academy of Child and Adolescent Psychiatry, Child Welfare League of America. AACAP/CWLA Policy Statement on Mental Health and Use of Alcohol and Other Drugs, Screening and Assessment of Children in Foster Care. 2003; http://www.aacap.org/. Accessed 18 Dec 2012.
National Collaborating Centre for Acute Care. Head injury. Triage, assessment, investigation and early Management of Head Injury in infants, children and adults. London, UK: National Institute for Health and Clinical Excellence (NICE); 2007. p. 54.
Pringsheim T, Panagiotopoulos C, Davidson J, Ho J. Evidence-based recommendations for monitoring safety of second generation antipsychotics in children and youth. J Can Acad Child Adolesc Psychiatry. 2011;20(3):218.
American Academy of Child and Adolescent Psychiatry. Practice parameter on the use of psychotropic medication in children and adolescents. J Am Acad Child Adolesc Psychiatry. 2009;48(9):961–73.
American Academy of Child and Adolescent Psychiatry. Practice parameter for the assessment and treatment of children and adolescents with schizophrenia. American Academy of Child and Adolescent Psychiatry. J Am Acad Child Adolesc Psychiatry. 2001;40(7 Suppl):4S–23S.
American Academy of Pediatrics Committee on Early Childhood and Adoption and Dependent Care. Developmental issues for young children in foster care. Pediatrics. 2000;106(5):1145–50.
Section on Radiology, American Academy of Pediatrics. Diagnostic imaging of child abuse. Pediatrics. 2009;123(5):1430–5.
Lahoti SL, McClain N, Girardet R, McNeese M, Cheung K. Evaluating the child for sexual abuse. Am Fam Physician. 2001;63(5):883–92.
Jenny C, Crawford-Jakubiak JE, Committee on Child Abuse and Neglect. The evaluation of children in the primary care setting when sexual abuse is suspected. Pediatrics. 2013;132(2):e558–67.
Kellogg ND, American Academy of Pediatrics Committee on Child Abuse and Neglect. Evaluation of suspected child physical abuse. Pediatrics. 2007;119(6):1232–41.
Kellogg N, American Academy of Pediatrics Committee on Child A, Neglect. The evaluation of sexual abuse in children. Pediatrics. 2005;116(2):506–12.
Committee on Early Childhood, Adoption, and Dependent Care. Health Care of Young Children in Foster Care. Pediatrics. 2002;109(3):536–41.
Committee on Practice Ambulatory Medicine, Bright Futures Steering Committee. Recommendations for preventive pediatric health care. Pediatrics. 2007;120(6):1376.
Fleiss JL. Design and analysis of clinical experiments, vol. 73. New York, NY: Wiley.com; 1999.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–74.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
National Resource Center for Child Welfare Data and Technology, Children’s Bureau. About Statewide Automated Child Welfare Information Systems (SACWIS). 2013. https://www.acf.hhs.gov/cb/research-data-technology/state-tribal-info-systems/managers. Accessed 21 Jan 2013.
National Committee for Quality Assurance. HEDIS 2013 volume 2: technical specifications for health plans, vol. 2012. Washington, DC: NCQA. p. 279–81.
Agency for Healthcare Research and Quality. Children's Electronic Health Record Format. United States Health Information Knowledgebase 2013; https://ushik.ahrq.gov/mdr/portals/cehrf?system=cehrf&enableAsynchronousLoading=true. Accessed 13 Jan 2014.
Hayrinen K, Saranto K, Nykanen P. Definition, structure, content, use and impacts of electronic health records: a review of the research literature. Int J Med Inform. 2008;77(5):291–304.
Centers for Disease Control and Prevention. Immunization Schedules. 2013; http://www.cdc.gov/vaccines/schedules/index.html?s_cid=ostltsdyk_govd_406. Accessed 12 Feb 2013.
Ohio Department of Medicaid. Guidelines for Medicaid Lead Testing. Lead Poisoning Prevention and Testing Information for Providers http://medicaid.ohio.gov/FOROHIOANS/Programs/Lead/ProviderLead.aspx. Accessed 15 Jan 2014.
Acknowledgements
We acknowledge Mr. Don Peasley, Director of Evaluation at Franklin County Children Services, who provided us with SACWIS data and whose knowledge of SACWIS informed our interpretation and analysis of the data.
Funding
This project was supported by grant number U18HS020503 from the Agency for Healthcare Research and Quality (AHRQ) and Centers for Medicare & Medicaid Services and, by Award Number Grant UL1TR001070 from the National Center For Advancing Translational Sciences.
The funding sources had no role in the design and conduct of this study; collection, management, analysis and interpretation of the data; preparation, review, or approval of the manuscript; or in the decision to submit the manuscript for publication.
Availability of data and materials
Due to the nature of the records and PHI, the data cannot be made available for public use.
Disclaimer
The content is the responsibility of the authors and does not necessarily represent the official views of AHRQ or of the National Center for Advancing Translational Sciences or the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
KD - participated in study design and coordination, helped to draft and revise the manuscript. PM - participated in study design and coordination, helped to revise the manuscript. KN – Acquisition of data, helped to draft and revise the manuscript. KL – Database design, acquisition of data, and revised manuscript. JC – Analysis and interpretation of data, helped to draft and revise the manuscript. SS - conceived of the study, and participated in its design, helped to draft and revise the manuscript. KK - conceived of the study, and participated in its design, helped to draft and revise the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved, with a waiver of informed consent, by the Nationwide Children’s Hospital Institutional Review Board (IRB) under the following submissions:
IRB13–00106 Feasibility Testing in EHR for Children in Foster Care.
IRB13–00564 Quality Measures for Adolescents in Foster Care.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Deans, K.J., Minneci, P.C., Nacion, K.M. et al. Health care quality measures for children and adolescents in Foster Care: feasibility testing in electronic records. BMC Pediatr 18, 79 (2018). https://doi.org/10.1186/s12887-018-1064-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-018-1064-4