
Abstract
Background
Globus pharyngeus is common and has a low cure rate. Its etiology is complex and reported to be associated with laryngopharyngeal reflux (LPR). However, some patients with globus do not exhibit any reflux symptoms or respond to proton pump inhibitors (PPIs) treatments. The purpose of this study was to clarify the related risk factors of these patients with a final objective of improving the curative effect.
Methods
Forty two patients afflicted with globus pharyngeus (G group) and 38 patients without globus pharyngeus (NG group) were included in this study. According to the laryngopharyngeal Reflux Symptom Index and the response to PPIs treatments, the patients were further divided into reflux groups (G-R, NG-R) and non-reflux groups (G-NR, NG-NR). High Resolution Manometry (HRM) was performed to assess esophageal motility. Questionnaires, including categories such as life exposure factors, were conducted.
Results
a) The average resting and residual pressures of the upper esophageal sphincter (UES) in the G-NR group was higher than in the NG-NR and NG-R groups (P < 0.05). b) The average resting and residual pressures of the lower esophageal sphincter showed no differences between the G-NR group and the NG-NR group (P > 0.05). c) The esophageal distal contractile integral score of the G-NR group was not different from the NG-NR group (P > 0.05). d) Compared to the NG-NR group, the G-NR group showed higher incidence of stress, smoking, drinking, high salt and anxiety (P < 0.05).
Conclusions
Globus pharyngeus without LPR may occur due to high UES pressure. Stress, smoking, alcoholic drinking, high salt and anxiety may be its risk factors.
Similar content being viewed by others

Background
Globus pharyngeus is one of the most common diseases encountered in otolaryngology clinics. However, the treatment of globus pharyngeus still has some major problems with low cure rate and high recurrence. Similar patients may often be seen by gastroenterologists [1,2,3]. Manifestations of globus pharyngeus include, but are not limited to, laryngopharyngeal dryness, tightness, burning, obstruction, and foreign body sensation. However, these symptoms are not accompanied by sore throat or difficulty swallowing and/or breathing. The etiologies of globus pharyngeus are very complicated, including the diseases of the pharynx and its adjacent and/or distant organs, systemic disorders, mental factors and functional diseases. With the development of clinical technologies, a large number of studies have been performed [2, 3]. In these studies, researchers found a close relationship between globus pharyngeus and backflow of gastric contents into the throat. In 1987, Wiener et al. placed probes into the esophagus and on the top of the upper esophageal sphincter (UES) to detect pH over a course of 24 h using double-probe pH testing. They found that patients with globus pharyngeus had laryngopharyngeal acid reflux. In 1989, they once again used the similar methods to monitor pH over 24 h in 32 patients with globus pharyngeus. However, this time they reported that the symptoms and the acid reflux times of these patients were all different from gastroesophageal reflux disease (GERD), and esophagitis was hardly found. Since then, research on globus pharyngeus has been extensively performed [4]. Although the results were not completely consistent, laryngopharyngeal reflux (LPR) was officially adopted by the American Academy of Otolaryngology-Head and Neck Surgery in 2002 [5]. However, whether there was a close relationship between globus pharyngeus and laryngopharyngeal reflux and/or gastroesophageal reflux still left some doctors feeling confused. One study showed that abnormal laryngopharyngeal or esophageal reflux was not indicated by pH-impedance monitoring in some patients with suspected LPR refractory to proton pump inhibitors (PPIs) treatments. The results proved that LPR is unlikely in these patients [6]. It can be induced that globus pharyngeus patients with non-LPR (G-NR) also account for a certain proportion. At present, there is no report about the etiologies and influence factors of these patients. This study was performed to clarify the related factors of the symptoms of globus pharyngeus refractory to PPIs treatments and to learn more about G-NR so as to improve the curative effect.
Methods
Study subjects
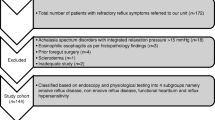
This study recruited 42 “globus pharyngeus” patients (G group) and 38 non-globus pharyngeus patients (NG group) depending on whether they had abnormal laryngopharyngeal sensations. For “globus pharyngeus”, the Rome III definition was met except with the exception of that for reflux disease which was not objectively assessed. All cases were performed using High Resolution Manometry in Gastrointestinal Motility Suit, First Affiliated Hospital of Dalian Medical University from December 1, 2015 to May 1, 2016. The two groups were further divided into laryngopharyngeal non-reflux groups (G-NR group, NG-NR group) and laryngopharyngeal reflux groups (G-R group, NG-R group) according to the laryngopharyngeal Reflux Symptom Index (RSI) and the response to PPIs treatments [7]. This study was approved by the hospital ethics committee (No. LCKY2016–33), and all participants in the study signed the informed consent form.
Inclusion and exclusion criteria
Inclusion and exclusion criteria of the G-NR group (N = 20)
Inclusion criteria
a. Conformed to Rome III criteria for globus [8]: 1) persistent or intermittent, non-painful sensation of a lump or foreign body in the throat; 2) occurrence of the sensation between meals; 3) absence of dysphagia or odynophagia; 4) absence of evidence that gastroesophageal reflux is the cause of the symptom (see b. d. e.); 5) absence of histopathology-based esophageal motility disorders. Criteria fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis. b. no positive sign of inflammation, or only slight inflammation found through the electronic laryngoscopy and electronic gastroscopy; c. no history of drug use within the last 1 month; d. no response to double-dose of PPIs treatment for 8 ~ 12 weeks: no improvement in laryngopharyngeal symptoms; e. RSI scores < 13 [7].
Exclusion criteria
a. Accompanied by malignant tumor, immune system disease, metabolic disease, heart and lung diseases and severe local infection, etc.; b. unable to tolerate the esophageal pressure test performed by High Resolution Manometry.
Inclusion and exclusion criteria of the G-R group (N = 22)
Inclusion criteria
a. Abnormal feelings such as persistent or intermittent foreign body, formication sign, burning, tightening, muffled, narrow sense and sputum adhesion were exhibited in the oropharynx and suprasternal fossa, without the presence of dysphagia, sore throat or difficulty swallowing and/or breathing; b. no positive sign of inflammation, or only slight inflammation found through the electronic laryngoscopy and electronic gastroscopy; c. no history of drug use within the last 1 month. d. response to PPIs treatment. e. RSI scores ≥ 13 [7].
Exclusion criteria
Others are in agreement with those of the G-NR Group.
Inclusion and exclusion criteria of NG-NR group (N = 20)
Inclusion criteria
No symptoms of globus pharyngeus, such as laryngopharyngeal dryness, tightness, burning, obstruction or foreign body sensation; no sore throat, difficulty swallowing and/or breathing; but received the high resolution esophageal motility test for non-cardiac chest pain, i.e., pain or discomfort behind the sternum without any cardiopulmonary diseases. Other inclusion and exclusion criteria are in agreement with those of the G-NR Group.
Inclusion and exclusion criteria of NG-R group (N = 18)
Inclusion criteria
No symptoms of globus pharyngeus, but received esophageal pressure measurements because of the mild discomfort behind the sternum. Other inclusion and exclusion criteria are in agreement with those of the G-R Group.
Questionnaires
The study participants completed the questionnaires under the guidance of a member of the study team who was present to ensure that the participants understood the forms clearly. However, the study member was prohibited from using any suggestive words regarding any of the questions.
General information
The general questionnaire included information about name, demographic data (age and gender), marriage, occupation, education, income, concomitant diseases, medications in use and family history.
RSI version
Patient information related to LPR symptoms was gathered through a questionnaire containing the validated version of RSI. The RSI score was applied as proposed by Belafsky et al., and LPR diagnosis was based on the RSI score ≥ 13 [7, 9]. A self-administered nine-item RSI was completed by the patients in less than 1 min. The score for each item ranged from 0 (none) to 5 (most severe) with a maximum total score of 45. The nine items included:1) hoarseness or a problem with your voice; 2) clearing your throat; 3) excessive throat mucus or postnasal drip; 4) difficulty swallowing food, liquids or pills; 5) coughing after eating or lying down; 6) breathing difficulties or choking episodes; 7) troublesome or annoying cough; 8) sensation of something sticking in your throat or a lump in your throat; 9) heartburn, chest pain, indigestion, or stomach acid reflux (Additional file 1).
Life exposure factors questionnaire [9,10,11]
Life exposure factors concerning behavioral characteristics probably related to globus pharyngeus were gathered through a questionnaire containing 17 items: smoking, alcohol, tea, coffee, chocolate, spicy food, greasy meal, fullness, high salt, night work, staying up late, fatigue, pressure, constipation, loneliness, anxiety and depression (Additional file 2).
Esophageal motility measurement
High resolution manometry was performed using a 24-channel water-perfused catheter of 4.0 mm in diameter as used previous studies [12](Ningbo Maida Medical Device Inc., Ningbo, China). Side hole 1, which starts at the most distal point, was 5 cm from hole 2. Holes 2–7 were 1.0 cm from each other and holes 8–24 were 1.5 cm from each other. Once placed, it covered the entire length of the esophagus from the upper esophageal sphincter to the lower esophageal sphincter with an additional channel in the stomach. The data acquisition frequency was 20 Hz for each sensor. Computer analysis software (Video was recorded by MedSample360 at a rate of 20 frames/s and analyzed by MedView360) was used to assess various esophageal motility parameters.
The patients were asked to fast for 12 h for foods and 6 hours for water before the measurement. The high resolution esophageal motility test was performed in a supine position. Firstly, a 30-s period of basal recording was obtained after the appropriate placement of the catheter. Then, the patient was asked to swallow 5 ml of water and the swallow was repeated for a total of 10 times with a 30-s interval between consecutive swallows. Lastly, multiple rapid swallows (5 swallows of 2 ml of water with 2- to 3-s intervals) were performed. The resting pressure and residual pressure of the UES and low esophageal sphincter (LES), as well as the esophageal distal contractile integral (DCI), were recorded.
Statistical analysis
All data were inputted into the SPSS 22.0 software package for processing. The λ [2] test was used for analysis of the correlation between the G group, the NG group and life exposure factors. The categorical data was shown using the percentage and analyzed by the λ [2] test. The measurement data are presented as mean ± standard deviation (x ± s). The Student’s t test was used for comparison between two groups. The significance level for all hypothesis testing (p-value) was 0.05.
Results
General data of patients
In the G group, the number of patients with non-laryngopharyngeal reflux symptoms (G-NR group) was 20/42, accounting for 48%; the number of patients with laryngopharyngeal reflux symptoms (G-R group) was 22/42, accounting for 52% (See Table 1). No statistical differences (P > 0.05) were noted in age among the 4 groups of patients (see Table 1).
Esophageal pressure results from HRM
Images of esophageal pressure measurements
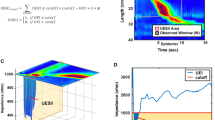
Typical images of esophageal motility measurements during a wet swallow in 4 different groups of patients are presented in Fig. 1. The top and bottom pressure bands reflect the UES and LES pressures before, during and after a wet swallow, respectively. The pressure tracings in between the UES and LES reflect esophageal body pressure changes during the swallow.

Typical high resolution esophageal manometric measurements in different groups of patients. a-d G-NR, G-R, NG-R and NG-NR
Analysis of UES
The average resting pressure of the UES in patients of the G group was higher than those in the NG group (P < 0.05, Fig. 2a). The resting UES pressure in the G-NR group was higher than that in the NG-R and NG-NR groups (P < 0.05), but lower than that in the G-R group (P < 0.05) (Fig. 2b). Similar differences were noted in the residual UES pressure among the groups: the average residual pressure of the UES in the G group was higher than that in the NG group (Fig. 2c); the average residual UES pressure in the G-NR group was higher than that in the NG-R and NG-NR groups (P < 0.05), but lower than that in the G-R group (P < 0.05) (Fig. 2d).

Esophageal manometric parameters in different groups of patients. a Average resting pressure of UES in patients with globus and patients without globus; b Average resting pressure of UES in 4 subgroups of patients; c Average residual pressure of UES in patients with globus and patients without globus; d Average residual pressure of UES in 4 subgroups of patients; e Average resting pressure of LES in patients with globus and patients without globus; f Average resting pressure of LES in 4 subgroups of patients; g Average residual pressure of LES in patients with globus and patients without globus; h Average residual pressure of LES in 4 subgroups of patients; i The DCI in patients with globus and patients without globus; j The DCI in 4 subgroups of patients
Analysis of LES
There was no statistical difference in the average resting pressure of the LES between the G group and the NG group (P > 0.05, Fig. 2e). The average resting pressure of the LES in the G-NR group was higher than that in the two G-R and NG-R reflux groups (P < 0.05) and showed no statistical difference with that in the NG-NR group (P > 0.05) (see Fig. 2f). The residual pressure of the LES exhibited similar results as the resting pressure of the LES among the groups (see Fig. 2g and 2h).
Analysis of DCI
There was no statistical difference in the DCI between the G group and the NG group (P > 0.05, Fig. 2i). The DCI in the G-NR group was higher than that in the G-R and NG-R groups (P < 0.05, Fig. 2j). No statistical difference was shown in the DCI between the G-NR group and the NG-NR group (P > 0.05, Fig. 2j).
Comparison of age, sex and life exposures between groups
Age characteristics of G-NR patients
The average age of patients was 51 years in the G-NR group, 50 years in the G-R group, 52 years in the NG-R group, and 51 years in the NG-NR group (See Table 1). Both the median age and the mean age were within the middle range (45–60 years) described by the World Health Organization. The age difference was shown to be insignificant between the groups (P > 0.05). These results suggested that the middle age could be a risk factor for globus pharyngeus (including G-NR).
Analysis of sex and life exposure factors in G-NR patients
As shown in Tables 1 and 2, females accounted for the majority of patients in the G-NG group. So the gender female was taken as an investigative factor in the study. From the comparison of the results in G and NG of Table 2, we found that the incidences of smoking, alcohol consumption, high salt and anxiety were higher in the G group than in the NG group (P < 0.05). From the comparison of the results in G-NR and G-R of Table 2, we found that the incidences of smoking, alcohol consumption and anxiety were lower in the G-NR group than the G-R group (P < 0.05). From Table 1, we can see that the prevalence of globus pharyngeus was higher in female. However, from the comparison of the results in G-NR and NG-NR of Table 2, we found that the incidences of stress, smoking, alcohol consumption, consumption of high salt and anxiety were higher in the G-NR group compared with the NG-NR group (P < 0.05). Similarly, the prevalence of globus pharyngeus was higher in female than in male.
Discussion
In this study we have found that the average resting and residual pressures of the UES in the patients with globus pharyngeus without laryngopharyngeal reflux were higher than in the patients without globus pharyngeus. The patients with globus pharyngeus but no laryngopharyngeal reflux showed higher incidences of stress, smoking, alcohol-drinking, high-salt and anxiety than the patients without globus pharyngeus or laryngopharyngeal reflux.
The symptoms of globus pharyngeus are usually present with dry swallowing rather than swallowing food [13]. They may be intermittent or sustainable, often accompanied by other symptoms such as belching or chest tightness [14, 15]. The etiologies and mechanisms of globus pharyngeus have been unclear [16]. Some studies suggested that these symptoms might be associated with rhinitis, sinusitis, thyroid diseases, sore throat, GERD, gastroduodenal ulcer, iron deficiency anemia, psychological disorders, etc. [17, 18]. However, most researchers consider globus pharyngeus as a series of symptoms without organic diseases that are more like hysteria defined as a subjective feeling of throat discomfort.
Wada [19] reported that GERD could cause globus pharyngeus. LPR is believed to be attributed to abnormal motility of the UES and may often arise in daytime or in an upright position, especially during a physical exertion. If the PPI treatment is effective, the diagnosis of LPR can be considered. Otherwise further examinations are needed to determine the etiologies of globus pharyngeus [20,21,22].
The HRM system can provide clear, intuitive and accessible images and data of esophageal motility. However, there have been limited reports on the assessment of globus pharyngeus using the HRM techniques [23]. Our results showed that the resting and residual pressures of the UES in the globus pharyngeus group were higher than those of the non-globus pharyngeus group. These elevated UES pressure may be responsible to cause symptoms of globus via the vagal afferent pathway. The UES plays an important role in preventing reflux of esophageal contents through the throat and into the mouth. It was also found in this study that the resting and residual pressures of the UES in patients with globus and LPR were higher than those in patients with globus but no LPR; this elevation might be attributed to stimulation of the UES by the refluxed gastric acid [24].
The results of our study showed that patients with LPR with or without globus showed a reduced LES pressures in both resting and residual states, suggesting that symptoms of LPR might be caused by a low pressure of LES which is known to be a decisive factor in the occurrence of gastroesophageal reflux. Furthermore, the refluxed gastric acid could stimulate the ring pharyngeal muscle around the UES and result in spasms [24, 25]. The fact that patients with globus but no LPR exhibited normal LES pressure suggested that globus pharyngeus might not be associated with gastroesophageal reflux.
In this study, no significant difference was noted in DCI between the G-NR and NG-NR groups, indicating normal esophageal body motility in G-NR patients. However, the DCI in the G-R and NG-R groups was reduced in comparison with the NG-NR group, suggesting that abnormal esophageal body motility could occur in both reflux groups with and without globus pharyngeus. Most of previous studies were performed in the G-R group and yielded similar results [1, 26], whereas, little attention has been pain in the G-NR group. Weak distal esophageal smooth muscle contractions result in feeble peristalsis and decreases scavenging abilities of bolus and refluxed stomach contents. The residual food and refluxed acid may then stimulate the local esophagus, aggravating symptoms of laryngopharyngeal abnormal sensation [27, 28]. On contrary, the globus symptoms in the G-NR patients who showed normal DCI or peristalsis could not attributed to acid reflux or food/bolus retention. Taken together, the symptoms in the G-NR patients might be attributed mainly to the high pressure of the UES.
The life exposure factors play an important role in the occurrence and development and even treatment of diseases [11]. This study further explored relationships between age, sex, and life exposures in the G-NR. The mean age and median age of the patients in each group were all within the World Health Organization-specified middle-age range. Accordingly, the middle age could be regarded as a risk factor for globus pharyngeus, as in the cases of G-NR groups. Compared with the NG group, the G group had a higher incidence of smoking, alcohol consumption, eating high salt, and anxiety as well as a higher prevalence of globus pharyngeus in female. The incidence of globus pharyngeus was previously reported to be correlated with both anxiety and depression [29, 30]; however, the depression as a risk factor was not indicated in this study. Furthermore, we compared the G-NR group with the G-R group and found that the incidence of smoking, drinking and anxiety was lower in the G-NR patients. Combined with the above mentioned factors, the incidence of globus pharyngeus without reflux may be more likely to occur in middle-aged women, especially those with smoking habits, high rates of alcohol consumption and anxiety, but these habits have been shown to be more common in patients with reflux symptoms. Further, we compared the G-NR group with the NG-NR group and found a higher incidence of smoking, alcohol consumption, high salt consumption, stress and anxiety in the G-NR patients; in addition, the prevalence of globus pharyngeus was higher in female than male.
This study was limited in a number of issues: a) The number of patients recruited was limited, so a multi-center and large sample study could be performed. b) In our study, the NG-NR group acted as the control group only according to the RSI scores and responses to proton pump inhibitors (PPIs) treatments which may be used as objective parameters with low cost and high practicality [31, 32]. 24-h pH monitoring was not performed during the experiment to completely exclude the possibility of reflux [33].
Conclusions
Globus pharyngeus without LPR may occur due to high UES pressure. Stress, smoking, alcoholic drinking, high salt consumption and anxiety may be its risk factors.
Abbreviations
- DCI:
-
Distal esophageal contraction integral
- GERD:
-
Gastroesophageal reflux disease
- HRM:
-
High Resolution Manometry
- LES:
-
Lower esophageal sphincter
- LPR:
-
Laryngopharyngeal reflux
- LPRD:
-
Laryngopharyngeal reflux disease
- PPIs:
-
Proton pump inhibitors
- RSI:
-
reflux symptom index
- UES:
-
Upper esophageal sphincter
- WHO:
-
the World Health Organization
References
Wang Z, Chen Y, Guo T. Analyses of the characteristics of esophageal motility in patients with pharyngeal paraesthesia who visit the Department of Gastroenterology. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2015;50(7):569–72.
Davids T, Sommer DD, Armstrong D. Survey of current perspectives on laryngopharyngeal reflux among Canadian otolaryngologists. J Otolaryngol Head Neck Surg. 2008;37(2):196–202.
Bărboi OB, Prelipcean CC, Cobzeanu MD, et al. The tribes and tribulations of laryngopharyngeal reflux: a review of recent studies with implications for interdisciplinary collaborations between otolaryngologists and gastroenterologists. Rev Med Chir Soc Med Nat Iasi. 2015;119(4):967–73.
Joniau S, Bradshaw A, Esterman A, Carney AS. Reflux and laryngitis: a systematic review. Otolaryngol Head Neck Surg. 2007;136(5):686–92.
Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology-Head and Neck Surgery. Otolaryngol Head Neck Surg. 2002;127(1):32–5.
Dulery C, Lechot A, Roman S, et al. A study with pharyngeal and esophageal 24-hour pH-impedance monitoring in patients with laryngopharyngeal symptoms refractory to proton pump inhibitors. Neurogastroenterol Motil. 2017;29(1)
Belafsky PC, Postma GN, Koufman JA. Validity and reliability of the reflux symptom index (RSI). J Voice. 2002;16:274–7.
Galmiche JP, Clouse RE, Bálint A, et al. Functional esophageal disorders. Gastroenterology. 2006;130:1459–65.
Wei C. A Meta-analysis for the role of proton pump inhibitor therapy in patients with laryngopharyngeal reflux. Eur Arch Otorhinolaryngol. 2016;273(11):3795–801.
Cook MB. Optimization and expansion of predictive models for Barrett's esophagus and esophageal adenocarcinoma: could a life-course exposure history be beneficial? Am J Gastroenterol. 2013;108(6):923–5.
Pierce JL, Tanner K, Merrill RM, Miller KL, Kendall KA, Roy N. Swallowing disorders in Sjögren's syndrome: prevalence, risk factors, and effects on quality of life. Dysphagia. 2016;31(1):49–59.
Zhou WC, Jia L, Chen DY, Liu Y, Liu J, Jiang SM, Yang M, Xu J. The effects of paroxetine and amitriptyline on the upper esophageal sphincter (UES) pressure and its natural history in globus pharyngeus. Dig Liver Dis. 2017 Jul;49(7):757–63.
Ford CN. Evaluation and management of larygopharyngeal reflux. JAMA. 2005;294(12):1534–40.
Kosoff RE, Gardiner KL, Merlo LM, Pavlov K, Rustgi AK, Maley CC. Development and characterization of an organotypic model of Barrett's esophagus. J Cell Physiol. 2012;227(6):2654–9.
Rong Z, Haibing L. Diagnosis and treatment of laryngopharyngeal reflux disease. J Clin Otorhinolaryngol Head Neck Surg (China). 2011;25(15):690–1.
Foden N, Ellis M, Shepherd K, Joseph T. A feeling of a lump in the throat. BMJ. 2014;348
Wada T, Sasaki M, Kataoka H, et al. Gastroesophageal and laryngopharyngeal reflux symptoms correlate with histopathologic inflammation of the upper and lower esophagus. J Clin Gastroenterol. 2009;43(3):249–52.
Yılmaz T, Bajin MD, Günaydın RÖ, Ozer S, Sözen T. Laryngopharyngeal reflux and helicobacter pylori. World J Gastroenterol. 2014;20(27):8964–70.
Lee BE, Kim GH, Ryu DY, et al. Combined dual channel impedance/pH-metry in patients with suspected Laryngopharyngeal reflux. J Neurogastroenterol Motil. 2010;16(2):157–65.
Lam PK, Ng ML, Cheung TK, et al. Rabeprazole is effective in treating laryngopharyngeal reflux in a randomized placebo-controlled trial. Clin Gastroenterol Hepatol. 2010;8(9):770–6.
Vaezi MF, Hagaman DD, Slaughter JC, et al. Proton pump inhibitor therapy improves symptoms in postnasal drainage. Gastroenterology. 2010;139(6):1887–93.
Guo H, Ma H, Wang J. Proton pump inhibitor therapy for the treatment of Laryngopharyngeal reflux: a meta-analysis of randomized controlled trials. J Clin Gastroenterol. 2016;50(4):295–300.
Peng L, Patel A, Kushnir V, Gyawali CP. Assessment of upper esophageal sphincter function on high-resolution manometry: identification of predictors of globus symptoms. J Clin Gastroenterol. 2015;49(2):95–100.
Ertekin C, Turman B, Tarlaci S, et al. Cricopharyngeal sphincter muscle responses to transcranial magnetic stimulation in normal subjects and in patients with dysphagia. Clin Neurophysiol. 2001;112(1):86–94.
Smout AJ, Bredenoord AJGERD. A challenge to our view of reflux oesophagitis pathogenesis. Nat Rev Gastroenterol Hepatol. 2016;13(9):504–5.
Mello MD, Shriver AR, Li Y, Patel A, Gyawali CP. Ineffective esophageal motility phenotypes following fundoplication in gastroesophageal reflux disease. Neurogastroenterol Motil. 2016;28(2):292–8.
Zhang S, Joseph AA, Gross L, Ghadimi M, Frahm J, Beham AW. Diagnosis of gastroesophageal reflux disease using real-time magnetic resonance imaging. Sci Rep. 2015;5:12112.
Bredenoord AJ, Weusten BL, Curvers WL, Timmer R, Smout AJ. Determinants of perception of heartburn and regurgitation. Gut. 2006;55(3):313–8.
Tang B, Cai HD, Xie HL, Chen DY, Jiang SM1, Jia L. Epidemiology of globus symptoms and associated psychological factors in China. J Dig Dis 2016; 17(5):319-324.
Martinucci I, de Bortoli N, Savarino E, et al. Optimal treatment of laryngopharyngeal reflux disease. Ther Adv Chronic Dis. 2013;4(6):287–301.
Nunes HS, Pinto JA, Zavanela AR, Cavallini AF, Freitas GS, Garcia FE. Comparison between the reflux finding score and the reflux symptom index in the practice of otorhinolaryngology. Int Arch Otorhinolaryngol. 2016;20(3):218–21.
Heloisa Sobreira Nunes1;José Antonio Pinto1;Adma Roberta Zavanela1;André Freitas Cavallini1;Gabriel Santos Freitas1;Fabiola Esteves Garcia1.Comparison between the Reflux Finding Score and the Reflux Symptom Index in the Practice of Otorhinolaryngology[J].Int Arch Otorhinolaryngol.2016,20(3): 218–221.
Cumpston EC, Blumin JH, Bock JM. Dual pH with multichannel Intraluminal impedance testing in the evaluation of subjective Laryngopharyngeal reflux symptoms. Otolaryngol Head Neck Surg. 2016;155(6):1014–20.
Acknowledgements
We are indebted to all related departments of our hospital for their encouraging criticism and discussions.
Funding
The authors received no specific funding for this work.
Availability of data and materials
All relevant data are included within the paper and their supporting information files. Raw Data are available from the corresponding author for researchers who meet the criteria for access to confidential data.
Author information
Authors and Affiliations
Contributions
Study concept and design: HD, ZD, JC. Acquisition of data, analysis and interpretation of data: DY, ZZ, LW, XS, YY, XL, HY, SW. Drafting of the manuscript: HD, ZD, JC, DY, ZZ, LW, XS, YY,XL, HY, SW. Critical revision of the manuscript for important intellectual content: HD, ZD, JC. Statistical analysis: HD. Administrative, technical, or material support: HD, ZD,JC, DY, ZZ, LW, XS, YY, XL,HY, SW. Study supervision: ZD, JC. Final approval of the version to be published: HD, ZD, JC, DY, ZZ, LW, XS, YY, XL, HY, SW.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee of First Affiliated Hospital of Dalian Medical University Ethical approved the report of scientific research project. It confirmed that project program and informed consent were reviewed. All the human subjects in the study had signed the informed consent. (Approval number: LCKY2016–33).
Additional files.
Additional file 1:
Additional file 2: Life exposure factors questionnaire.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
The reflux symptom idex. (DOCX 68 kb)
Additional file 2:
Life exposure factors questionnaire. (ZIP 45 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Ding, H., Duan, Z., Yang, D. et al. High-resolution manometry in patients with and without globus pharyngeus and/or symptoms of laryngopharyngeal reflux. BMC Gastroenterol 17, 109 (2017). https://doi.org/10.1186/s12876-017-0666-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-017-0666-x