
Abstract
Background
Age, obesity, and metabolic syndrome are known risk factors for gallstones; however, the combined impact of these different risk factors on gallstone formation has not yet been examined.
Methods
This retrospective, cross-sectional study involved 3190 participants, including 207 participants (6.5%) with gallstones and 986 (30.9%) with metabolic syndrome. Participants were divided into four phenotypes according to metabolic syndrome and obesity status: 1378 participants were metabolically healthy and non-obese (MHNO); 826 were metabolically healthy but obese (MHO); 185 were metabolically abnormal but not obese (MANO); and 801 participants were metabolically abnormal and obese (MAO).
Results
The MAO and MANO phenotypes had more gallstones than the MHO and MHNO phenotypes, regardless of age (< 50 or ≥ 50 years old). Multivariate analyses showed that phenotype was an independent risk factor for gallstones in participants < 50 years old (odds ratio (OR) = 1.73, 95% confidence interval (CI) = 1.32–2.28). Younger participants also had a higher risk of gallstones in the MAO (OR = 5.41, 95% CI = 2.31–12.66), MANO (OR = 3.18, 95% CI = 0.86–11.75), and MHO (OR = 2.17, 95% CI = 0.90–5.22) phenotypes than the MHNO phenotype.
Conclusions
Our retrospective results demonstrate an increased association of gallstones in younger people (< 50 years old) with metabolic syndrome and obesity.
Similar content being viewed by others


Background
Gallstones and their associated complications are common conditions worldwide. Approximately 6–20% of the population has gallstones and some studies have indicated rates of screen-detected gallstones between 0.6 and 1.39% per year in Taiwan and Europe [1,2,3]. Moreover, specific groups, such as those with cirrhosis and Type 2 diabetes mellitus (DM), have gallstone incidence rates of 2–5% per year [4]. More than 20% of people with gallstones develop biliary colic or gallstone-associated complications, including acute pancreatitis, cholangitis, cholecystitis, and common bile duct stones [5].
Several studies have shown that age, sex, body mass index (BMI), non-alcoholic fatty liver, Type 2 DM, and insulin resistance are associated with gallstones [6,7,8]. Furthermore, people with greater incidence of metabolic abnormality have a higher risk of developing gallstones [9]. BMI and obesity also increase risk of gallstone development [10, 11]. Because obese individuals with different metabolic profiles can present with distinct cardiovascular or diabetes outcomes, many investigators have developed obesity sub-types, using metabolic factors, as four phenotypes: metabolically-healthy and non-obese (MHNO), metabolically-healthy but obese (MHO), metabolically-abnormal but not obese (MANO) and metabolically-abnormal and obese (MAO) [12, 13]. The studies found that the MAO phenotype has the highest risk of cardiovascular disease, chronic kidney disease (CKD), and advanced colorectal neoplasia compared to MHO or MANO individuals [14,15,16]. However, the association between gallstones and these four phenotypes is still unknown. Age is also a major risk factor that is positively correlated with gallstone development. However, it is not known whether these risk factors contribute equally in younger and older populations. Our study aimed to analyze the impact of risk factors including age, metabolic syndrome, and obesity on gallstone formation.
Methods
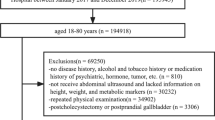
This retrospective, cross-sectional study included patients who received voluntary physical check-ups from the Health Examination Center of Changhua Christian Hospital, Changhua City, Taiwan between 2010 and 2014. A total of 4456 participants were initially enrolled in this study; however, 774 were excluded because:
-
51 had incomplete data to define their metabolic syndrome;
-
415 underwent repeat examination during the study period;
-
257 refused to undergo abdominal ultrasound;
-
491 had incomplete data for hepatitis B or C; and
-
51 had already undergone cholecystectomy.
In the end, 3190 participants were eligible for further analysis. All participants in the final group received blood tests (including glucose, glycated hemoglobin (HbA1c), cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides, hepatitis B surface antigen, and anti-hepatitis C virus antibody), blood pressure measurement, waist circumference measurements, and abdominal sonography. The Ethics Committee of Changhua Christian Hospital approved the study protocol used in this work (CCH IRB No: 150807).
A gallstone was defined as a hyperechoic area with a typical acoustic shadow and positional change by sonography and was diagnosed by an experienced gastroenterologist who has more than 5-years of experience and was unaware of personal history or laboratory data. Cholecystectomy was defined as an invisible gallbladder can be identified by sonography or by a personal history of cholecystectomy. Metabolic syndrome was defined as fulfilling at least three of the five Adult Treatment Panel III criteria: (1) central obesity, defined as a waist circumference of ≥90 cm in Asian men and ≥ 80 cm in Asian women; (2) low HDL-C levels, defined as fasting HDL-C < 40 mg/dL in men and < 50 mg/dL in women; (3) hypertension, defined as systolic pressure ≥ 130 mmHg and/or diastolic ≥85 mmHg, or in patients with a history of hypertension receiving antihypertensive therapy; (4) high triglyceridemia, defined as fasting triglyceride levels ≥150 mg/dL; and (5) hyperglycemia, defined as fasting glucose level ≥ 100 mg/dL, or in patients with a history of diabetes receiving medications to control elevated glucose [17]. Obesity was defined as BMI ≥ 25 kg/cm2 in the study by using the classification for adult Asians proposed by WHO in 2000 [18].
Participants were further divided into four phenotypes according to metabolic syndrome and obesity profile: MHNO included participants without both metabolic syndrome and obesity; MHO included those without metabolic syndrome but with obesity; MANO included participants with metabolic syndrome but without obesity; and MAO included those who had metabolic syndrome combined with obesity.
Statistical analyses
Continuous variables are presented as mean ± standard deviation and were compared using an ANOVA test. Categorical data were compared using a chi-square test. Single-variable, binary logistic regression and non-parsimonious multivariable logistic regression analysis were used to analyze the significance of variables in gallstones. Statistical analyses were performed using PASW Statistics version 18 (formerly SPSS; IBM, Hong Kong). P < 0.05 (two-tailed) was considered statistically significant.
Results
Baseline characteristics
There were 3190 participants enrolled for the final analysis, including 207 participants (6.5%) with gallstones and 986 (30.9%) with metabolic syndrome. The numbers and rates of participants in each phenotype were 1633 (51.2%) for the MHNO phenotype, 571 (17.9%) for the MHO phenotype, 292 (9.2%) for the MANO phenotype, and 694 (21.8%) for the MAO phenotype. Participants in the MAO and the MANO phenotypes were older and had higher blood pressure and more abnormal levels of blood glucose, liver function tests (aspartate transaminase, alanine transaminase, alkaline phosphatase, and gamma-glutamyl transferase, except bilirubin), lipid profiles, uric acid, and renal function (blood urea nitrogen and creatinine) compared to those in the MHNO and MHO phenotypes. Detailed results are listed in Table 1 (Additional file 1: Table S1).
A total of 98 (10%) participants with metabolic syndrome had gallstones but only 109 (5%) had gallstones among those without metabolic syndrome. Age, HCV infection and four phenotypes were the risk factors for gallstones after non-parsimonious multivariable logistic regression (Additional file 2: Table S2). The median age in the study was 50 years old and the interaction effect is statistically significant in subgroups divided by age below and above 50. Table 2 shows higher rates of gallstones in both the MAO and MANO phenotypes compared to the MHO and MHNO phenotypes, regardless of age (< 50 or ≥ 50 years old). The rate of gallstones was similar in younger participants (< 50 years old) in the MAO phenotype compared to older participants (≥50 years old) in the MHNO phenotype (7.2% vs. 6.8%; P = 0.837).
As shown in Table 3, we used univariate and multivariate regression analysis to determine the risk factors for gallstones in two the different groups divided by age. The results revealed that the four phenotypes— according to metabolic syndrome and obesity profile— were the only independent risk factors for gallstones in participants younger than 50 years old (odds ratio (OR) = 1.73, 95% confidence interval (CI) = 1.32–2.28; P < 0.001). However, in participants older than 50, only HCV infection was a significant independent factor for gallstones (OR = 2.58, 95% CI = 1.43–4.68; P < 0.05). Subgroup analyses were performed after multivariate regression to identify effects in each group of participants. The results are listed in Table 4. When MHNO was used as a reference, the ORs in each phenotype of participants (< 50 years old) were MHO (OR = 2.17, 95% CI = 0.86–11.75; P = 0.08), MANO (OR = 3.18, 95% CI = 0.86–11.75; P = 0.08) and MAO (OR = 5.41, 95% CI = 2.31–12.66; P < 0.001). No statistically significant differences were found between MHNO, MHO and MAO phenotypes (≥50 years old).
Discussion
Many studies have shown that several independent factors are associated with gallstone development, including age, sex, metabolic syndromes, obesity, Type 2 DM, BMI, HCV, and CKD [2, 5, 19]. While age is a very strong risk factor for gallstones, it is unknown whether these risk factors contribute differently toward gallstone formation in younger people. This study is the first to analyze these risk factors for gallstones according to different age groups in an Asian population. Our results showed that the combination of metabolic syndrome and obesity posed the greatest likelihood of gallstone formation in people younger than 50 years old. However, in people older than 50, HCV was the major associated factor for gallstone formation.
Metabolic syndrome and obesity are two of the main risk factors for gallstones and the prevalence of gallstones is higher in individuals with a greater number of abnormal metabolic factors [3, 6, 9, 20]. Some studies have shown waist circumference, HDL, and blood glucose as major factors for gallstone formation [3, 20]. The same was also noted for obesity; high BMI was associated with prevalence of gallstones [10, 11]. However, it is unclear whether both metabolic syndrome and obesity, or only one of these factors, contributes to the high prevalence of gallstones. Many studies have attempted to classify four different phenotypes—MAO, MANO, MHO, and MHNO—according to obesity and metabolic health status [21,22,23,24]. Risk of diabetes, cardiovascular disease, and CKD remained inconclusive in the MHO phenotype. Hashimoto et al. showed that the MHO phenotype had a similar risk of CKD compared with the MHNO phenotype [16]. Luo et al. showed no increased risk of diabetes or cardiovascular disease in the MHO phenotype. Moreover, there was no significant difference in the risk of advanced colorectal neoplasia between the MHO and MHNO but MANO and MAO are increased risk of metachronous colorectal neoplasia in a study by Kim et al. [14] In contrast, Ryoo et al. concluded that the MHO phenotype had an increased risk of diabetes according to the degree of obesity [25]. In addition to age, the levels of serum uric acid, liver function tests, and renal function significantly differed amongst the four groups, being more abnormal in MAO and MANO than MHO and MHNO in our study. However, after adjusting all these factors by multivariate regression, only age, HCV infection and the four phenotypes were independent factors associated with gallstones. We also found that the MAO phenotype had a higher prevalence (7.2%) and odds ratio (5.41) for gallstones than the other three phenotypes (prevalence 2.2–4.8%; OR: 2.17–3.78) in people younger than 50.
Many studies have reported age as a major risk factor for gallstones [8, 26,27,28]. In addition, the elderly population has been shown to have a higher rate of gallstone-associated complications, such as cholecystitis and gallstone pancreatitis, and a higher rate of surgical complications after cholecystectomy [29, 30]. A study by Li et al. revealed HCV to be a substantial risk factor for gallstones in populations older than 60 (adjusted OR: 2.394 (1.066–5.375)) [31]. We found a similar result in our study: in the older groups (≥50 years old), HCV infection was the only significant risk factor for gallstones. However, this effect was not seen in the younger group (< 50 years old). The prevalence of gallstones in younger participants (< 50 years old) with both metabolic syndrome and obesity was similar to that observed in metabolically healthy and non-obese older participants (≥50 years old) (7.2% vs. 6.8%; P = 0.837). Therefore, the effect of metabolic syndrome and obesity on gallstones in younger participants was similar to the effect of age on gallstones in older participants without metabolic syndrome and obesity. The HCV infection rate was lower in the younger population, with the prevalence of both metabolic syndrome and obesity in young adults increasing gradually in Taiwan. HCV may also have a close association with insulin resistance and hepatic steatosis [32, 33]. All these factors (HCV infection, insulin resistance, or hepatic steatosis) were positively correlated with gallstones [31, 34]. Whether the relationship between HCV and metabolic syndrome has a synergistic effect or a causal relationship on gallstone formation requires further study [35]. Our study also showed that the effect of metabolic syndrome and obesity on gallstones was stronger in younger participants. The effect would be decreased in older participants because they had more interactive effects with factors that were also associated with gallstones, such as Type 2 DM, HCV, and CKD.
Although more than 3000 participants were included in the study, there were still several limitations. Firstly, we did not distinguish between the types of gallstones included (cholesterol or pigment stones) because we used sonographic findings. Secondly, this was a cross-sectional, retrospective study; the incident rate of gallstones in different age groups with metabolic syndrome and obesity needs to be confirmed using longitudinal studies. Thirdly, the study lacked some published data that is currently available in the literature regarding other risk factors of gallstones, such as smoking, drinking alcohol, exercise and lifestyle, pregnancy, oral contraceptive use, or family history. Fourth, the study groups were from an Asian population in Taiwan; the incidences of viral hepatitis B or C infection and definitions of obesity differ between the Eastern and Western worlds. Further studies are needed using data from different races for comparison with the current results.
Conclusions
In conclusion, the present study has shown an increased association of gallstones in younger people with metabolic syndrome and obesity. The prevalence of gallstones in younger people with metabolic abnormality and obesity was equal to that of metabolically-healthy and non-obese elderly people. Diet and exercise intervention may be beneficial for high-risk groups to prevent gallstone formation; however, additional studies are required to confirm these findings.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALP:
-
Alkaline phosphatase
- ALT:
-
Alanine transaminase
- AST:
-
Aspartate transaminase
- BMI:
-
Body mass index
- BUN:
-
Blood urea nitrogen
- CKD:
-
Chronic kidney disease
- DBP:
-
Diastolic blood pressure
- DM:
-
Diabetes mellitus
- FBG:
-
Fasting blood glucose
- HBV:
-
Hepatitis B virus
- HCV:
-
Hepatitis C virus
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- MANO:
-
Metabolically-abnormal but not obese
- MAO:
-
Metabolically-abnormal and obese
- MHNO:
-
Metabolically-healthy and non-obese
- MHO:
-
Metabolically-healthy but obese
- OR:
-
Odds ratio
- SBP:
-
Systolic blood pressure
References
Shabanzadeh DM. Incidence of gallstone disease and complications. Curr Opin Gastroenterol. 2018;34:81–9.
Lammert F, Acalovschi M, Ercolani G, et al. EASL clinical practice guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol. 2016;65:146–81.
Lin I-C, Yang Y-W, Wu M-F, et al. The association of metabolic syndrome and its factors with gallstone disease. BMC Fam Pract. 2014;15:138.
Li X, Guo X, Ji H, Yu G, Gao P. Gallstones in Patients with Chronic Liver Diseases. Biomed Res Int. 2017;2017:9749802.
Lammert F, Gurusamy K, Ko CW, et al. Gallstones. Nat Rev Dis Prim. 2016;2:16024.
Shabanzadeh DM, Skaaby T, Sørensen LT, Eugen-Olsen J, Jørgensen T. Metabolic biomarkers and gallstone disease–a population-based study. Scand J Gastroenterol. 2017;52:1270–7.
Ahmed F, Baloch Q, Memon ZA, Ali I. An observational study on the association of nonalcoholic fatty liver disease and metabolic syndrome with gall stone disease requiring cholecystectomy. Ann Med Surg. 2017;17:7–13.
Zhu Q, Sun X, Ji X, et al. The association between gallstones and metabolic syndrome in urban Han Chinese: a longitudinal cohort study. Sci Rep. 2016;6:1–9.
Tsai CH, Wu JS, Chang YF, Lu FH, Yang YC, Chang CJ. The number of metabolic abnormalities associated with the risk of gallstones in a non-diabetic population. PLoS One. 2014;9:1–6.
Aune D, Norat T, Vatten LJ. Body mass index, abdominal fatness and the risk of gallbladder disease. Eur J Epidemiol. 2015;30:1009–19.
Bonfrate L, DQH W, Garruti G, Portincasa P. Obesity and the risk and prognosis of gallstone disease and pancreatitis. Best Pract Res Clin Gastroenterol. 2014;28:623–35.
Karelis AD, St-Pierre DH, Conus F, Rabasa-Lhoret R, Poehlman ET. Metabolic and body composition factors in subgroups of obesity: what do we know? J Clin Endocrinol Metab. 2004;89:2569–75.
Denis GV, Obin MS. 'Metabolically healthy obesity': origins and implications. Mol Asp Med. 2013;34:59–70.
Kim TJ, Kim ER, Hong SN, et al. Metabolic unhealthiness is an important predictor for the development of advanced colorectal neoplasia. Sci Rep. 2017;7:9011.
Luo D, Liu F, Li X, et al. Comparison of the effect of ‘metabolically healthy but obese’ and ‘metabolically abnormal but not obese’ phenotypes on development of diabetes and cardiovascular disease in Chinese. Endocrine. 2015;49:130–8.
Hashimoto Y, Tanaka M, Okada H, et al. Metabolically healthy obesity and risk of incident CKD. Clin J Am Soc Nephrol. 2015;10:578–83.
KGMM A, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international. Circulation. 2009;120:1640–5.
WHO/IASO/IOTF. The Asia-Pacific perspective: redefining obesity and its treatment. Melbourne: Health Communications Australia; 2000.
Venneman NG, van Erpecum KJ. Pathogenesis of gallstones. Gastroenterol Clin N Am. 2010;39:171–83.
Chen J-Y, Hsu C-T, Liu J-H, Tung T-H. Clinical predictors of incident gallstone disease in a Chinese population in Taipei, Taiwan. BMC Gastroenterol. 2014;14:83.
Denis GV, Obin MS. “Metabolically healthy obesity”: origins and implications. Mol Asp Med. 2013;34:59–70.
Stefan N, Häring HU, Hu FB, Schulze MB. Metabolically healthy obesity: epidemiology, mechanisms, and clinical implications. Lancet Diabetes Endocrinol. 2013;1:152–62.
Denis GV, Hamilton JA. Healthy obese persons: how can they be identified and do metabolic profiles stratify risk? Curr Opin Endocrinol Diabetes Obes. 2013;20:369–76.
Blüher M. Mechanisms in endocrinology: are metabolically healthy obese individuals really healthy? Eur J Endocrinol. 2014;171:R209–19.
Ryoo JH, Park SK, Ye S, et al. Estimation of risk for diabetes according to the metabolically healthy status stratified by degree of obesity in Korean men. Endocrine. 2015;50:650–8.
Shen HC, Hu YC, Chen YF, Tung TH. Prevalence and associated metabolic factors of gallstone disease in the elderly agricultural and fishing population of taiwan. Gastroenterol Res Pract. 2014;2014:876918.
Stinton LM, Myers RP, Shaffer EA. Epidemiology of gallstones. Gastroenterol Clin N Am. 2010;39:157–69.
Lirussi F, Nassuato G, Passera D, et al. Gallstone disease in an elderly population: the Silea study. Eur J Gastroenterol Hepatol. 1999;11:485–91.
Agrusa A, Romano G, Frazzetta G, et al. Role and outcomes of laparoscopic cholecystectomy in the elderly. Int J Surg. 2014;12:S37–9.
Magnuson TH, Ratner LE, Zenilman ME, Bender JS. Laparoscopic cholecystectomy: applicability in the geriatric population. Am Surg. 1997;63:91–6.
Li X, Gao P. Hepatitis C virus infection increases risk of gallstone disease in elderly Chinese patients with chronic liver disease. Sci Rep. 2018;8:14–9.
Wong RJ, Gish RG. Metabolic manifestations and complications associated with chronic hepatitis C virus infection. Gastroenterol Hepatol (NY). 2016;12:293–9.
Stepanova M, Lam B, Younossi Y, Srishord MK, Younossi ZM. Association of hepatitis C with insulin resistance and type 2 diabetes in US general population: the impact of the epidemic of obesity. J Viral Hepat. 2012;19:341–5.
Acalovschi M, Buzas C, Radu C, Grigorescu M. Hepatitis C virus infection is a risk factor for gallstone disease: a prospective hospital-based study of patients with chronic viral C hepatitis. J Viral Hepat. 2009;16:860–6.
Negro F. HCV infection and metabolic syndrome: which is the chicken and which is the egg? Gastroenterology. 2012;142:1288–92.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
WWS designed the study. PYS and YFC wrote the manuscript and contributed to literature review. CTK contributed to collect and analyzed the data. YCH contributed to the interpretation of data and revised the manuscript. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study’s protocol was approved by the institutional review board at Changhua Christian Hospital in Taiwan (CCH IRB No: 150807) and conducted in compliance with the declaration of Helsinki. The ethics committee waived the need for informed consent from the participants because the data in this research was de-linked and anonymized. Only researchers who meet the criteria for access to confidential data of Changhua Christian Hospital/ Ethics committee can request the data.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Table S1. Baseline characteristics of participants according to participants < 50 and ≥ 50 years. (DOCX 16 kb)
Additional file 2:
Table S2. Risk of gallstones in multivariate analyses. (DOCX 16 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Su, Py., Hsu, YC., Cheng, Yf. et al. Strong association between metabolically-abnormal obesity and gallstone disease in adults under 50 years. BMC Gastroenterol 19, 117 (2019). https://doi.org/10.1186/s12876-019-1032-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-019-1032-y