
Abstract
Background
A new staging system recently proposed by the IGCA has demonstrated a better capacity of stratifying different prognoses for gastric cancer than the 7th edition AJCC staging system (AJCC7). The aim of this study was to evaluate the efficacy of the IGCA system in Chinese patients.
Methods
Medical records of patients with gastric cancer who received curative surgery in our center from January 2003 to December 2011 were reviewed retrospectively. All the lesions were staged according to both AJCC7 and IGCA staging systems. Overall survival (OS) of the patients was used as the observation endpoint.
Results
One thousand five hundred twenty-six cases were included in this study. By comparing the AJCC7 system with the IGCA systems, 395 cases were stratified into different stages, most of which were in stage III. The IGCA system could better stratify stage IIIB and IIIC patients (5-year OS, 38.1% vs. 29.0%; P = 0.005) than the AJCC7 system (5-year OS, 38.2% vs. 35.9%; P = 0.148). T3N3bM0, T4aN2M0 and T4aN3bM0 made up 97.5% (385/395) of the stage shift. T3N3bM0, which was stratified to stage IIIB in the AJCC7 system, showed a significant poorer prognosis than T4aN2M0 and T4aN3aM0, which were staged to IIIB and IIIC in the same system. The improper staging was revised in the IGCA staging system.
Conclusions
The IGCA staging system can stratify stage III gastric cancer patients more properly than the AJCC7 system.
Similar content being viewed by others

Background
Gastric cancer is the fourth most common cancer and the second leading cause of cancer-related death [1, 2]. Lymph node (LN) metastasis is the most common metastatic pattern and the most important factor that impacts the prognosis of gastric cancer. However, there is no real consensus over the definition of LN staging. The Japanese Classification of Gastric Carcinoma (JCGC) used to assess the metastatic status of LN according to the anatomical distribution and this classification was widely applied in China because it could properly depict the extent of lymph node removal of surgery. However, many studies argued that the numeric LN staging system proposed by the American Joint Committee on Cancer (AJCC) TNM staging system was simpler and more practical which demonstrated a better prognostic prediction than the anatomical LN staging pattern [3].
The latest edition of the AJCC is the seventh edition (AJCC7) published in 2010, which can more precisely predict the prognosis of gastric cancer after curative surgery by revising the cutoffs of metastatic lymph node counts in the previous edition [4, 5]. In this edition, previous N1 stage (metastasis in 1-6 regional LN) is divided into N1 (metastasis in 1-2 regional lymph nodes) and N2 (metastasis in 3-6 regional lymph nodes). Besides, N3 stage is sub-grouped to N3a (metastasis in 7-15 regional LN) and N3b (metastasis in more than 15 regional LN). According to the existing literature [6, 7], a much better prognosis was observed in patients with N3a stage than those with N3b. However, the AJCC7 gastric staging system fails to incorporate N3a and N3b into any stage group, which would impact the prognostic prediction of advanced diseases, especially for patients with the N3 diseases.
Recently, International Gastric Cancer Association (IGCA) has proposed a new staging system for gastric cancer. This system shares the same TNM classification with the AJCC7 system but introduces pN3a and pN3b into staging. In this system, all resectable lesions are also stratified into seven groups from IA to IIIC as is the cases with the AJCC7 system [7] and each group is classified according to the number of deaths during five-year period after surgery. The aim of this study was to evaluate the suitability of the IGCA staging system for patients with gastric cancer in China.
Methods
All medical records of gastric cancer patients who received curative surgery in our center from January 2003 to December 2011 were reviewed retrospectively. The criteria for eligibility were histologically proven gastric adenocarcinoma and R0 resection. Patients with M1 lesions (para-aortic LN, hepatic, peritoneal, or other distant metastases) were excluded from this study. Patients who received neoadjuvant therapy were also excluded, knowing that it may affect the assessments of the resected specimen and lead to incorrect staging. Demographic data, clinical features, treatment methods and pathological findings were investigated based on the medical records. Each lesion was classified by TNM classification, and then stratified according to the AJCC7 and IGCA staging systems independently.
Follow-up was carried out in the outpatient department and/or through telephone interviews. The observation endpoint was overall survival (OS). OS was defined as the duration from surgery to the last follow-up or patient death. The Kaplan-Meier method and log-rank test were used to compare OS within patients of different stages. All tests were two-tailed and P < 0.05 was considered statistically significant. All statistical analyses were carried out using SPSS 17.0.
Results
Between January 2003 and December 2011, 1768 consecutive cases were collected, of which 242 were deemed ineligible for the reasons listed in Fig. 1. The clinical and pathologic features of the included patients are listed in Table 1. They included 1024 men and 502 women with a median age of 63 (range 22-95) years at the time of surgery. Patients with early cancers (pT1 stage) only accounted for 19.5%. The number of retrieved LN was 23.60 ± 10.59. The prognosis of N3a subgroup (7–15 involved lymph nodes) was significantly better than N3b (>15 involved LN) (5-year OS, 42.4% vs. 28.7%, P < 0.001, Fig. 2).

List of the ineligible reasons in this study

The distribution of OS curves of N stages
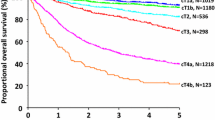
According to the AJCC7 and the IGCA systems, 395 cases were stratified into different stages, and most of them fell in stage III (Table 2). Only one case of T1N3b, which was stratified into stage IIB in AJCC7 shifted to stage IIIB in the IGCA system. So the distribution of patients in stage I and II was quite consistent between the two systems. The survival curves showed dissimilarity in stage III patients of the two systems (Fig. 3). Both AJCC7 and IGCA systems demonstrated a much better OS for IIIA patients than that for IIIB or IIIC patients (P < 0.001, Fig. 3a, b). However, the IGCA system could better stratify stage IIIB and IIIC patients (5-year OS, 38.1% vs. 29.0%; P = 0.005, Fig. 3b) than the AJCC7 system (5-year OS, 38.2% vs. 35.9%; P = 0.148, Fig. 3a).

The distribution of OS curves of the different stages grouped by a.AJCC7 staging system; b. IGCA staging system
Only 332 patients in this cohort with advanced diseases had adjuvant chemotherapy in our center. For these patients, the IGCA system also better stratified the prognoses of patients in different stages than the AJCC7 system (Additional file 1: Figure S1).
Most cases with a stage shift between the two systems were in the following three groups: T3N3b, T4aN2 and T4aN3a (Table 2). The patients in T3N3b had a significant shorter OS than those in T4aN2 (P = 0.003, Fig. 4a) and T4aN3a (P = 0.030, Fig. 4b).

Comparison of the survival of T3N3b, T4aN2 and T4aN3a. a. T3N3b and T4aN2, which were both grouped to III B in AJCC7, were indicated a different survival, P = 0.003. b. T3N3b still had a poorer survival than T4aN3a (III C in AJCC7), P = 0.030. The 5-year survival rate of T3N3b, T4aN2 and T4aN3a was 20.6%, 43.9% and 39.1% respectively
Discussion
The TNM stage is the most important factor used to instruct treatment strategies in patients with gastric cancer and indicate the prognosis. The AJCC7 TNM classification is the latest staging system for gastric cancer and contains major modifications compared with the previous editions. In this edition, N1 stage in the 6th edition is divided into N1 (metastasis in 1-2 regional LN) and N2 (metastasis in 3-6 regional LN) based on the different prognoses. N2 (metastasis in 7-15 regional LN) and N3 (metastasis in more than 15 regional LN) in the 6th edition are defined as N3a and N3b in the AJCC7. It was found in this study that survival was much better in patients with N3a stage than that in patients with N3b stage, which is consistent with the existing literature [6, 8, 9]. This result was also recognized in the AJCC7 staging system. However, N3a and N3b were still grouped together as N3 for TNM staging, which could impact the proper prediction of the stage-based prognosis.
In contrast, the IGCA took N3a and N3b separately and established a new staging system in order to better stratify gastric cancer patients with different prognoses. In this staging system, every N3 stage is subdivided into N3a and N3b, whereby patients are divided into 25 TNM subgroups (Table 2) when M1 was excluded [7]. However, compared with the AJCC7 staging system, only seven TNM subgroups (T1N3b, T2N3b, T3N3b, T4aN2, T4aN3a, T4bN0 and T4bN2) have stage shift in IGCA system. T2N3b, T3N3b, T4aN2, T4aN3a, T4bN0 and T4bN2 all fall in stage III in both AJCC7 and IGCA systems but classified into different groups. Although T1N3b shifts from stage IIB in the AJCC7 system to stage IIIB in the IGCA system, there are rare patients in this subgroup. The IGCA system mostly redistributes patients in the three groups (IIIA, IIIB and IIIC) of stage III.
It was found in this study that the AJCC7 system excellently separated the survival curves of stage IIIA from IIIB and IIIC, but failed to discriminate the prognosis of patients in stage IIIB and stage IIIC. The IGCA systems precisely stratified the survival probabilities of patients in IIIA, IIIB and IIIC. This change is obviously due to the stage shift of the seven TNM subgroups mentioned above. 395 cases were included in the seven groups and most of them were stageIII in the AJCC7 or IGCA systems except for one T1N3b case. Since T1N3b (n = 1), T2N3b (n = 3), T4bN0 (n = 5) and T4bN2 (n = 1) contained very few cases, the stage shift of the other three subgroups (T3N3b, T4aN2 and T4aN3a) played a leading role on the change of survival curves in stage III. The results of this study indicate that the three subgroups are not properly staged in the AJCC7 systems. T3N3b and T4aN2 are both in IIIB, but the 5-year survival rate of T4aN2 (43.9%) was much better than that of T3N3b (20.6%). Even T4aN3a in stage IIIC had a better survival than T3N3b. The improper staging is revised in the IGCA staging system. The 5-year survival rate of T4aN3a was 39.1%, which perfectly matched that of stage IIIB (38.1%) in the IGCA system. As a matter of fact, the 5-year survival rate of T3N3b was even poorer than stage IIIC disease. Whether this subgroup, together with T4N3b [6], should be considered as stage IV diseases needs further assessment [10–12].
As mentioned above, the IGCA system shows almost no revision of stage I and II in AJCC7, suggesting that the IGCA staging system does not seem to make up for the defects of AJCC7 on the earlier stages of the disease. When the IGCA staging system is used, more regional LN should be harvested, for less than a minimum number of 16 retrieved LN could cause stage migration by inaccurate LN staging. Besides, an improved survival outcome was reported to be associated with more lymph node harvested (>15) [13–15]. However, the threshold for the harvested LN counts needs to be further studied.
This retrospective study has certain limitations. Firstly, although all the patients in this cohort underwent surgery in our center, many of them did not receive subsequent standard adjuvant therapy here owing to their different sources and economic reasons, which might impact the prognostic assessment. We only analyzed the data of patients who received adjuvant chemotherapy in our own center. The IGCA staging system still showed a better performance in prognostic stratification as indicated in Additional file 1: Figure S1. Secondly, according to the 6th AJCC staging systems, the lesions in esophagogastric junction (EGJ) were not distinguished from those in the upper part of the stomach in this cohort. Although EGJ tumors were recommended to be staged as esophageal cancers [16], some current studies had indicated that the adenocarcinoma of EGJ (Siewert II and Siewert III) showed similar clinical and pathological characteristics to the disease derived from stomach and should be considered as gastric cancer [17, 18].
Conclusions
In summary, after taking pN3a and pN3b as separate groups, the IGCA system indicates a dissimilarity of survival curves in stage III patients with comparison to AJCC7 system. The result of the present study seems to indicate that the IGCA system is more accurate than the AJCC7 system in stratifying survival of patients with gastric cancer in stage III.
Abbreviations
- AJCC:
-
American joint committee on cancer
- EGJ:
-
Esophagogastric junction
- IGCA:
-
International gastric cancer association
- JCGC:
-
Japanese classification of gastric carcinoma
- LN:
-
Lymph node
- OS:
-
Overall survival
References
Goggins WB, Wong GK. Poor survival for US Pacific islander cancer patients: evidence from the surveillance, epidemiology, and end results database: 1991 to 2004. J Clin Oncol Off J Am Soc Clin Oncol. 2007;25(36):5738–41.
Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin. 2008;58(2):71–96.
Aurello P, D'Angelo F, Rossi S, Bellagamba R, Cicchini C, Nigri G, Ercolani G, De Angelis R, Ramacciato G. Classification of lymph node metastases from gastric cancer: comparison between N-site and N-number systems. Our experience and review of the literature. Am Surg. 2007;73(4):359–66.
Chae S, Lee A, Lee JH. The effectiveness of the new (7th) UICC N classification in the prognosis evaluation of gastric cancer patients: a comparative study between the 5th/6th and 7th UICC N classification. Gastric cancer: official journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association. 2011;14(2):166–71.
Deng J, Liang H, Sun D, Wang D, Pan Y. Suitability of 7th UICC N stage for predicting the overall survival of gastric cancer patients after curative resection in China. Ann Surg Oncol. 2010;17(5):1259–66.
Sun Z, Wang ZN, Zhu Z, Xu YY, Xu Y, Huang BJ, Zhu GL, Xu HM. Evaluation of the seventh edition of American Joint committee on cancer TNM staging system for gastric cancer: results from a Chinese monoinstitutional study. Ann Surg Oncol. 2012;19(6):1918–27.
Sano T, Coit DG, Kim HH, Roviello F, Kassab P, Wittekind C, Yamamoto Y, Ohashi Y. Proposal of a new stage grouping of gastric cancer for TNM classification: International Gastric Cancer Association staging project. Gastric Cancer. 2017;20(2):217–25.
Marrelli D, Morgagni P, de Manzoni G, Coniglio A, Marchet A, Saragoni L, Tiberio G, Roviello F. Italian research Group for Gastric C: prognostic value of the 7th AJCC/UICC TNM classification of noncardia gastric cancer: analysis of a large series from specialized western centers. Ann Surg. 2012;255(3):486–91.
Ahn HS, Lee HJ, Hahn S, Kim WH, Lee KU, Sano T, Edge SB, Yang HK. Evaluation of the seventh American Joint committee on cancer/International Union against Cancer classification of gastric adenocarcinoma in comparison with the sixth classification. Cancer. 2010;116(24):5592–8.
Li FX, Zhang RP, Liang H, Quan JC, Liu H, Zhang H. Validity and necessity of sub-classification of N3 in the 7th UICC TNM stage of gastric cancer. Asian Pacific journal of cancer prevention: APJCP. 2013;14(3):2091–5.
Yeh CN, Wang SY, Hsu JT, Chiang KC, Cheng CT, Tsai CY, Liu YY, Liao CH, Liu KH, Yeh TS. N3 subclassification incorporated into the final pathologic staging of gastric cancer: a modified system based on current AJCC staging. Medicine. 2015;94(8):e575.
Warneke VS, Behrens HM, Hartmann JT, Held H, Becker T, Schwarz NT, Rocken C. Cohort study based on the seventh edition of the TNM classification for gastric cancer: proposal of a new staging system. J Clin Oncol Off J Am Soc Clin Oncol. 2011;29(17):2364–71.
Yang K, Zhang WH, Hu JK. Lymph node count as a quality measure for gastric cancer surgery. JAMA surgery. 2015;150(6):595–6.
Morgan JW, Ji L, Friedman G, Senthil M, Dyke C, Lum SS. The role of the cancer center when using lymph node count as a quality measure for gastric cancer surgery. JAMA surgery. 2015;150(1):37–43.
Biondi A, D'Ugo D, Cananzi FC, Papa V, Borasi A, Sicoli F, Degiuli M, Doglietto G, Persiani R. Does a minimum number of 16 retrieved nodes affect survival in curatively resected gastric cancer? European journal of surgical oncology: the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2015;41(6):779–86.
Rice TW, Rusch VW, Ishwaran H, Blackstone EH. Worldwide esophageal cancer C: cancer of the esophagus and esophagogastric junction: data-driven staging for the seventh edition of the American Joint committee on cancer/International Union against Cancer cancer staging manuals. Cancer. 2010;116(16):3763–73.
Suh YS, Han DS, Kong SH, Lee HJ, Kim YT, Kim WH, Lee KU, Yang HK. Should adenocarcinoma of the esophagogastric junction be classified as esophageal cancer? A comparative analysis according to the seventh AJCC TNM classification. Ann Surg. 2012;255(5):908–15.
Kim HI, Cheong JH, Song KJ, An JY, Hyung WJ, Noh SH, Kim CB. Staging of adenocarcinoma of the esophagogastric junction: comparison of AJCC 6th and 7th gastric and 7th esophageal staging systems. Ann Surg Oncol. 2013;20(8):2713–20.
Acknowledgements
Not applicable.
Funding
Funded by Shanghai Municipal Planning Commission of Health and Family Planning, 201,540,047. The funding mainly contributes to the cost of data collection and follow-up of the patients in this study.
Availability of data and materials
The datasets used and analyzed during the current study available from the corresponding author on reasonable request.
Authors’ contributions
The current study was designed by ZS, YS, XQ. The study materials and patients were provided by ZS, KS, YS, XQ. PS, JQ, WC, FL, YF, XW, HW collected and assembled the data. PS, JQ analyzed and interpreted the data. PS was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This retrospective study was approved by the Ethics Committee of the Scientific Research Board of Zhongshan Hospital affiliated to Fudan University (Shanghai, China). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. The written informed consent covered the entire study including the telephone interview.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and Institutional affiliations.
Author information
Authors and Affiliations
Corresponding authors
Additional file
Additional file 1: Figure: S1.
The survival distributions of 332 patients who received adjuvant chemotherapy in our own center. a The survival distributions of different stages Grouped by AJCC7 staging system. It was unable to distinguish the OS difference between III B and III C diseases (P = 0.958); b The survival distributions of different stages Grouped by IGCA staging system. The survival of III B and III C diseases were perfectly stratified (P = 0.003). (TIFF 5298 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Shu, P., Qin, J., Shen, K. et al. The IGCA staging system is more accurate than AJCC7 system in stratifying survival of patients with gastric cancer in stage III. BMC Cancer 17, 238 (2017). https://doi.org/10.1186/s12885-017-3235-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-017-3235-3