
Abstract
Background
The average delay in diagnosis for patients with axial spondyloarthritis (axSpA) is 7 to 10 years. Factors that contribute to this delay are multifactorial and include the lack of diagnostic criteria (although classification criteria exist) for axSpA and the difficulty in distinguishing inflammatory back pain, a key symptom of axSpA, from other highly prevalent forms of low back pain. We sought to describe reasons for diagnostic delay for axSpA provided by primary care physicians.
Methods
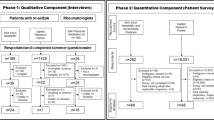
We conducted a qualitative research study which included 18 US primary care physicians, balanced by gender. Physicians provided informed consent to participate in an in-depth interview (< 60 min), conducted in person (n = 3) or over the phone (n = 15), in 2019. The analysis focuses on thoughts about factors contributing to diagnostic delay in axSpA.
Results
Physicians noted that the disease characteristics contributing to diagnostic delay include: back pain is common and axSpA is less prevalent, slow progression of axSpA, intermittent nature of axSpA pain, and in the absence of abnormal radiographs of the spine or sacroiliac joints, there is no definitive test for axSpA. Patient characteristics believed to contribute to diagnostic delay included having multiple conditions in need of attention, infrequent interactions with the health care system, and “doctor shopping.” Doctors noted that patients wait until the last moments of the clinical encounter to discuss back pain. Problematic physician characteristics included lack of rapport with patients, lack of setting appropriate expectations, and attribution of back pain to other factors. Structural/system issues included short appointments, lack of continuity of care, insufficient insurance coverage for tests, lack of back pain clinics, and a shortage of rheumatologists.
Conclusion
Primary care physicians agreed that lengthy axSpA diagnosis delays are challenging to address owing to the multifactorial causes (e.g., disease characteristics, patient characteristics, lack of definitive tests, system factors).
Similar content being viewed by others

Background
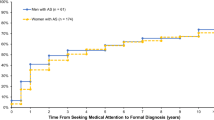
The average delay in diagnosis for patients with axial spondylarthritis (axSpA) [1,2,3] ranges from 7 to 10 years [4,5,6,7,8], with estimates as high as 13 years between symptom onset and diagnosis in the United States [9]. The significant diagnostic delay is a well-known feature of spondyloarthritis management [10]. Patients with longer delay in diagnosis (e.g., > 5 years) display more structural damages and limited spinal mobility [11]. In addition, patients may experience distress, depression, and desperation associated with their prolonged search for diagnosis and treatment [12]. Therefore, the improvement of delay in diagnosis for axSpA may slow disease progression and thus avoid or delay serious disability due to the early treatment interventions and access to care [13].
The delay in diagnosis for axSpA is multifactorial including characteristics of the patients, providers, healthcare system, and disease itself. For instance, patients may seek care from different medical professionals without guidance due to varied disease manifestations of axSpA or the lack of proper access to care (e.g., limited rheumatologists). Despite the use of sensitive imaging tool such as magnetic resonance imaging, the delayed diagnosis for patients with non-radiographic axSpA is still significant [14]. On the other hand, physicians may also play an important role in the early diagnosis of axSpA. Despite the low awareness of axial SpA among non-rheumatologist physicians [13], most axSpA patients are diagnosed by non-rheumatologists [15], with rheumatologists having diagnosed only 37% between 2000 and 2012 [16]. Primary care physicians may have difficulty discriminating inflammatory back pain from other types of back pain and may be unaware of other features that are important in making a diagnosis of axSpA.
In this qualitative research study, we sought the perspectives of primary care physicians to gain a better understanding of the reasons for diagnostic delay in primary care settings. We chose a qualitative approach because qualitative data frequently yield surprising insights and provide in-depth detail about participants’ perceptions and experiences that quantitative data often cannot [17]. Such foundational knowledge may be useful in developing interventions to reduce the delay in diagnosis of axSpA.
Methods
The University of Massachusetts Medical School Institutional Review Board approved this study.
Study design
The physician in-depth interviews were part of a larger qualitative study- The SpondyloArthritis Screening and Early Detection (SpA-SED) Study. Our protocol was guided by best practices for the conduct and reporting of qualitative research (COREQ) [18]. The appropriately completed COREQ checklist for the current study is included (Appendix A).
Participant recruitment
We recruited 18 primary care physicians (a sample size likely adequate to achieve saturation) who were willing to participate in a recorded, 60-min in-depth discussion. We used purposive sampling to enroll equal numbers of men and women and family medicine and internal medicine physicians. Thirty-four participants including those who were known to the research team or their colleagues (approached by emails) or who were identified through state and regional primary care professional societies (face-to-face) were invited to participate. Six declined, nine were non-responders, and one physician was not selected because of our need for balance by gender and type of physician. All 18 participants participated in scheduled interviews and completed the study. Participants were offered a cash card of $300 to compensate for their time.
Study setting
The interviews were conducted either in person in a private conference room in Rhode Island or Massachusetts (n = 3) or over the phone (n = 15) between February–May 2019. We conducted phone interviews using Zoom.
Interview guide
A multidisciplinary team developed the interview guide (< 60 min interviews, Appendix B). Questions included experience with back pain, how back pain is evaluated, what laboratory tests are ordered when axSpA is suspected, what referrals participants would make, awareness of axSpA, speculation about what contributes to diagnostic delay in axSpA, etc. The average length of the interviews was 47.1 min (standard deviation: 11.3).
Conduct of interviews
Interviews were conducted by experienced, trained personnel (KLL, DS), with an observer from the research team participating and taking notes. For one interview, the research interviewer (KLL) had previously worked as an investigator on a research project with the physician participant (> 5 years previously). Research staff were trained to assure standardized data collection. The protocol was pilot tested with one physician. The researchers conducting the interviews reported no obvious bias but did report prior assumptions that lack of awareness of axSpA and lack of time would emerge as leading barriers to axSpA screening in primary care settings. No repeat interviews were conducted.
Data collection and management
The study data were collected and managed using REDCap electronic data capture tools hosted at the University of Massachusetts Medical School [19]. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing: 1) an intuitive interface for validated data entry; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for importing data from external sources.
Analytic strategy
We conducted a group method of data analysis known as immersion / crystallization [20]. Four team members independently listened to selected interview recordings, read in-depth transcripts, and wrote analytic notes for each. The transcript texts were subjected to line-by-line coding with NVivo qualitative software [21]. The codebook was modified by team consensus. Searches for alternative interpretations were conducted again and discussed before final decisions were made about how to report the findings of the study. This manuscript focused on one parent node in our coding scheme: Reasons for Diagnostic delay.
Feedback from participants
We prepared a preliminary report of our findings and emailed participants who indicated they were willing to review and provide feedback (Appendix C).
Results
Of the participants, 44% were women, 66.7% were non-Hispanic white and 83.3% attended an allopathic medical school in the United States (Table 1). All physicians considered that the length of diagnostic delay was problematic, and all agreed that this delay was unacceptable. Physicians believed that multiple factors were contributing to the diagnostic delay in axSpA. Figure 1 depicts the multifactorial components perceived by primary care providers participating in the study. Barriers to early diagnosis included disease characteristics (e.g., slow disease progression; Table 2), patient factors (e.g., multiple other conditions, back pain not chief complaint, Table 3), physician characteristics (e.g., lack of rapport/trust, Table 4), and structural/system issues (e.g., lack of time, Table 5). Primary care physicians noted that, because back pain is multifactorial and very common and axSpA is not, axSpA may be missed. Physicians explained that the slow progression of the disease may contribute to the diagnostic delay. The intermittent nature of symptoms and range of symptoms severity related to axSpA also was noted as a factor contributing to diagnostic delay. Additionally, physicians pointed out that it takes time for radiographic evidence to appear and that there are no other definitive diagnostic tests.

Factors influencing timely diagnosis of axSpA
A common theme was that patients do not interact frequently enough with the health care system and the lack of continuity of care (Table 3). Primary care physicians uniformly noted that patients often have multiple issues to discuss and back pain is mentioned only at the very end of the visit. Physicians did not discuss why patients waited until the last moment to share their complaints of back pain. Some physicians explained that they are likely to attribute back pain to other conditions (Table 4); most emphasized the need to establish trust and a good rapport with patients. The importance of setting appropriate expectations with patients was noted, since back pain may not be addressed adequately in one visit. Primary care physicians lamented that the limited amount of time available for appointments impedes their ability to diagnose axSpA in a timely fashion (Table 5). Further, physicians noted that the lack of continuity of care may contribute to diagnostic delay. Patient concerns about the expense of copayments expected when undergoing testing needed to evaluate axSpA may also contribute to the diagnostic delay. The lack of dedicated spine clinics and the shortage of rheumatologists were reported as barriers to timely diagnosis.
Discussion
This study sheds light on the challenges faced by primary care physicians that may contribute to the delay in diagnosing axSpA, which typically presents with the insidious onset of back pain that often is attributed to other, more prevalent conditions [22, 23]. The subjective quality of pain may be difficult for patients to describe and is not easily measured objectively. In our study, primary care physicians noted that axSpA patients may not interact frequently enough with the health care system to facilitate a correct diagnosis. Consistent with previous research [16], lack of diagnostic criteria, lack of definitive biomarkers, and lack of radiographic confirmation of axSpA until later in the disease course [13, 24] were identified as factors contributing to axSpA diagnostic delay.
Several physician-related factors that may contribute to diagnostic delay were identified, including a lack of awareness about axSpA among non-rheumatology health care professionals [9]. Lack of trust, poor rapport, ineffective communication, and misaligned expectations between providers and patients were factors that likely contribute to diagnostic delay. Among patients with immune-mediated inflammatory diseases, distrust of health care providers has been associated with poor medication adherence [25] while, conversely, good patient-provider communication has been shown to improve health outcomes [26]. Our participants also reported that patients may not realize that axSpA often is not diagnosed during a single visit, but rather involves a journey that occurs over a period of time. Physicians mentioned that infrequent contact with the health care system and lack of continuity of care contributed to the diagnostic delay. To our knowledge, research has not been conducted on whether discordant expectations between patients being evaluated for axSpA and their primary care physicians contributes to diagnostic delay. Nevertheless, improved alignment of patient expectations to care processes may improve patient continuity of care.
Primary care physicians mentioned system-level factors that impede timely diagnosis of axSpA, including the short appointment length and difficulty arranging rheumatology referrals. The median length of a primary care visit was 15.7 min, during which a median of six topics were covered with ~ 5 min spent discussing the primary complaint and 1.1 min on each remaining topic [27]. A musculoskeletal or rheumatologic condition accounted for the chief complaint in only about 8.3% of primary care visits [28], which is consistent with reports by providers in our study that mention of back pain may be withheld by patients until the end of the clinical encounter. Patients with axSpA often have multiple conditions, such as hypertension and depression, which might supersede back pain as the main focus of a primary care visit [29]. Given the challenges of reduce time with patients and increased complexity of patient issues, automated tools may be useful to primary care physicians to identify uncommon diseases such as axSpA.
Delays in diagnosis of axSpA also have been attributed to late referral of patients with inflammatory back pain by general practitioners to rheumatologists [15, 16, 30, 31]. However, the average wait for a rheumatology appointment is 4 months [32]. Difficulty accessing rheumatology care is exacerbated by the shortage of and decline in the number of practicing rheumatologists [33]. By 2025, the demand for rheumatologists is projected to exceed supply and a shortage of 3845 rheumatologists is predicted [34, 35]. This shortage results in burdens for patients, including excessive travel time – which may exceed 90 min for some patients [36]. The American College of Rheumatology has proposed multiple strategies to address this workforce shortage, but the extent to which these will be successful remains uncertain.
Limitations must be considered. Most of the participants practiced in Massachusetts and Rhode Island and had academic affiliations. Systems factors may be specific to local context. Physicians with academic affiliations may be more aware of axSpA. Patient factors were reported by the physician participants and are derived from experiences with their own patients. It is possible that physicians only had experience with patients with ankylosing spondylitis. Misinterpretations of direct quotes may have occurred, although the analytic approach used reduced this likelihood. However, despite these potential limitations, our findings appear to be aligned with previous research [16].
Conclusions
Aiming to provide a better understanding of the reasons for diagnostic delay in primary care settings, this study identified primary care physicians’ perceptions of several root causes of diagnostic delay in axSpA. These contributing factors of delay in diagnosis for axSpA were believed to be multifactorial and were attributed to characteristics of patients, providers, the healthcare system, and the disease itself. While in our study primary care physicians felt that the diagnostic delay reported in the literature is lengthy, it must be noted that Primary care physicians believed that strategies to address these barriers and reduce delay in diagnosis of axSpA are needed. Early diagnosis of axSpA is difficult and as such solutions to shorten the diagnostic journey must consider the multitude of contributing factors (i.e., patient, disease, physician, system).
Availability of data and materials
The data analyzed during the current study are not publicly available due to the nature of the qualitative data. We also did not include the sharing of data in our informed consent procedures, so we are unable to share our qualitative data.
Abbreviations
- axSpa:
-
axial spondyloarthritis
- COREQ:
-
Conduct and reporting of qualitative research
- REDCap:
-
Research Electronic Data Capture
- SpA-SED:
-
The SpondyloArthritis Screening and Early Detection
References
Dougados M, van der Linden S, Juhlin R, Huitfeldt B, Amor B, Calin A, et al. The European Spondylarthropathy study group preliminary criteria for the classification spondylarthropathy. Arthritis Rheum. 1991;34:1218–27.
Amor B, Dougados M, Mijiyawa M. Critères de classification des spondylarthropathies [criteria of the classification of spondylarthropathies]. Rev Rhum. 1990;57(2):85–9.
van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984;27:361–8.
https://www.spondylitis.org/For-Primary-Care-Physicians, Accessed 17 July 2018.
Feldtkeller E, Khan MA, van der Heijde D, et al. Age at disease onset and diagnosis delay in HLA-B27 negative vs. positive patients with ankylosing spondylitis. Rheumatol Int. 2003;23:61–6.
Redeker I, Callhoff J, Hoffmann F, et al. Determinants of diagnostic delay in axial spondyloarthritis: an analysis based on linked claims and patient-reported survey data. Rheumatology (Oxford). 2019;58(9):1634–8.
Masson Behar V, Dougados M, Etcheto A, et al. Diagnostic delay in axial spondyloarthritis: a cross-sectional study of 432 patients. Joint Bone Spine. 2017;84(4):467–71. https://doi.org/10.1016/j.jbspin.2016.06.005.
Rudwaleit M, Haibel H, Baraliakos X, et al. The early disease stage in axial spondylarthritis: results from the German Spondyloarthritis inception cohort. Arthritis Rheum. 2009;60:717–27.
Deodhar A, Mease PJ, Reveille JD, et al. Frequency of axial spondyloarthritis diagnosis among patients seen by US rheumatologists for evaluation of chronic back pain. Arthritis Rheum. 2016;68(7):1669–76.
Dougados M, Baeten D. Spondyloarthritis. Lancet. 2011;377:2127–37.
Ibn Yacoub Y, Amine B, Laatiris A, et al. Relationship between diagnosis delay and disease features in Moroccan patients with ankylosing spondylitis. Rheumatol Int. 2012;32:357–60.
Martindale J. The Impact of Delay in Diagnosing Ankylosing Spondylitis/Axial SpA. Rheumatology 2014; 53 (suppl_1): i16,https://doi.org/10.1093/rheumatology/keu068.002.
Sieper J, Braun J, Rudwaleit M, Boonen A, Zink A. Ankylosing spondylitis: an overview. Annals of the Rheumatic Diseases 2002;61(Suppl 3):iii8-iii18.
Rudwaleit M, van der Heijde D, Khan MA, Braun J, Sieper J. How to diagnose axial spondyloarthritis early. Ann Rheum Dis. 2004;63(5):535–43.
Deodhar A, Mittal M, Reilly P, et al. Ankylosing spondylitis diagnosis in US patients with back pain: identifying providers involved and factors associated with rheumatology referral delay. Clin Rheumatol. 2016;35(7):1769–76.
Danve A, Deodhar A. Axial spondyloarthritis in the USA: diagnostic challenges and missed opportunities. Clin Rheumatol. 2019;38:625–34.
Rimer BK, Glassman B. Tailoring communications for primary care settings. Meth Inform Med. 1998;37:1–6.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57.
Harris PA, Taylor T, Thielke T, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
Borkan J. Immersion/crystallization. In: Crabtree B, Miller W, editors. Doing qualitative research. 2nd ed. Thousand Oaks: Sage Publications; 1999. p. 179–94.
QSR NVivo. QSR international Pty ltd., Melbourne, Australia, 2000.
Sykes MP, Doll H, Sengupta R, Gaffney K. Delay to diagnosis in axial spondyloarthritis: are we improving in the UK? Rheumatology. 2015;54:2283–4.
Waddell G, Burton AK. Occupational health guidelines for the management of lower back pain at work: evidence review. Occup Med. 2001;51:124–35.
Mau W, Zeidler, Mau R, Majewski A, Freyschmidt J, Stangel W, et al. Clinical features and prognosis of patients with possible ankylosing spondylitis. Results of a 10-year followup. J Rheumatol 1988;15(7):1109–1114.
Vangeli E, Bakhshi S, Baker A, et al. A systematic review of factors associated with non-adherence to treatment for immune-mediated inflammatory diseases. Adv Ther. 2015;32(11):983–1028.
Suarez-Almazor ME. Patient-physician communication. Curr Opin Rheumatol. 2004;16(2):91–5.
Tai-Seale M, McGuire TG, Zhang W. Time allocation in primary care office visits. Health Serv Res. 2007;42(5):1871–94.
NCHS, National Ambulatory Medical Care Survey, 2016. Table 14.
Zhao SS, Radner H, Siebert S, et al. Comorbidity burden in axial spondyloarthritis: a cluster analysis. Rheumatology. 2019;58(10):1746–54.
Lubrano E, De Socio A, Perrotta FM. Unmet needs in axial Spondyloarthritis. Clinic Rev Allerg Immunol. 2018;55:332–9.
Rudwaleit M, Sieper J. Referral strategies for early diagnosis of axial spondyloarthritis. Nat Rev Rheumatol. 2012;8:262–8.
Graydon SL, Thompson AE. Triage of referrals to an outpatient rheumatology clinic: analysis of referral information and triage. J Rheumatol. 2008;35(7):1378–83.
Pincus T, Gibofsky A, Weinblatt ME. Urgent care and tight control of rheumatoid arthritis as in diabetes and hypertension: better treatments but a shortage of rheumatologists. Arthritis Rheum. 2002;46:851–4.
Deal CL, Hooker R, Harrington T, Birnbaum N, Hogan P, Bouchery E, Klein-Gitelman M, Barr W. The United States rheumatology workforce: supply and demand, 2005-2025. Arthritis Rheum. 2007;56(3):722–9.
https://www.rheumatology.org/Portals/0/Files/ACR-Health-Policy-Statements.pdf, Accessed 1 Mar 2020.
Schmajuk G, Tonner C, Yazdany J. Factors associated with access to rheumatologists for Medicare patients. Semin Arthritis Rheum. 2016;45(4):511–8.
Acknowledgements
We thank the primary care physicians who participated in this study. We also thank Jina Park and Katarina Ferrucci for their assistance with this project.
Funding
Funding for this project was provided by Novartis Pharmaceuticals Corporation. Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1TR000161. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. This work was also supported by a charitable contribution to the UMass Memorial Foundation from Timothy S. and Elaine L. Peterson.
Author information
Authors and Affiliations
Contributions
CD, SL, JK, EY designed the study. KL, SL, DS conducted the interviews. DS, AB, SK analyzed the data. All contributed to the interpretation of the data analysis. KL and SK wrote the first draft. All authors provided critical contributions during the revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the University of Massachusetts Medical School Institutional Review Board. All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
Dr. Lapane has served as a consultant to Barbara Zorowitz periodically to review prescribing guideline in post-acute settings for Empirian. Dr. Kay has served as a consultant to pharmaceutical companies. Dr. Yi is an employee of Novartis.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix A
Appendix B
Appendix C
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lapane, K.L., Khan, S., Shridharmurthy, D. et al. Primary care physician perspectives on barriers to diagnosing axial Spondyloarthritis: a qualitative study. BMC Fam Pract 21, 204 (2020). https://doi.org/10.1186/s12875-020-01274-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-020-01274-y