
Abstract
Background
There is a paucity of specific data on early stages of chronic kidney disease (CKD) among Asian Americans (AAs). The objective of this study was to examine the independent association of Asian race/ethnicity and socio-demographic and co-morbidity factors with markers of early kidney damage, ascertained by ACR levels, as well as kidney dysfunction, ascertained by eGFR levels in a large cross-sectional sample of AAs enrolled in the National Health and Nutrition Examination Survey (NHANES).
Methods
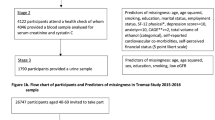
Secondary data analyses of the NHANES 2011–2014 data of a nationally representative sample of 5907 participants 18 years and older, US citizens, and of Asian and White race. NHANES data included race (Asian vs. White), as well as other socio-demographic information and comorbidities. Urine albumin-to-creatinine ratio (ACR) categories and estimated glomerular filtration rate (eGFR) were used as indicators for CKD. Descriptive analyses using frequencies, means (standard deviations), and chi-square tests was first conducted, then multivariable logistic regression serial adjustment models were used to examine the associations between race/ethnicity, other socio-demographic factors (age, sex, education), and co-morbidities (obesity, diabetes, hypertension) with elevated ACR levels (A2 & A3 – CKD Stages 3 and 4–5, respectively) as well as reduced eGFR (G3a-G5 and G3b –G5 - CKD Stage 3–5).
Results
AAs were more likely than White participants to have ACR levels > 300 mg/g (A3) (adjusted OR (aOR) (95% CI) 2.77 (1.55, 4.97), p = 0.001). In contrast, adjusted analyses demonstrated that AAs were less likely to have eGFR levels < 60 ml/min/1.73 m2 (G3a-G5) (aOR (95% CI) 0.50 (0.35, 0.72), p < .001).
Conclusions
This is one of the first large U.S. population-based studies of AAs that has shown a comparatively higher risk of elevated ACR > 300 mg/g levels (A3) but lower risk of having eGFR levels < 60 ml/min/1.732 m2 (G3a-G5). The findings support the need to address the gaps in knowledge regarding disparities in risk of early stage CKD among AAs.
Similar content being viewed by others


Background
Asian Americans (AA)s are projected to be the second fastest growing racial/ethnic group in the U.S and are projected to nearly double to 9.3% of the total population by 2060 [1]. Currently, AAs represent 5.8% of the overall U.S. population [2] and there are approximately 20.4 million Asian adults and children living in the U.S. [3, 4]. Furthermore based on the 2016 U.S. Census, major Asian subgroups of people reported were Chinese (except Taiwanese) (4.9 million), Asian Indian (4.1 million), Filipino (3.9 million), Vietnamese (2.1 million), Korean (1.8 million), and Japanese (1.5 million).
Thirty million adults in the United States (US) have chronic kidney disease (CKD) [5]. Compared to Whites, the prevalence of end-stage renal disease is 1.5 times greater for AAs [6]. AAs constitute about 5.5% of all patients in the U.S. receiving dialysis [7] and 5% of patients living with a functioning kidney transplant in 2013 [8]. In 2011, total Medicare spending rose 5% to $549.1 billion, while end-stage-renal disease expenditures rose 5.4% to $34.3 billion. In addition, total fee-for-service Medicare expenditures per person per year were $87,945 in 2011 [9]. The costs and spending will continue to increase based on the projected population growth of AAs in the U.S. in the next 50 years. Given these projections, disease prevention are imperative to address in the early stages of CKD among this population. While state-level data exists on end-stage renal disease and its treatment, there are no granular and precise data on early stages of CKD specifically among AAs.
CKD is common in people with cardiovascular disease (CVD), diabetes mellitus (DM), hypertension (HTN), and obesity [10]. DM and HTN are the two major risk factors for CKD worldwide [11] and are listed as the primary causes for 70% of new cases of CKD in the U.S. [12]. The prevalence of DM is approximately 40% higher in AAs relative to Whites [12] and 19% of AAs have HTN [13, 14]. Obesity is disproportionately more prevalent in certain Asian subgroups, is also associated with increased risk of development of CKD [15,16,17] as well as various kidney disease risk factors (e.g., HTN, DM, and dyslipidemia) [18].
There is a paucity of studies exploring the association of albumin to creatinine ratio (ACR) and estimated glomuerular filtration rate (eGFR) with CKD among AAs. International researchers who studied ACR and eGFR with CKD among Asians were from countries such as China, Korea, Japan, and Thailand. Among Asian populations with DM, CKD progresses twice as rapidly [19]. HTN has been associated with CKD among Chinese, Japanese, Filipino, and South Asians [14, 20, 21]. International researchers also found that obesity led to CKD through both indirect (i.e., DM, HTN, dyslipidemia) and direct mechanisms (i.e., glomerular hyperfiltration, inflammation) [22, 23].
Jolly et al. [24] and Mau et al. [25] utilized the U.S. National Kidney Foundation (NKF) Kidney Early Evaluation Program (KEEP) cross-sectional data of community-dwelling racial/ethnic participants and found AAs to have one of the highest odds for CKD based ACR levels. Kataoka-Yahiro et al. [26] and Wong et al. [27] conducted a cross-sectional study of the National Kidney Foundation of Hawaii (NKFH) Kidney Early Screening Program (KEDS) of community dwelling participants to further examine the relationship of risk factors and CKD of Asian Pacific Islanders (Native Hawaiians, Japanese, Chinese, Filipino, and Whites) in Hawaii. ACR and/or urine albumin levels, respectively were used as predictors for CKD. Significant results related to ACR in these studies included BMI, glucose, HTN, and Asian and/or Pacific Islander race/ethnicity.
Racial/ethnic differences in ACR and eGFR evaluation and CKD definition and staging among AAs is particularly needed in the early stages of CKD [28, 29]. While impaired ACR and eGFR have been associated with heightened risk of cardiovascular complications and mortality among Asians [30], further research is needed to determine the impact of ACR and eGFR markers of kidney damage and kidney function, respectively, in AA populations.
Hence, identification of CKD in its earlier stages is a high priority in the AA population [27]. Thus, to better inform the field, we sought to examine the relationship between Asian race/ethnicity and CKD indicators among a nationally representative cohort of AA adults. We examined the independent association of Asian race/ethnicity and socio-demographic and co-morbidity factors with markers of early kidney damage, ascertained by higher ACR levels, as well as kidney dysfunction, ascertained by lower eGFR levels. We further examined the association between socio-demographic and co-morbidity factors with these outcomes stratified by race/ethnicity.
Methods
Study design and population
In this study, we examined data from participants enrolled in the National Health and Nutrition Examination Survey (NHANES) [31] over the period of 2011–2014. NHANES is a national population-based survey, designed to assess the health and nutritional status of adults and children in the U.S. The survey is unique in that it combines interviews, physical examinations and laboratory data. In the NHANES study, survey data is obtained via personal household interviews of a stratified, multistage probability sample of the civilian, non-institutionalized population of the U.S. Data from the NHANES were de-identified and provided as downloadable public-use data files.
Participants included were 18 years and older and of AA or non-Hispanic White race/ethnicity. Participants were excluded if they were pregnant women, if their race was Mexican-American or other Hispanic categories, non-Hispanic Black, if they were multi-racial, if they did not identify their race/ethnicity, and if their sampling weights were missing or zero. After the exclusions, the sample included 5907 non-Hispanic Asian and non-Hispanic White participants (referred to in the remainder of the study as Asian and White participants, respectively).
Measurements and definitions
The primary predictor of interest was race/ethnicity, which was categorized in analyses as Asian and White. In the NHANES study, race/ethnicity information was self-reported by participants. Other predictors included were age, sex, education (measured for SES), DM, HTN, and BMI.
The primary outcomes of interest were ACR and eGFR [9]. ACR was analyzed at two cutpoints: (1) ≥ 30 mg/g (Kidney Disease Improving Global Outcomes [KDIGO] category A2 – CKD Stage 3), and (2) > 300 mg/g (KDIGO category A3 – CKD Stages 4 & 5) [32]. ACR was calculated as urine albumin (mg/dL) divided by urine creatinine (g/dL ratio). In the NHANES study, ACR specimens (urine albumin and urine creatinine) were measured in a random urine collection by the Mobile Examination Center (MEC) (first collection) and a first morning void urine collected by the participant at home (second collection). eGFR was examined at two thresholds chosen as (1) < 60 ml/min/1.73m2 (KDIGO category G3a – G5 - Stages 3–5), and (2) < 45 ml/min/1.73m2 (KDIGO category G3b –G5 - Stage 3–5). We specifically selected these cut-points as indicators of moderate vs. severe CKD, respectively. The eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation: eGFR = 141 x min (Scr/k,1)α x max (Scr/k,1)-1.209 × 0.993Age × 1.018 [if female], where, Scr is serum creatinine in mg/dl, k is 0.7 for females and 0.9 for males, α is − 0.329 for females and − 0.411 for males, min indicates the minimum of Scr/k or 1, and max indicates maximum of Scr/k or 1 [33].
Statistical analyses
Descriptive statistics for the survey data were summarized by frequencies and percentages for categorical variables, and by means and standard deviations or medians and interquartile ranges for continuous variables, depending on the distributions. Bivariate analyses used Rao-Scott chi-square tests to assess associations between the outcomes ACR and eGFR and other factors.
Multivariable logistic regression analyses were used to examine the association between race/ethnicity, other socio-demographic factors, and comorbidities with elevated ACR, and reduced eGFR, based upon the chosen cut points. The analyses accounted for confounding by age (categorized as 18–64, 65–74, 75 and older years), education (≤ high school/GED, some college, college graduate), sex (male, female), BMI (categorized as normal [< 25.0 kg/m2], overweight [25.0–29.9 kg/m2] and obesity [≥30.0 kg/m2]), and presence of self-reported DM (yes or no) and HTN (yes or no). In secondary analyses, logistic regression models were fit stratified by race/ethnicity using the cut-points for ACR ≥30 mg/g and > 300 mg/g and for eGFR < 60 and < 45 ml/min/1.73m2. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs).
All analyses accounted for the NHANES’s complex multistage sampling design in order to ensure that calculated estimates were representative of the U.S. civilian non-institutionalized population. A value of p < 0.05 was considered statistically significant. Statistical analyses were conducted using SAS software, version 9.4 [34]. Figures were generated using R version 3.0.2.
Results
Study population
After applying the eligibility criteria, the final study population comprised 5907 Asian and White participants. The total sample size for the ACR analyses was 5792 (115 participants were missing ACR data), and 5605 for the eGFR analyses (302 participants were missing eGFR data). Table 1 provides participants’ descriptive characteristics stratified by race/ethnicity. Asians were more likely than Whites to be 18–64 years of age (86% vs. 79%), college graduates (49.9% vs. 34.4%), have normal weight (60% vs. 31%) and less frequently had HTN (22% vs 34%). Descriptive statistics by race/ethnicity for the outcomes, ACR and eGFR are summarized in Table 2. Asians had higher mean and median levels of ACR than Whites when compared for ACR overall and when examined at A2 and A3 (CKD Stages 3 and 4–5, respectively), ACR levels were skewed towards high values rendering means much higher than medians; thus the median comparisons may be preferable. eGFR levels were reasonably normally distributed and means and medians were similar. Asians has a higher mean overall but the Asian and White means were comparable at levels of G3a–G5 and G3b-G5 (CKD Stage 3–5).
Comparison of Asians and whites in serially-adjusted, multivariable logistic regression models for ACR ≥ 30 mg/g and ACR > 300 mg/g (A2 and A3) and eGFR < 60 ml/min/1.73 m2 and eGFR < 45 ml/min/1.73 m2 (G3a-G5 and G3b-G5)
The ACR levels of Asians and Whites were compared using four models of serial adjustments: unadjusted; age- and sex-adjusted; age-, sex- and education adjusted, including education as a measure of socioeconomic status; and a model with additional adjustment for health characteristics (normal, overweight, obesity, DM, and HTN). For ACR levels ≥30 mg/g differences were not significant in the unadjusted model, but with age-, sex-adjustment and with further adjustment, Asians had increasing odds of higher ACR levels than Whites at 1.35 (95% CI = 1.05, 1.74, weighted p-value = 0.020) (Table 3; Fig. 1). Significant socio-demographic and co-morbidity factors were (a) age 65–74 and 75 and older with odds ratios of 1.39 and 3.19, (95% CI = 1.02, 1.89; 2.43, 4.17), respectively; (b) BMI overweight with an odds ratio of − 0.65 (95% CI = 0.49, 0.88); (c) DM with an odds ratio of 2.89 (95% CI = 2.20, 3.79); and (d) HTN with an odds ratio of 1.77 (95% CI = 1.38, 2.27). Using ACR of > 300 mg/g, Asians had significantly higher odds in all of the serial-adjusted models reaching an odds ratio of 2.77 in the fully adjusted model (95% CI = 1.55, 4.97, weighted p-value = 0.001). Significant socio-demographic and co-morbidity factors were (a) age 75 and older with an odds ratio of 3.79 (95% CI = 1.91, 7.52); (b) DM with odds ratio of 7.68 (95% CI = 4.24, 13.92); and (c) HTN with odds ratio of 3.6 (95% CI = 1.77, 7.29) (Table 3; Fig. 1). At the eGFR level of < 60 ml/min/1.73 m2, Asians consistently had lower odds compared to Whites in all of the serial adjusted models. The odds ratio went from 0.38 (95% CI = 0.27–0.52, weighted p-value = < 0.001) in the unadjusted model to 0.50 (95% CI = 0.35, 0.72, weighted p-value = < 0.001) in the fully adjusted model (Table 4; Fig. 2). Significant socio-demographic and co-morbidity factors were (a) ages 65–75 and 75 and older with odds ratios of 4.99 and 17.15 (95% CI = 3.53, 7.06 and 12.45, 23.61), respectively; (b) DM with an odds ratio of 2.21 (95% CI = 1.61, 3.03); and (c) HTN with an odds ratio of 2.7 (95% CI = 2.02, 3.61). For eGFR < 45 ml/min/1.73m2, Asians had a significantly lower odds than Whites in the unadjusted model [odds ratio = 0.39 (95% CI = 0.22, 0.67, weighted p-value = 0.001)] but the odds ratio increased and became non-significant with age-, sex- adjustment, and remained non-significant with adjustment for additional covariates [odd ratio = 0.62 (95% CI = 0.33, 1.17, weighted p-value = 0.139) (Table 4: Fig. 2).

Comparison of Asians & Whites in Multivariable Logistic Regression Models Adjusted for ACR ≥30 mg/g (A2) and ACR > 300 mg/g (A3)

Comparison of Asians & Whites in Adjusted Multivariable Logistic Regression Models for eGFR < 60 mg/ml/1.73 m2 and eGFR < 45 mg/ml/1.73 m2
Association of Other Socio-Demographic and Comorbidities with CKD outcomes across racial/ethnic subgroups
To better understand the risks of Asians and Whites, separate models were fit for the two ethnicities. For ACR levels ≥30 mg/g, diabetes (p = 0.001) and having hypertension (p = .022) were significant risk factors for both Asians and Whites and only sex for Whites (p = 0.000) (Additional file 1: Table S1). For ACR levels > 300 mg/g DM was significant risk factor for both ethnicities (p = 0.032 and 0.000, respectively). Older age and HTN was also significant for Whites (p = 0.000 and p = 0.002, respectively) (Additional file 1: Table S2). For eGFR < 60 ml/min/1.73 m2, older age (p = 0.000), DM (p = 0.001 and 0.000, respectively), and having HTN (p = 0.003 and 0.000), were significant risk factors for Asians and for Whites (Additional file 1: Table S3). Results had a similar pattern using eGFR < 45 ml/min/1.73 m2 although statistical significance was not observed (Additional file 1: Table S4).
Discussion
The objective of this study was to examine the relationship of Asian race/ethnicity, socio-demographic and co-morbidity factors, and CKD outcomes in a nationally representative sample of AAs and Whites who were enrolled in the NHANES study from 2011 to 2014. To our knowledge, this is one of the first large U.S. population-based studies that has shown a comparatively higher risk of elevated ACR levels (A3), an early marker of kidney damage, among Asians compared to Whites.
CKD is defined as the abnormality of kidney structure or function, present for > 3 months, with varying implications upon health status and CKD Stages 1 to 5 depending upon underlying cause. In this study, the ACR and eGFR levels of Asians and Whites were compared using four models of serial adjustments for socio-demographic and co-morbidity factors, adjusted and unadjusted. With adjustment, ACR was a key determinant of CKD [35, 36]. In this study, socio-demographic and co-morbidity factors which were significant for KDIGO-defined A2, A3, and G3a-G5 were related to age, DM, and HTN independent of race/ethnicity. Similarly, when race/ethnicity was stratified into Asian and White; age, DM, and HTN were significant factors related to A2, A3, and G3a-G5. These results were consistent with the existing literature [24,25,26,27]. Other studies also indicated that albuminuria was an important correlate of HTN among patients with CKD [37, 38] as well as an indicator of insulin resistance [39,39,, 40]. Age was the best correlate of low eGFR (eGFR < 60 ml/min/1.73m2) while HTN was the greatest predictor of albuminuria [41]. In this study, obesity was a significant independent factor worth mentioning for A2, but not for A3 or eGFR of 60 ml/min/1.73m2. There were several studies which support this study finding [42, 43], but obesity was not a consistent finding in this study with ACR or eGFR. In this study, albuminuria and eGFR prevalence was independently higher among participants who were (a) older, (b) with DM, (c) had HTN, and (d) of Asian background. These findings suggest a need for access to early screening and detection of kidney damage in the community [24, 26, 27, 44]. More specifically, targeted programs which include not only CKD early screening, but also encompasses the identification of CVD risk factors (HTN, DM, Obesity) inclusive of culturally appropriate screening, detection, referral, and intervention in routine kidney screening [24, 26].
In this study, we observed that Asian participants had a 2.77-fold higher risk of KDIGO-defined albuminuria categories A3 and a trend towards higher risk of category A2. Studies of AA samples have also similar results of a trend towards higher risk of albuminuria category A2 [24, 26, 27, 45, 46]. There is a paucity of studies which have found a higher risk of albuminuria category A3 among AA participants compared to their non-Hispanic White counterparts. Possible reasons to consider to explain this apparent higher risk may include diet [47], genetic or environmental [45, 48,49,50], urine specimen procedure [51, 52], and other laboratory values [53, 54]. Sato et al. [47] analyzed 675 men and 924 women who did not have DM and found those who had less animal protein and more B-cryptoxanthin in the diet did not have abnormal microalbuminuria in comparison to those who ingested n-3 polyunsaturated fatty acids. Sakamoto et al. [50] found YKL-40 levels were significantly elevated in type 1 diabetic patients than in healthy controls and demonstrated YKL-40 levels were a determinant of ACR independent of other risk factors. Prior et al. [55] found a significant association between genotype (GG/GA/AA) and urinary albumin (normoalbumuria vs. micro/macroalbuminuria, p = 0.01). Mashima et al. [56] single nucleotide polymorphisms (SNPs) in six proinflammatory cytokine genes IL-6 and CCL1 genes were associated with albuminuria and the combination of these genotypes had an additive effect on the prevalence and severity of albuminuria.
Matsushita et al. [51] reported that measurements of creatinine and albuminuria were not standardized. In some studies, researchers measured creatinine and albuminuria using fresh samples while others used frozen samples which may have an effect on the validity of results for both eGFR and albuminuria. Carter et al. [52] described the influence of urine creatinine concentrations on the relation of albumin-creatinine ratio with cardiovascular disease events from the Multi-Ethnic Study of Athersclerosis (MESA). Carter et al. found urine creatinine was lower in older female, and White and Chinese participants, and those with lower body weight (reflecting lower muscle mass). The urine tonicity may make spot urine creatinine a less reliable marker of muscle mass than 24 h urine creatinine.
In this study, we utilized the CKD-EPI Creatinine Equation based on the CKD Prognosis Consortium (CKD-PC) [57,58,59]. The CKD-PC provided a comprehensive method to define and stage CKD, eGFR, and albuminuria on kidney outcomes.
In our analyses of kidney function defined by eGFR as the outcome of interest, we observed contrasting associations, such that Asians had a lower risk of mild to moderately reduced eGFR (< 60 ml/min/1.73m2) compared to Whites. There are limitations in the application of creatinine-based GFR estimating equations. For example, the equation ascertaining kidney function using these methods were not specifically derived from AA populations and cannot overcome the limitations of serum creatinine as a filtration marker, which may be lower in Asian populations due to lower generation of creatinine from muscle. Indeed, several studies have proposed using an Asian-specific ethnic equation for the Chronic Kidney Disease Epidemiology Collaboration formula analysis. Hence, in our study the eGFR findings must be carefully interpreted, and further studies are needed to define what ethnic equation may be used for AAs. A limitation in the use of serum creatinine to eGFR ratio within this study is that the ratio is different among various Asian subgroup populations. For example, Horio et al. [60] and Teo et al. [61] reported the correction factors of Chinese, Malay, and Indians/other (1.100, 1.032, and 0.996 for the CKD-EPI equation, respectively). However, in the NHANES cohort, AAs were examined as a single non-granular sub-group. Levey, Becker, and Inker [33] have recommended for the initial assessment of eGFR, measuring serum creatinine and reporting eGFR be based on CKD-EPI 2009 equation. They also mentioned if there is difficulty to confirm the eGFR results based on “extremes of muscle mass, diet, interference of assay”, cystatin C should be measured and eGFR should be measured directly using clearance procedure rather than initial assessment of albuminuria measuring urine albumin and creatinine based on ‘spot’ urine collection and reporting of ACR (p.1, 5–6). Hence, further studies are needed to determine the role of cystatin C and cystatin-C based eGFR assessment among the AA population and individual subgroups.
Our study has a number of strengths, including its examination of a large nationally represent cohort of healthy U.S. participants with a large sample of AAs; comprehensive availability of detailed information, including socio-demographic and comorbidity data; and rigorous analytic approaches that examined various thresholds of ACR and eGFR and accounted for key confounders of the Asian race/ethnicity - CKD associations. However, several limitations of our study should be acknowledged. First, given the study’s cross-sectional and observational nature, our findings do not confirm causal associations. Second, as socio-demographic and comorbidity data were self-reported by the participants, it is possible that the participants’ responses may be affected by biases. Participants who self-reported and self-selected to be in this study may not be representative of the general population. This study did not report on lab values, medications, or management of HTN, DM, obesity, or CKD which could provide additional objective information along with self-reported data. Third, since AAs were aggregated in the NHANES cohort, the results may not be generalizable to Asian subgroups. Fourth, the definition of eGFR is based on single assessment of serum creatinine which may introduce misclassification bias. Low muscle mass and serum creatinine and creatinine generation in AAs may also affect the denominator in the ACR ratio, thereby falsely augmenting ACR among this population.
Conclusions
In conclusion, our findings suggest that AAs are at higher risk of early damage manifested by abnormal levels of albuminuria. It is important to continue to explore and examine large cohorts or longitudinal studies on AAs and sub-groups in order to accurately identify CKD prevalence in community dwelling populations. Valid and reliable outcome measures of ACR and eGFR are needed to examine the relationship to socio-demographic and co-morbidity risk factors in efforts to justify a need to target culturally appropriate early screening, detection, referral, and intervention in community settings.
Abbreviations
- AA:
-
Asian American
- ACR:
-
Urine albumin-to-creatinine ratio
- BMI:
-
Body Mass Index
- CKD:
-
Chronic Kidney Disease
- CVD:
-
Cardiovascular disease
- DM:
-
Diabetes mellitus
- eGFR:
-
Estimated glomerular filtration rate
- HTN:
-
Hypertension
- KEDS:
-
Kidney Early Screening Program
- KEEP:
-
Kidney Early Evaluation Program
- MDRD:
-
Modification of Diet in Renal Disease
- NHANES:
-
National Health and Nutrition Examination Survey
- OR:
-
Odds ratio
- U.S.:
-
United States
References
Colby S, Ortman JM. Projections of the size and composition of the U.S. population: 2014 to 2060. In: Current Population Reports. Washington, DC: Census Bureau; 2014. p. P25–1143.
U.S. Census Bureau. https://www.census.gov/quickfacts/fact/table/US/RHI125217. Accessed 1 Dec 2018.
U.S. Census Bureau. FFF. Asian-American and Pacific Islander heritage month: May 2018. Release Number: CB18-FF.or. https://www.census.gov/newsroom/facts-for-features/2018/asian-american.html. Accessed 1 Dec 2018.
Lopez G, Ruiz NG, Patten E. Key facts about Asian Americans, a diverse and growing population. Pew Research Center. 2017. http://www.pewresearch.org/fact-tank/2017/09/08/key-facts-about-asian-americans/. Accessed 1 Dec 2018.
Global Nation. https://www.cdc.gov/kidneydisease/basics.html. Accessed 1 Dec 2018.
National Institute of Diabetes, Digestive, and Kidney Diseases. https://www.niddk.nih.gov/health-information/health-statistics/kidney-disease. Accessed 1 Dec 2018.
U.S. Renal Data Systems. https://www.kidney.org/news/newsroom/factsheets/Demographics-of-Kidney-Disease. Accessed 1 Dec 2018.
U.S. Renal Data System. https://www.usrds.org/2016/view/v2_07.aspx. Accessed 1 Dec 2018.
Levey AS, Atkins R, Coresh J, et al. Chronic kidney disease as a global public health problem: approaches and initiatives – a position statement from kidney disease improving global outcomes. Kidney Int. 2007. http://www.kdigo.org/pdf/Levey_KI_2007.pdf. Accessed 1 Dec 2018.
Zhang QL, Rothenbacher D. Prevalence of chronic kidney disease in population-based studies: systematic review. BMC Public Health. 2008;11(8):117. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-8-117. Accessed 1 Dec 2018.
Centers for Disease Control and Prevention: National chronic kidney disease fact sheet: General information and national estimates on chronic kidney disease in the U.S. Atlanta: USDHHS, Centers for Disease Control and Prevention; 2014. https://www.cdc.gov/kidneydisease/pdf/kidney_factsheet.pdf. Accessed 1 Dec 2018.
Grandinetti A, Chang HK, Mau MK, et al. Prevalence of glucose intolerance among native Hawaiians in two rural communities. Native Hawaiian Health Research (NHHR) project. Diabetes Care. 1998;21(4):549–54.
Go AS, Mozaffarian D, Roger VL, et al. American Heart Association statistics committee and stroke statistics subcommittee. Heart disease and stroke statistics – 2013 update: a report from the American Heart Association. Circulation. 2013;127:e6–e245.
Major RW, Davies MJ, Crasto W. Association between undiagnosed hypertension and microalbuminuria in south Asians without known diabetes. J Hum Hypertens. 2015;29(3):185–9.
Park Y, Wang S, Kitahara CM, et al. Body mass index and risk of death of Asian Americans. Am J Public Health. 2014;104(3):520–5.
Reynolds K, Gu D, Muntner P, et al. Body mass index and risk of ESRD in China. Am J Kidney Dis. 2007;50(5):754–64.
Foster MC, Hwang S-J, Larson MG, et al. Overweight, obesity, and the development of stage 3 CKD. Framingham Heart Study. 2008;52(1):39–48.
Echeverria SE, Mustafa M, Pentakota SR, et al. Social and clinically-relevant cardiovascular risk factors in Asian American adults: NHANES 2011-2014. Prev Med. 2017;99:222–7. https://doi.org/10.1016/j.ypmed.2017.02.016 Epub 2017 Feb 17.
Vejakama P, Ingsathit A, Attia J, et al. Epidemiological study of chronic kidney disease progression: a large-scale population-based cohort study. Medicine. 2015;94(4):1–8.
Mau MK, West MR, Shara NM, et al. Epidemiologic and clinical factors associated with chronic kidney disease among Asian Americans and native Hawaiians. Ethnicity Health. 2007;12(2):111–27.
Konta T, Hao Z, Abiko H. Prevalence and risk factor analysis of microalbuminuria in Japanese general population: the Takahata study. Kidney Int. 2006;70:751–6.
Park J, Ahmadi SF, Streja E, et al. Obesity paradox in end-stage kidney disease patients. Progressive Cardiovascular Disease. 2014;56(4):415–25.
Rhee CM, Ahmadi S-F, Kalantar-Zedeh K. The dual roles of obesity in chronic kidney disease: a review of the current literature. Current Opinion. 2016;25(3):208–16.
Jolly SE, Burrows NR, Chen S-C, Li S, Jurkovitz CT, Narva AS, Norris KC, Shlipak MG. Racial and ethnic differences in albuminuria in individuals with estimated GFR greater than 60 ml/min/1.73m2: results from the kidney early evaluation program (KEEP). Am J Kidney Dis. 2010;55(3 Suppl 2):S15–22.
Mau M, West M, Shara NM, Efird JT, Alimineti K, Saito E, Sugihara J, Ng R. Epidemiologic and clinical factors associated with chronic kidney disease among Asian Americans and native Hawaiians. Ethnicity & Health. 2007;12(3):111–27.
Kataoka-Yahiro MR, Page V, Li D. Relationship of associated cardiovascular risk factors and chronic kidney disease with participants enrolled in the National Kidney Foundation of Hawai’i kidney early detection screening (KEDS) program. J Health Disparities Res Pract. 2016;9(3):66–79.
Wong LL, Kalantar-Zadeh K, Page V, et al. Insights from screening a racially and ethnically diverse population for chronic kidney disease. Am J Nephrol. 2017;45:200–8.
Matsushita K, van der Velde M, Astor BC. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality: a collaborative meta-analysis of general population cohorts. Lancet. 2010;375(9731):2073–81.
Derose SF, Rutkowski MP, Crooks PW, et al. Racial differences in estimated GFR decline, ESRD, and mortality in an integrated health system. Am J Kidney Dis. 2013;62(2):236–44.
Wada T, Haneda M, Furuichi K, et al. Clinical impact of albuminuria and glomerular filtration rate on renal and cardiovascular events, and all-cause mortality in Japanese patients with type 2 diabetes. Clinical Exp Nephrology. 2014;18(4):613–20.
National Health and Nutrition Examination Survey (NHANES). https://www.cdc.gov/nchs/nhanes/. Accessed 1 Dec 2018.
Inker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014. https://www.kidney.org/sites/default/files/docs/inker_et_al_ajkd_ckd_commentary_epub.pdf. Accessed 1 Dec 2018.
Levey AS, Becker C, Inker LA. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: a systematic review. JAMA. 2015;313(8):837–46.
SAS Institute Inc. SAS® 9.4 System Options: Reference, Fifth Edition. Cary: SAS Institute In; 2016.
Rosansky SJ. Renal function trajectory is more important than chronic kidney disease stage for managing patients with chronic kidney disease. Am J Nephrol. 2012;36:1–10.
Amin P A, Whaley-Connell A T, Li S. The synergistic relationship between estimated GFR and microalbuminuria in predicting long-term progression to ESRD or death in patients with diabetes: results from the kidney early evaluation program (KEEP). Am J Kidney Dis. 2013;61(4)(suppl.2):S12-S23.
Joshi V, Mooppil N, Lim J. Prevalence and risk factors of undetected proteinuria in an elderly south-east Asian population. Nephrology. 2006;11:347–54.
Koroshi A. Microalbuminuria, is it so important. HIPPOKRATIA. 2007;11(3):105–7.
Agarwal R. Epidemiology of chronic kidney disease among normotensives: but what is chronic kidney disease. Hypertension. 2010;55(5):1097–9.
Sugawara A, Kawai K, Motohashi S, Saito K, Kodama S, Yachi Y, et al. HbA(1c) variability and the development of microalbuminuria in type 2 diabetes: Tsukuba Kawai diabetes registry 2. Diabetologia. 2012;55(8):2128–31.
U.S. Renal Data Systems. Chapter 1: CKD in the general population. https://www.usrds.org/2017/view/v1_01.aspx
Matsushita K, Yasuda G, Shouda M, Umemura S. Evaluation of renal function and proteinuria based on mass health examinations in young Japanese obese adults. Clinical Exp. Nephrology. 2009;13:316–24.
Lee JWR, Brancati FL, Yeh H-C. Trends in the prevalence of type 2 diabetes in Asians versus whites. Diabetes Care. 2011;34:353–7.
Kataoka-Yahiro MR, Wong KA, Tamashiro J, Page V, Ching J, Li D. Evaluation of the National Foundation of Hawaii’s kidney early detection screening program. Hawaii J Med & Public Health. 2012;71(7):186–92.
Choi AI, Karter AJ, Liu JY, Young BA, Go AS, Schillinger D. Ethnic differences in the development of albuminuria: The DISTANCE study. Am J Manag Care. 2011;17(11):737–45.
Kataoka-Yahiro MR, Wong KA, Tamashiro J, Page V, Ching J, Li D. Evaluation of the National Foundation of Hawaii’s kidney early detection screening program. Hawaii Journal of Medicine & Public Health. July 2012;71(7):186–92.
Sato M, Hozawa A, Konta T, Shao L, Otani K, Narimatsu H, et al. Relationship between dietary intake and microalbuminuria: findings from the Takahata study. Clinical Exp Nephrology. 2012;16(1):147–55.
Prior S, Clark AR, Jones DA, Bain SC, Hurel SJ, Humphries SE, Stephens JW. Association of the PGC-1α rs819678 variant with microalbuminuria in subjects with type 2 diabetes mellitus. Dis Markers. 2012:363–9.
Mashima Y, Konta T, Kudo K, Suzuki K, Ikeda A, Ichikawa K, et al. Polymorphism of proinflammatory cytokine genes and albuminuria in the Japanese general population: the Takahata study. Nephrol Dial Transplant. 2011;26(12):3902–7.
Sakamoto F, Katakami N, Kaneto H, Yasuda T, Takahara M, Miyashita K, et al. Association of serum YKL-40 levels with urinary albumin excretion rate in young Japanese patients with type 1 diabetes mellitus. Endocr J. 2013;60(1):73–9.
Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality: a collaborative meta-analysis of general population cohorts. Lancet. 2010;375(9731):2073–81.
Carter C, Katz R, Kramer H, de Boer IH, Kestenbaum BR, Peralta CA, et al. Influence of urine creatinine concentrations on the retention of albumin-creatinine ratio with cardiovascular disease events: the multi-ethnic study of atherosclerosis (MESA). Am J Kidney Dis. 2013;62(4):722–9.
Oh C-M, Park SK, Ryoo J-H. Serum uric acid level is associated with the development of microalbuminuria in Korean men. Eur J Clin Investig. 2013. https://doi.org/10.1111/eci.12180.
Liao L-N, Liu C-S, Li C-I, et al. Three-year incidence of elevated albuminuria and associated factors in a population-based cohort: the Taichung community health study. Eur J Prev Cardiol. 2014;22(6):788-97.
Prior SL, Clark AR, Jones DA, Bain SC, Hurel SJ, et al. Association of the PGC-1 α rs8192678 variant with microalbuminuria in subjects with type 2 diabetes mellitus. Dis Markers. 2012;32:363–9.
Mashima Y, Konta T, Suzuki K, Ikeda A, Ichikawa K, Shibata Y, et al. Polymorphism of proinflammatory cytokine genes and albuminuria in the Japanese general population: the Takahata study. Nephrol Dial Transplant. 2011;26(11):3902–7.
Matsuo S, Yasuda Y, Imai E. Current status of estimated glomerular filtration rate (eGFR) equations for Asians and an approach to create a common eGFR equation. Nephrology. 2010;15:45–8.
Matsushita K, Ballew SH, Astor BC, de Jong PE, Gansevoort RT, et al. Cohort profile: the chronic kidney disease prognosis consortium. Int J Epidemiol. 2013;42:1660–8.
Liu X, Gan X, Chen J. A new modified CKD-EPI equation for Chinese patients with type 2 diabetes. PLoS One. 2014;9(10)). https://doi.org/10.1371/journal.pone.0109743.
Horio M, Yasuda Y, Imai E. Ethnic factors of the glomerular filtration rate estimating equation. Kidney Int. 2012;81:799–801.
Teo BW, Xu H, Wang D, et al. GFR estimating equations in multiethnic Asian populations. Am J Kidney Dis. 2011;58:56–3.
Acknowledgements
Not applicable.
Funding
Research reported in this publication was supported by the National Institute of Minority Health and Health Disparities (NIMHD), of the National Institutes of Health under the award number U54MD008149, U54MD007584, and U54MD007601. The consent is solely the responsibility of the authors and does not necessarily represent the official view of NIMHD or NIH.
Availability of data and materials
NHANES data and material availability can be obtained from National Health and Nutrition Examination Survey (NHANES). Available at: https://www.cdc.gov/nchs/nhanes/index.htm Accessed June 30, 2017.
Author information
Authors and Affiliations
Contributions
All authors had access to the data and had a role in writing the manuscript. Research idea and study design: MKY, JD, CR, KG, VP; data acquisition: JD, KG; data analysis/interpretation: MKY, JD, CR, KG, VP; statistical analysis: JD, KG, CR, MKY; supervision or mentorship: CR, JD. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Formal ethics approval obtained from the University of Hawaii Office of Research Compliance Human Studies Program – Protocol #2018–00247. Data was de-identified.
Consent for publication
Not applicable.
Competing interests
No conflict of interest of any sponsorship or funding arrangements relating to the research of all authors. We confirm that we do not have any competing interests and have read the BioMed Central’s guidance on competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. Multivariable logistic regression models for urine albumin-to-creatinine ratios (ACR) ≥ 30 mg/g (A2) stratified by race/ethnicity. Table S2. Multivariable logistic regression models for urine albumin-to-creatinine ratios (ACR) > 300 mg/g (A3) stratified by race/ethnicity. Table S3. Multivariable logistic regression models for eGFR < 60 ml/min/1.73 m2 (G3a-G5) stratified by race/ethnicity. Table S4. Multivariable logistic regression models for eGFR < 45 ml/min/1.73 m2 (G3b-G5) stratified by race/ethnicity. (DOCX 18 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kataoka-Yahiro, M., Davis, J., Gandhi, K. et al. Asian Americans & chronic kidney disease in a nationally representative cohort. BMC Nephrol 20, 10 (2019). https://doi.org/10.1186/s12882-018-1145-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-018-1145-5