
Abstract
Background
Improved understanding of the molecular mechanisms involved in pediatric severe malarial anemia (SMA) pathogenesis is a crucial step in the design of novel therapeutics. Identification of host genetic susceptibility factors in immune regulatory genes offers an important tool for deciphering malaria pathogenesis. The IL-23/IL-17 immune pathway is important for both immunity and erythropoiesis via its effects through IL-23 receptors (IL-23R). However, the impact of IL-23R variants on SMA has not been fully elucidated.
Methods
Since variation within the coding region of IL-23R may influence the pathogenesis of SMA, the association between IL-23R rs1884444 (G/T), rs7530511 (C/T), and SMA (Hb < 6.0 g/dL) was examined in children (n = 369, aged 6–36 months) with P. falciparum malaria in a holoendemic P. falciparum transmission area.
Results
Logistic regression analysis, controlling for confounding factor of anemia, revealed that individual genotypes of IL-23R rs1884444 (G/T) [GT; OR = 1.34, 95% CI = 0.78–2.31, P = 0.304 and TT; OR = 2.02, 95% CI = 0.53–7.74, P = 0.286] and IL-23R rs7530511 (C/T) [CT; OR = 2.6, 95% CI = 0.59–11.86, P = 0.202 and TT; OR = 1.66, 95% CI = 0.84–3.27, P = 0.142] were not associated with susceptibility to SMA. However, carriage of IL-23R rs1884444T/rs7530511T (TT) haplotype, consisting of both mutant alleles, was associated with increased susceptibility to SMA (OR = 1.12, 95% CI = 1.07–4.19, P = 0.030).
Conclusion
Results presented here demonstrate that a haplotype of non-synonymous IL-23R variants increase susceptibility to SMA in children of a holoendemic P. falciparum transmission area.
Similar content being viewed by others


Background
One of the most prevalent parasitic infections in humans is Plasmodium falciparum malaria [1]. Based on the latest WHO estimates [2], there were 212 million cases of malaria worldwide in 2015 with 90% of the cases occurring in Africa. However, between 2000 and 2015, malaria incidence has declined by 22%. P. falciparum-related morbidity and mortality primarily occurs in immune-naïve infants and young children [3, 4]. Severe malaria presents with overlapping clinical sequelae that include severe malarial anemia (SMA), metabolic acidosis, respiratory distress, cerebral malaria (CM) and hypoglycemia [5]. In P. falciparum holoendemic transmission areas, such as Siaya County, western Kenya, severe malaria is a predominant cause of under-five morbidity and mortality [6], presenting primarily as SMA (Hb < 6.0 g/dL and any density parasitemia) [7, 8]. The pathophysiology of pediatric SMA is driven by a complex interaction between the human host and P. falciparum parasite. The etiological basis of SMA is multifactorial and includes lysis of both infected and uninfected erythrocytes [9–11], an imbalance in production of inflammatory mediators [12–14] that can promote bone marrow suppression and inhibition of erythropoiesis [15–17]. Moreover, we and others have previously demonstrated that SMA is exacerbated by HIV-1 and bacteremia co-infections [18–21].
Interleukin-23 receptor (IL-23R) engagement by IL-23 promotes T-helper 17 (Th17) cell-mediated inflammatory reactions [22, 23]. Th17 cells are pro-inflammatory CD4+ effector T-cells that mediate inflammatory process by secreting IL-17 [24]. Binding of IL-23 to IL-23R activates signal transduction via the Janus kinase (JAK)–signal transducer activator of transcription (STAT3/4), and NF-κB pathways [25]. IL-17 is produced by activated T-cells and is involved in priming of T-cells through its ability to stimulate macrophages and some epithelial cells to produce pro-inflammatory mediators [e.g., IL-1, IL-6, TNF-α, NOS-2, metalloproteases known to be important in inflammatory diseases [26, 27]. IL-17 is also important in linking immune responses with erythropoiesis through its ability to enhance proliferation of erythroid precursor cells [28–30]. Although IL-17 has not previously been explored during malaria mono-infection in the cohort of children investigated here, we have shown that IL-17 has a significant positive association with Hb in malaria-infected children with HIV-1 [31]. We have also shown that IL-17 is elevated in children with falciparum malaria and bacteremia co-infections [32], and that IL-23 is elevated in children with SMA [33]. Thus, the IL-23/IL-17 cytokine axis appears to be important in mediating the development of inflammatory reactions in children that develop SMA.
We and others have further shown that in polygenic infectious diseases such as malaria, pathogenesis is influenced by genetic variation in regulatory and/or coding regions of inflammatory mediators and conserved molecular pattern receptors [33–36]. As such, an improved understanding of SMA pathogenesis can be achieved through identification of polymorphisms in genes that mediate the development of severe disease. Although IL-23 receptor variation has not been explored in malaria, carriage of rs10889677CC in the IL-23R was associated with increased risk of cancer in Chinese populations [37]. Additional studies have provided evidence on the important role of the IL-23/Th17 axis on immune-mediated diseases such as Crohn’s disease (CD) [38], psoriasis [39, 40] and ankylosing spondylitis (AS) [41]. Collectively, these previous studies established that variations in IL-23R influence immune responses and thereby mediates the risk of inflammatory diseases. Even though these diseases present differently from malaria, they all elicit inflammatory reactions in the host. Despite its potential importance, the role of non-synonymous IL-23R polymorphisms has not been explored in the context of susceptibility to SMA. To address this gap-in-knowledge, we determined the association between the genotypic and haplotypic structures of non-synonymous IL-23R variants (i.e., rs1884444 G/T and rs7530511 C/T) and susceptibility to SMA.
Methods
Study site
The study was conducted at Siaya County Referral Hospital (SCRH), western Kenya, a region with holoendemic P. falciparum transmission [8]. The region is largely inhabited by the Luo ethnic tribe (~96%), therefore, providing a genetically homogenous population for the study. Falciparum malaria prevalence is ~83% in children aged <4 years, with severe disease manifests as SMA [7, 8]. Main mosquito vectors in this area are Anopheles gambiae s.s, Anopheles arabiensis and Anopheles funestus [42]. The residents receive between 100 and 300 infective mosquito bites per year [43] while intense malaria transmission occurs during April to August and also between November and January seasons [44].
Study participants
Children [n = 369, aged 6–36 months] of both sexes were recruited at SCRH during their first reported hospitalization for treatment of malaria. Recruitment followed a two-tier process of initial screening and enrollment i.e. the parent/guardian of the child received a detailed explanation of the study. Enrollment decisions were made after initial HIV-1 screening of the child and obtaining informed consent from the parent or legal guardian. Written informed consent was administered in the language of choice (i.e., English, Kiswahili or Dholuo). Children with acute malaria were stratified into two categories: non-severe malarial anemia (non-SMA)-defined as a positive smear for asexual P. falciparum parasitemia (of any density) and Hb ≥ 6.0 g/dL; and SMA - defined by a positive smear for asexual P. falciparum parasitemia (of any density) and Hb < 6.0 g/dL [45]. Children were excluded from the study for any one of the following reasons: children with CM (a rare occurrence in this holoendemic area) and clinical evidence of acute respiratory infection. All children were treated according to the Ministry of Health (MOH)-Kenya guidelines. These included the administration of oral artemether/lumefantrine (Coartem®) for uncomplicated malaria and intravenous quinine for severe malaria, and blood transfusion wherever indicated.
Sample collection
Venous blood samples (<3.0 mL) were collected in EDTA-containing vacutainer tubes at the time of enrollment, prior to provision of treatment or any supportive care. Blood samples were used for malaria diagnosis, hematological measurements, HIV testing, bacterial culture, and DNA isolation for genetic analyses.
Laboratory investigations
Hemoglobin levels and complete blood counts (CBC) were performed using the Beckman Coulter ACT diff2™ (Beckman-Counter Corporation, Miami, FL, USA). To determine parasite density, 10% Giemsa-stained thick blood smears were prepared and examined under a compound microscope on high-power magnification. P. falciparum parasites per 300 white blood cells (WBC) were determined and parasitemia (/μL) estimated using the total WBC count. To account for the most common causes of severe anemia in the region, anemia-promoting conditions such as HIV-1, bacteremia, sickle-cell trait (HbAS) status, alpha-thalassemia, and glucose-6-phosphate dehydrogenase deficiency (G6PD) were determined and controlled for during analyses. Pre- and post-test HIV counseling was provided for all participants. HIV-1 exposure was determined serologically (i.e., Unigold™ and Determine™), and HIV-1 infection was determined by proviral DNA PCR testing according to our previous methods [20]. Bacteremia was determined using the Wampole Isostat Pediatric 1.5 system (Wampole Laboratories), and blood was processed according to the manufacturer’s instructions. API biochemical galleries (bioMerieux, Inc.) and/or serology were used for identification of blood-borne bacterial isolates. G6PD deficiency was determined by a fluorescent spot test using the manufacturer’s methods (Trinity Biotech Plc., Bray, Ireland), while presence of the sickle cell trait (HbAS) was determined by cellulose acetate electrophoresis as per manufacturer’s conditions (Helena Bio-Sciences, Oxford, United Kingdom).
DNA isolation for genetic analyses
Blood spots were made on FTA Classic® cards (Whatman Inc., Clifton, NJ, USA), air dried and stored at room temperature until use. DNA was extracted using the Gentra System (Gentra System Inc., Minneapolis, MN, USA) according to the manufacturer’s protocol. The house-keeping gene; human glucose-3-phosphate dehydrogenase (hG3PDH) was used to confirm DNA presence. The genomic DNA (gDNA) was initially amplified using Genomiphi DNA Amplification Kit (Amershan Biosciences SV Corp, CA, USA) according manufacturer’s instructions to obtain more copies.
IL-23R rs1884444 G/T and rs7530511 C/T genotyping
The IL-23R rs1884444 G/T, (assay ID: C__11728603_10) and IL-23R rs7530511C/T (assay ID: C__2990018_10) polymorphisms were genotyped using the TaqMan® 5′ allelic discrimination Assay-By-Design high-throughput method based on the manufacturer’s instructions (Applied Biosystems, Foster City, CA, USA).
Data analyses
SPSS® statistical software package version 22.0 (IBM SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. Chi-square (χ2) analysis was used to examine differences between proportions. Mann-Whitney U test was used for comparisons of demographic and clinical characteristics between the clinical groups. Construction of haplotypes was performed using HPlus software program (Version 2.5). The association between genotypes and/or haplotypes and SMA was determined by logistic regression analysis, controlling for the confounding effects of age, sex, co-infections (HIV-1 and bacteremia), G6PD deficiency, HbAS and alpha-thalassemia status in the regression model at 95% confidence interval (CI) with statistical significance set at P ≤ 0.05.
Results
Clinical, demographic, and laboratory characteristics of the study participants
The clinical, demographic, and laboratory characteristics of the study participants are presented in Table 1. Parasitemic children (n = 369, aged 6–36 months) were categorized as non-SMA (n = 207) and SMA (n = 162). The distribution of sex was comparable between the clinical groups (P = 0.252). Children in the non-SMA group [median (IQR); 13.0 (7.8, 19.0)] were older than children in the SMA group [median (IQR); 9.6 (6.6, 16.3), P = 0.019]. Parasitemia levels were comparable between non-SMA [median (IQR); 14,711.7 (3257.4, 48,353.7)] and SMA [median (IQR); 15,656.6 (3258.0, 46,598.1), P = 0.760] groups. Axillary temperature at enrollment was also comparable between the groups; non-SMA [median (IQR); 37.6 (36.8, 38.6)]; and SMA [median (IQR); 37.9 (36.9, 38.5), P = 0.542], respectively. Children with SMA had an increased respiration rate (breaths/min) [median (IQR); 32.0 (28.0, 40.0)] relative to children with non-SMA [median (IQR); 30.0 (24.0, 40.0), P = 0.028]. As expected based on a priori grouping: Hb (g/dL) was lower in SMA [median (IQR); 5.0 (4.3, 5.5)] vs. non-SMA [median (IQR); 9.4 (8.1, 11.2), P < 0.001]; hematocrit (%) was lower in SMA [median (IQR); 16.1 (13.5, 17.8)] vs. non-SMA [median (IQR); 29.0 (24.8, 34.6), P < 0.001]; and RBC count (×1012/μL) was lower in SMA [median (IQR); 2.2 (1.9, 2.7)] vs. non-SMA [median (IQR); 4.2 (3.6, 4.9), P < 0.001]. Red cell distribution width (RDW, %) was higher in SMA [median (IQR); 22.9 (21.1, 25.8)] compared to children with non-SMA [median (IQR); 19.6 (16.5, 21.5), P < 0.001]. The SMA group also had elevated WBC counts (×103/μL) [median (IQR); 13.0 (9.2, 17.4)] relative to non-SMA group [median (IQR); 10.9 (9.0, 14.3)], P = 0.010], while platelet counts (×103/μL) were reduced in children with SMA [median (IQR); 147.5 (105.0, 200.5)] relative to the non-SMA group [median (IQR); 176.0 (122.0, 282.0), P < 0.001]. Considering confounding factors demonstrated that bacteremia was more common in children with SMA, 52 (53.1%) relative to non-SMA, 46 (46.9%), P = 0.350) while HIV-1 in SMA were 14 (60.9%) compared to non-SMA 9 (39.1%) P = 0.090. These distributions were, however, comparable between the two clinical groups. Analysis of the distribution of the genetic factors that have been shown to influence malaria outcome (sickle cell trait, G6PD and alpha thalassemia) also did not reveal any significant differences between the two groups. Sickle cell traits in SMA were 4 (80%) and in non-SMA 1 (20.0%), (P = 0.110) while that of G6PD in SMA were 6 (33.3%) and in non-SMA 12 (66.7%) (P = 0.310). Even though the proportions of alpha thalassemia were higher in SMA, 41 (53.9%) compared to non-SMA 35 (46.1%), (P = 0.070), they were not statistically different (Table 1).
Distribution of IL-23R rs1884444 G/T and IL-23R rs7530511 C/T genotypes in the clinical groups
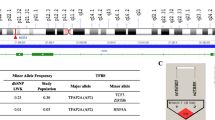
Prior to determination of the association between genotypes and SMA, distributions of the IL-23R rs1884444G/T and IL-23R rs7530511C/T genotypes were determined in the clinical categories. Chi-square (χ2) analyses showed that the distribution of the IL-23R rs1888444G/T and IL-23R rs7530511C/T genotypes were not different between the clinical groups (P = 0.278 and P = 0.386, respectively, Table 2). IL-23R rs1884444G/T genotypes within the non-SMA group were 70.5% GG, 26.6% GT and 2.9% TT, while those in the SMA group were 66.0% GG, 27.8% GT and 6.2% TT (Table 2). Genotypes of IL-23R rs1884444G/T in the non-SMA (χ2 = 0.087, P = 0.767) and SMA (χ2 = 2.901, P = 0.088) groups were consistent with Hardy-Weinberg Equilibrium (HWE). Allele frequencies of the IL-23R rs1884444G/T in the overall study population were 0.82 (G) and 0.18 (T), respectively (Table 2). In addition, the genotypic distribution of the IL-23R rs1884444G/T in the overall study population was consistent with HWE (χ2 = 2.21, P = 0.137).
The genotypic distribution of the IL-23R rs7530511C/T in non-SMA group was 84.5% CC, 12.6% CT, and 2.9% TT, while those in the SMA group were 79.0% CC, 17.3% CT and 3.7% TT (Table 2). In both non-SMA and SMA groups, there was deviation from HWE (χ2 = 12.98, P < 0.001 and χ2 = 6.57, P = 0.010), respectively. The major and the minor allele frequency for the IL-23R rs7530511C/T in the overall study population was 0.89 (C) and 0.11 (T), respectively (Table 2). In the overall study population, the IL-23R rs7530511C/T genotypic distribution showed deviation from HWE (χ2 = 18.81, P < 0.001).
Association between IL-23R rs1884444 G/T and IL-23R rs7530511 C/T genotypes and SMA
The association between individual genotypes of IL-23R rs1884444G/T and IL-23R rs7530511C/T and susceptibility to SMA was determined using logistic regression analysis, controlling for the confounding effects of age, sex, co-infection (HIV-1 status and bacteremia), HbAS, alpha-thalassemia and G6PD deficiency [46–48]. Relative to the wild-type IL-23R rs1884444 (GG), no significant associations with susceptibility to SMA were observed for either the GT (OR = 1.34, 95% CI = 0.78–2.31, P = 0.304) or TT (OR = 2.02, 95% CI = 0.53–7.74, P = 0.286) genotypes (Table 3). In addition, relative to the wild-type IL-23R rs7530511 (CC), neither the CT (OR = 2.60, 95% CI = 0.59–11.86, P = 0.202) nor the TT (OR = 1.66, 95% CI = 0.84–3.27, P = 0.142) were associated with susceptibility to SMA. Moreover, to provide a more global representation, we also included analysis based on the WHO cut-off of SMA (SMA; Hb < 5.0 g/dL and any density parasitemia). We however did not observe any significant association between the IL-23R rs1884444G/T and IL-23R rs7530511C/T genotypes and SMA in this study population (Table 3).
Association between IL-23R rs1884444 G/T and IL-23R rs7530511 C/T haplotypes and SMA
Using logistic regression analysis models, controlling for the confounding effects of age, sex, co-infection (HIV-1 status and bacteremia), HbAS, alpha-thalassemia, and G6PD deficiency [8, 46–49], we determined the association between carriage of the IL-23R rs1884444 and rs7530511 haplotype constructs and SMA. These analyses revealed that there was no association between carriage vs. non-carriage of the IL-23R rs1884444G/rs7530511C (GC) haplotype and SMA (OR = 0.49, 95% CI = 0.18–1.33, P = 0.161, Table 4). Susceptibility to SMA was also not influenced by carriage vs. non-carriage of either the GT (OR = 1.04, 95% CI = 0.33–3.31, P = 0.949) or TC (OR = 0.97, 95% CI = 0.52–1.81, P = 0.923) haplotypes (Table 4). However, carriage of the TT haplotype was associated with a significant increase in susceptibility to SMA (OR = 1.12, 95% CI = 1.07–4.19, P = 0.030, Table 4). Likewise, using the WHO cut-off for SMA, only the TT haplotype was associated with the risk of SMA (OR = 2.50, 95% CI = 1.18–5.29, P = 0.016, Table 4).
Discussion
In P. falciparum holoendemic transmission areas, one of the most common clinical outcomes of malaria is SMA. To further provide additional information on genes that condition susceptibility to SMA, we investigated the role of the IL-23/IL-17 cytokine pathway by determining the genetic association between non-synonymous mutations of IL-23R rs188444G/T and rs7560511C/T polymorphisms and susceptibility to SMA. The study showed that individual genotypes in IL-23R (rs188444G/T and rs7530511C/T) were not independently associated with susceptibility to SMA. However, carriage of the IL-23R rs188444T/rs7560511T (TT) haplotype was associated with increased susceptibility to SMA [using both modified (Hb < 6.0 g/dL) and WHO (Hb < 5.0 g/dL) definition of SMA].
The protein encoded by the IL-23R gene located on chromosome 1 is a subunit of the receptor for IL-23 sub-unit alpha (IL-23A) which pairs with the receptor molecule IL-12β1, both of which are required for IL-23A signaling [50]. The IL-23R/IL-12β1 dimer binds to IL-23, which is made up of a p19 protein and IL-12p40 sub-units [51]. In addition to its expression on memory T-cells, IL-23R is present on other immune cells, including activated antigen presenting cells (APCs), natural killer cells, and monocytes, all of which are involved in host-defense against invading pathogens [52–54]. Genetic variation in IL-23R plays an important role in determining the efficacy of cellular immune responses [55]. The current study demonstrates that genotypic variants of IL-23R [i.e., rs1884444 (G/T) and rs7530511 (C/T)] are not individually associated with susceptibility to SMA.
The IL-23R (rs188444 G/T) is located at codon 3 in exon 2 of the IL-23R and results in a histidine-to-glutamine substitution. This G to T change is known to be responsible for changes in the signal peptide of the IL-23R and results in exon skipping, alternative splicing, or malformation [55] resulting in alteration of the receptor-ligand binding specificity. Previous studies showed that IL-23R rs1884444 variation is associated with susceptibility to esophageal and gastric cancer, schistosomiasis-associated immune reconstitution inflammatory syndrome, and inflammatory bowel disease [56–58]. However, consistent with a study in Chinese adults with pulmonary tuberculosis (PTB) and drug-resistant PTB [59], we found no association in the current investigation between rs1884444 variants and malaria disease outcomes.
The IL-23R rs7530511 C/T polymorphism results in a replacement of proline for leucine at codon 310 (P310L). The rs7530511 C/T is located adjacent to the motif sequence, WQPWS, present in the membrane-transmembrane proximal IL-23R domain, and is capable of altering receptor affinity [60], a variation that can influence differential production of downstream molecules. Individual genotypes of rs7530511 in our population, however, did not show any independent associations with susceptibility to SMA, despite earlier observations that the rare TT genotype of the rs7530511 was associated with autoimmune conditions, such as Graves’ disease (GD) [60]. This could be explained by the autoimmune nature of GD which is thyroid gland specific while P. falciparum malaria that affects multiple organs.
Considering the fact that haplotypes within particular genes are often capable of exposing genetic combinations which can moderate or interact to produce effects that are not observable with individual genotypes [33, 61], we therefore constructed haplotypes of IL-23R rs1884444 G/T and rs7530511 (C/T). The current study revealed that the carriage of IL-23R rs1884444/rs7530511 (TT) haplotype was associated with an increased risk of SMA. This observation implies that carriage of both mutant genotypes (TT) is an important genetic risk factor for developing SMA once a child becomes infected with P. falciparum. Although presently undetermined, one can speculate that the TT haplotype may amplify exon skipping and/or mRNA splicing, resulting in altered affinity of the receptor for IL-23 (ligand) binding [55, 60]. Since IL-23/T-helper 17 axis leads to the production of IL-17, and other pro-inflammatory mediators, the TT haplotype may potentially inhibit the generation of pro-inflammatory mediators that aid in controlling malarial infections. However, the complex interplay between successfully controlling an infection and the generation of inflammatory-derived anemia during a malaria infection is difficult to discern at the molecular level [62]. IL-17 is a prototypical example of such complexity since IL-17 bridges immune and hematopoietic regulation by stimulating early stage erythroid progenitors (i.e., burst forming unit erythroid, BFU-E) [63], and in the opposite context, inhibits late stage erythroid progenitors [30, 64, 65]. Further studies are required to delineate the influence of genetic polymorphisms within IL-23R on differential expression and production of inflammatory mediators to unravel the molecular mechanisms through which the IL-23/T-helper 17 axis collectively influences the development of malarial disease outcomes.
Conclusion
In summary, the current study provides evidence that haplotypes of the IL-23R alter the risk of developing SMA in pediatric populations. We present data on a homogenous population consisting of ~96% Luo ethic group, a key characteristic in genetic studies of this nature. Furthermore, our study underscores the use of haplotype analysis approach in genetic association studies as it presents unique association not identifiable using individual allele or genotype analysis. We are currently investigating the impact of multi-haplotypes of IL-23R variants on longitudinal outcomes of malaria including mortality. In addition, due to the fact that polymorphisms may have distinct effects in different ethnic groups presenting with varied forms of severe malaria, studies across various ethnic groups are warranted to decipher fully the impact of IL-23R variation on susceptibility to severe malaria anemia.
Abbreviations
- APCs:
-
Antigen presenting cells
- BFU-E:
-
Burst forming unit erythroid
- CM:
-
Cerebral malaria
- G6PD:
-
Glucose-6-phosphate dehydrogenase
- Hb:
-
Hemoglobin
- HbAS:
-
Hemoglobin AS type
- HDP:
-
High density parasitemia
- HWE:
-
Hardy Weinberg Equilibrium
- IL-23R:
-
Interleukin −23 receptor
- IQR:
-
Interquartile range
- MOH:
-
Ministry of Health
- NF-κB:
-
Nuclear factor kappa-light-chain-enhancer of B cells
- SMA:
-
Severe malarial anemia
- SNP:
-
Single nucleotide polymorphisms
- WBCs:
-
White blood cells
References
WHO. Severe falciparum malaria. World Health Organization communicable diseases cluster. Trans R Soc Trop Med Hyg. 2000;94(Suppl. 1):S1–9.
WHO: World Health Organization. Malaria Report. ISBN 978-92-4-151171. 2016.
Giha HA, Elghazali G, A-Elgadir TM, A-Elbasit IE, Eltahir EM, Baraka OZ, Khier MM, Adam I, Troye-Blomberg M, Theander TG, et al. Clinical pattern of severe plasmodium falciparum malaria in Sudan in an area characterized by seasonal and unstable malaria transmission. Trans R Soc Trop Med Hyg. 2005;99(4):243–51.
Marsh K, Forster D, Waruiru C, Mwangi I, Winstanley M, Marsh V, Newton C, Winstanley P, Warn P, Peshu N, et al. Indicators of life-threatening malaria in African children. N Engl J Med. 1995;332(21):1399–404.
Rowe JA, Opi DH, Williams TN. Blood groups and malaria: fresh insights into pathogenesis and identification of targets for intervention. Curr Opin Hematol. 2009;16(6):480–7.
Amek NO, Odhiambo FO, Khagayi S, Moige H, Orwa G, Hamel MJ, Van Eijk A, Vulule J, Slutsker L, Laserson KF. Childhood cause-specific mortality in rural western Kenya: application of the inter VA-4 model. Glob Health Action. 2014;7:25581.
Obonyo CO, Vulule J, Akhwale WS, Grobbee DE. In-hospital morbidity and mortality due to severe malarial anemia in western Kenya. Am J Trop Med Hyg. 2007;77(6 Suppl):23–8.
Ong’echa JM, Keller CC, Were T, Ouma C, Otieno RO, Landis-Lewis Z, Ochiel D, Slingluff JL, Mogere S, Ogonji GA, et al. Parasitemia, anemia, and malarial anemia in infants and young children in a rural holoendemic Plasmodium falciparum transmission area. Am J Trop Med Hyg. 2006;74(3):376–85.
Dondorp AM, Angus BJ, Chotivanich K, Silamut K, Ruangveerayuth R, Hardeman MR, Kager PA, Vreeken J, White NJ. Red blood cell deformability as a predictor of anemia in severe falciparum malaria. Am J Trop Med Hyg. 1999;60(5):733–7.
Egan AF, Fabucci ME, Saul A, Kaslow DC, Miller LH. Aotus new World monkeys: model for studying malaria-induced anemia. Blood. 2002;99(10):3863–6.
Price RN, Simpson JA, Nosten F, Luxemburger C, Hkirjaroen L, ter Kuile F, Chongsuphajaisiddhi T, White NJ. Factors contributing to anemia after uncomplicated falciparum malaria. Am J Trop Med Hyg. 2001;65(5):614–22.
Kurtzhals JA, Akanmori BD, Goka BQ, Adabayeri V, Nkrumah FK, Behr C, Hviid L. The cytokine balance in severe malarial anemia. J Infect Dis. 1999;180(5):1753–5.
McDevitt MA, Xie J, Gordeuk V, Bucala R. The anemia of malaria infection: role of inflammatory cytokines. Curr Hematol Rep. 2004;3(2):97–106.
Prakash D, Fesel C, Jain R, Cazenave PA, Mishra GC, Pied S. Clusters of cytokines determine malaria severity in Plasmodium falciparum-infected patients from endemic areas of Central India. J Infect Dis. 2006;194(2):198–207.
Abdalla S, Weatherall DJ, Wickramasinghe SN, Hughes M. The anaemia of P. falciparum malaria. Br J Haematol. 1980;46(2):171–83.
Dormer P, Dietrich M, Kern P, Horstmann RD. Ineffective erythropoiesis in acute human P. falciparum malaria. Blutalkohol. 1983;46(5):279–88.
Phillips RE, Looareesuwan S, Warrell DA, Lee SH, Karbwang J, Warrell MJ, White NJ, Swasdichai C, Weatherall DJ. The importance of anaemia in cerebral and uncomplicated falciparum malaria: role of complications, dyserythropoiesis and iron sequestration. Q J Med. 1986;58(227):305–23.
Bassat Q, Guinovart C, Sigauque B, Mandomando I, Aide P, Sacarlal J, Nhampossa T, Bardaji A, Morais L, Machevo S, et al. Severe malaria and concomitant bacteraemia in children admitted to a rural Mozambican hospital. Tropical Med Int Health. 2009;14(9):1011–9.
Berkley JA, Lowe BS, Mwangi I, Williams T, Bauni E, Mwarumba S, Ngetsa C, Slack MP, Njenga S, Hart CA, et al. Bacteremia among children admitted to a rural hospital in Kenya. N Engl J Med. 2005;352(1):39–47.
Otieno RO, Ouma C, Ong’echa JM, Keller CC, Were T, Waindi EN, Michaels MG, Day RD, Vulule JM, Perkins DJ. Increased severe anemia in HIV-1-exposed and HIV-1-positive infants and children during acute malaria. AIDS. 2006;20(2):275–80.
Were T, Davenport GC, Hittner JB, Ouma C, Vulule JM, Ong’echa JM, Perkins DJ. Bacteremia in Kenyan children presenting with malaria. J Clin Microbiol. 2010;49(2):671–6.
Chen Z, Laurence A, O’Shea JJ. Signal transduction pathways and transcriptional regulation in the control of Th17 differentiation. Semin Immunol. 2007;19(6):400–8.
Volpe E, Servant N, Zollinger R, Bogiatzi SI, Hupe P, Barillot E, Soumelis V. A critical function for transforming growth factor-beta, interleukin 23 and proinflammatory cytokines in driving and modulating human T(H)-17 responses. Nat Immunol. 2008;9(6):650–7.
Onishi RM, Gaffen SL. Interleukin-17 and its target genes: mechanisms of interleukin-17 function in disease. Immunology. 2010;129(3):311–21.
Cho ML, Kang JW, Moon YM, Nam HJ, Jhun JY, Heo SB, Jin HT, Min SY, Ju JH, Park KS, et al. STAT3 and NF-kappaB signal pathway is required for IL-23-mediated IL-17 production in spontaneous arthritis animal model IL-1 receptor antagonist-deficient mice. J Immunol. 2006;176(9):5652–61.
Kolls JK, Linden A. Interleukin-17 family members and inflammation. Immunity. 2004;21(4):467–76.
Nakae S, Saijo S, Horai R, Sudo K, Mori S, Iwakura Y. IL-17 production from activated T cells is required for the spontaneous development of destructive arthritis in mice deficient in IL-1 receptor antagonist. Proc Natl Acad Sci U S A. 2003;100(10):5986–90.
Jovcic G, Bugarski D, Krstic A, Vlaski M, Petakov M, Mojsilovic S, Stojanovic N, Milenkovic P. The effect of interleukin-17 on hematopoietic cells and cytokine release in mouse spleen. Physiol Res. 2007;56(3):331–9.
Jovcic G, Bugarski D, Petakov M, Krstic A, Vlaski M, Stojanovic N, Milenkovic P. In vivo effects of interleukin-17 on haematopoietic cells and cytokine release in normal mice. Cell Prolif. 2004;37(6):401–12.
Jovcic G, Bugarski D, Petakov M, Stankovic J, Stojanovic N, Milenkovic P. Effect of IL-17 on in vitro hematopoietic progenitor cells growth and cytokine release in normal and post-irradiated murine bone marrow. Growth Factors. 2001;19(1):61–71.
Davenport GC, Hittner JB, Were T, Ong’echa JM, Perkins DJ. Relationship between inflammatory mediator patterns and anemia in HIV-1 positive and exposed children with Plasmodium falciparum malaria. Am J Hematol. 2012;87(7):652–8.
Davenport GC, Hittner JB, Otieno V, Karim Z, Mukundan H, Fenimore PW, Hengartner NW, McMahon BH, Kempaiah P, Ong’echa JM, et al. Reduced parasite burden in children with Falciparum malaria and Bacteremia Coinfections: role of mediators of inflammation. Mediat Inflamm. 2016;2016:4286576.
Ong’echa JM, Remo AM, Kristoff J, Hittner JB, Were T, Ouma C, Otieno RO, Vulule JM, Keller CC, Awandare GA, et al. Increased circulating interleukin (IL)-23 in children with malarial anemia: in vivo and in vitro relationship with co-regulatory cytokines IL-12 and IL-10. Clin Immunol. 2008;126(2):211–21.
Hobbs MR, Udhayakumar V, Levesque MC, Booth J, Roberts JM, Tkachuk AN, Pole A, Coon H, Kariuki S, Nahlen BL, et al. A new NOS2 promoter polymorphism associated with increased nitric oxide production and protection from severe malaria in Tanzanian and Kenyan children. Lancet. 2002;360(9344):1468–75.
Munde EO, Okeyo WA, Anyona SB, Raballah E, Konah S, Okumu W, Ogonda L, Vulule J, Ouma C. Polymorphisms in the Fc gamma receptor IIIA and toll-like receptor 9 are associated with protection against severe malarial anemia and changes in circulating gamma interferon levels. Infect Immun. 2012;80(12):4435–43.
Tishkoff SA, Williams SM. Genetic analysis of African populations: human evolution and complex disease. Nat Rev Genet. 2002;3(8):611–21.
Zheng J, Jiang L, Zhang L, Yang L, Deng J, You Y, Li N, Wu H, Li W, Lu J, et al. Functional genetic variations in the IL-23 receptor gene are associated with risk of breast, lung and nasopharyngeal cancer in Chinese populations. Carcinogenesis. 2012;33(12):2409–16.
Duerr RH, Taylor KD, Brant SR, Rioux JD, Silverberg MS, Daly MJ, Steinhart AH, Abraham C, Regueiro M, Griffiths A, et al. A genome-wide association study identifies IL23R as an inflammatory bowel disease gene. Science. 2006;314(5804):1461–3.
Capon F, Di Meglio P, Szaub J, Prescott NJ, Dunster C, Baumber L, Timms K, Gutin A, Abkevic V, Burden AD, et al. Sequence variants in the genes for the interleukin-23 receptor (IL23R) and its ligand (IL12B) confer protection against psoriasis. Hum Genet. 2007;122(2):201–6.
Cargill M, Schrodi SJ, Chang M, Garcia VE, Brandon R, Callis KP, Matsunami N, Ardlie KG, Civello D, Catanese JJ, et al. A large-scale genetic association study confirms IL12B and leads to the identification of IL23R as psoriasis-risk genes. Am J Hum Genet. 2007;80(2):273–90.
Rueda B, Orozco G, Raya E, Fernandez-Sueiro JL, Mulero J, Blanco FJ, Vilches C, Gonzalez-Gay MA, Martin J. The IL23R Arg381Gln non-synonymous polymorphism confers susceptibility to ankylosing spondylitis. Ann Rheum Dis. 2008;67(10):1451–4.
Beach RF, Ruebush 2nd TK, Sexton JD, Bright PL, Hightower AW, Breman JG, Mount DL, Oloo AJ. Effectiveness of permethrin-impregnated bed nets and curtains for malaria control in a holoendemic area of western Kenya. Am J Trop Med Hyg. 1993;49(3):290–300.
Bloland PB, Ruebush TK, McCormick JB, Ayisi J, Boriga DA, Oloo AJ, Beach R, Hawley W, Lal A, Nahlen B, et al. Longitudinal cohort study of the epidemiology of malaria infections in an area of intense malaria transmission I. Description of study site, general methodology, and study population. AmJTrop Med Hyg. 1999;60(4):635–40.
Beier JC, Oster CN, Onyango FK, Bales JD, Sherwood JA, Perkins PV, Chumo DK, Koech DV, Whitmire RE, Roberts CR, et al. Plasmodium falciparum incidence relative to entomologic inoculation rates at a site proposed for testing malaria vaccines in western Kenya. Am J Trop Med Hyg. 1994;50(5):529–36.
McElroy PD, Lal AA, Hawley WA, Bloland PB, Kuile FO, Oloo AJ, Harlow SD, Lin X, Nahlen BL. Analysis of repeated hemoglobin measures in full-term, normal birth weight Kenyan children between birth and 4 years of age. III. The Asemobo Bay cohort project. Am J Trop Med Hyg. 1999;61(6):932–40.
Aidoo M, Terlouw DJ, Kolczak MS, McElroy PD, ter Kuile FO, Kariuki S, Nahlen BL, Lal AA, Udhayakumar V. Protective effects of the sickle cell gene against malaria morbidity and mortality. Lancet. 2002;359(9314):1311–2.
Wambua S, Mwacharo J, Uyoga S, Macharia A, Williams TN. Co-inheritance of alpha+−thalassaemia and sickle trait results in specific effects on haematological parameters. Br J Haematol. 2006;133(2):206–9.
Wambua S, Mwangi TW, Kortok M, Uyoga SM, Macharia AW, Mwacharo JK, Weatherall DJ, Snow RW, Marsh K, Williams TN. The effect of alpha+−thalassaemia on the incidence of malaria and other diseases in children living on the coast of Kenya. Plos Med. 2006;3(5):e158.
Were T, Davenport GC, Hittner JB, Ouma C, Vulule JM, Ong’echa JM, Perkins DJ. Bacteremia in Kenyan children presenting with malaria. J Clin Microbiol. 2011;49(2):671–6.
Parham C, Chirica M, Timans J, Vaisberg E, Travis M, Cheung J, Pflanz S, Zhang R, Singh KP, Vega F, et al. A receptor for the heterodimeric cytokine IL-23 is composed of IL-12Rbeta1 and a novel cytokine receptor subunit, IL-23R. J Immunol. 2002;168(11):5699–708.
Oppmann B, Lesley R, Blom B, Timans JC, Xu Y, Hunte B, Vega F, Yu N, Wang J, Singh K, et al. Novel p19 protein engages IL-12p40 to form a cytokine, IL-23, with biological activities similar as well as distinct from IL-12. Immunity. 2000;13(5):715–25.
Bailey SL, Schreiner B, McMahon EJ, Miller SD. CNS myeloid DCs presenting endogenous myelin peptides ‘preferentially’ polarize CD4+ T(H)-17 cells in relapsing EAE. Nat Immunol. 2007;8(2):172–80.
Cheung PF, Wong CK, Lam CW. Molecular mechanisms of cytokine and chemokine release from eosinophils activated by IL-17A, IL-17F, and IL-23: implication for Th17 lymphocytes-mediated allergic inflammation. J Immunol. 2008;180(8):5625–35.
Schmidt-Weber CB, Akdis M, Akdis CA. TH17 cells in the big picture of immunology. J Allergy Clin Immunol. 2007;120(2):247–54.
Kan SH, Mancini G, Gallagher G. Identification and characterization of multiple splice forms of the human interleukin-23 receptor alpha chain in mitogen-activated leukocytes. Genes Immun. 2008;9(7):631–9.
Chen J, Lu Y, Zhang H, Ding Y, Ren C, Hua Z, Zhou Y, Deng B, Jin G, Hu Z, et al. A nonsynonymous polymorphism in IL23R gene is associated with risk of gastric cancer in a Chinese population. Mol Carcinog. 2010;49(10):862–8.
Chu H, Cao W, Chen W, Pan S, Xiao Y, Liu Y, Gu H, Guo W, Xu L, Hu Z, et al. Potentially functional polymorphisms in IL-23 receptor and risk of esophageal cancer in a Chinese population. Int J Cancer. 2012;130(5):1093–7.
Ogola GO, Ouma C, Jura WG, Muok EO, Colebunders R, Mwinzi PN. A non-synonymous polymorphism in IL-23R Gene (rs1884444) is associated with reduced risk to schistosomiasis-associated immune reconstitution inflammatory syndrome in a Kenyan population. BMC Infect Dis. 2014;14:316.
Jiang D, Hu X, Li S, Julaiti A, Xia Y, Wang J, Wushouer Q. Polymorphisms of IL-23 receptor gene are associated with susceptibility to pulmonary tuberculosis and drug-resistant pulmonary tuberculosis. Zhonghua Yi Xue Za Zhi. 2015;95(20):1576–80.
Huber AK, Jacobson EM, Jazdzewski K, Concepcion ES, Tomer Y. Interleukin (IL)-23 receptor is a major susceptibility gene for graves’ ophthalmopathy: the IL-23/T-helper 17 axis extends to thyroid autoimmunity. J Clin Endocrinol Metab. 2008;93(3):1077–81.
Wilson JN, Rockett K, Jallow M, Pinder M, Sisay-Joof F, Newport M, Newton J, Kwiatkowski D. Analysis of IL10 haplotypic associations with severe malaria. Genes Immun. 2005;6(6):462–6.
Chen Q, Schlichtherle M, Wahlgren M. Molecular aspects of severe malaria. Clin Microbiol Rev. 2000;13(3):439–50.
Krstic A, Mojsilovic S, Jovcic G, Bugarski D. The potential of interleukin-17 to mediate hematopoietic response. Immunol Res. 2012;52(1–2):34–41.
Bugarski D, Jovcic G, Katic-Radivojevic S, Petakov M, Krstic A, Stojanovic N, Milenkovic P. Hematopoietic changes and altered reactivity to IL-17 in Syphacia obvelata-infected mice. Parasitol Int. 2006;55(2):91–7.
Bugarski D, Krstic A, Vlaski M, Petakov M, Jovcic G, Stojanovic N, Milenkovic P. Interleukine-17-induced inhibitory effect on late stage murine erythroid bone marrow progenitors. Eur Cytokine Netw. 2004;15(3):247–54.
Acknowledgements
We are grateful to the Siaya County Referral Hospital for clinical support. We are indebted to the parents/guardians of the study participants and children who took part in the study.
Funding
This work was supported by grants from the National Institute of Health [(7R01-TW008306–05-CO) and TW05884–05 (DJP)].
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its Additional file 1].
Authors’ contributions
EOM, ER, WAO, JMO, DJP and CO designed, carried out the study in the rural population and participated in the drafting of the manuscript. EOM, WAO, and ER performed the statistical analyses and participated in the drafting of the manuscript. All authors read and approved the final manuscript.
Competing interests
All authors have declared no competing interests in the submitted work.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The study was approved by the Scientific and Ethics Review Committee of the Kenya Medical Research Institute and the University of New Mexico IRB. Informed written consent was obtained from the parent or legal guardian of all children participating in the study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
These are details of the raw data for the study participants (N = 369) used in the analyses of results presented in the current paper. (XLS 384 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Munde, E.O., Raballah, E., Okeyo, W.A. et al. Haplotype of non-synonymous mutations within IL-23R is associated with susceptibility to severe malaria anemia in a P. falciparum holoendemic transmission area of Kenya. BMC Infect Dis 17, 291 (2017). https://doi.org/10.1186/s12879-017-2404-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-017-2404-y