
Abstract
Background
Cigarette smoking harms nearly every organ, including the heart and lungs. A comprehensive assessment of both cardiac and respiratory function is necessary for evaluating the direct effects of tobacco on the heart. However, few previous studies examining the effects of cigarette smoking on cardiac function included an assessment of lung function. This cross-sectional study investigated the influence of cigarette smoking on cardiac function, independent of respiratory function.
Methods
We retrospectively reviewed the medical records of 184 consecutive cases that underwent both spirometry and transthoracic echocardiography around the same time (within 1 month) in one hospital from April 2019 to March 2020. Participants were classified into three groups based on lifetime smoking exposure (pack-years): non-smoker (n = 49), low exposure (1–20 pack-years, n = 40), and high exposure (≥ 20 pack years, n = 95). Multiple linear regression analysis was used to assess the relationship among cigarette smoking, and cardiac and respiratory functions. The relationship between selected dependent variables and lifetime pack-years was assessed in two models with multiple linear regression analysis. Model 1 was adjusted for age and male sex; and Model 2 was adjusted for Model 1 plus forced expiratory volume percentage in 1 s and forced vital capacity percentage.
Results
Compared with the non-smokers, the participants with high smoking exposure had lower left ventricular (LV) systolic function and larger LV size. Multiple linear regression analysis revealed a negative association of cumulative lifetime pack-years with LV and right ventricular (RV) systolic functions, even after adjustment for age, sex, and spirometric parameters (forced expiratory volume percentage in 1 s and forced vital capacity percentage). Meanwhile, there was no significant association of smoking exposure with LV diastolic function (E/e′ and E/A) and RV diastolic function (e′t and e′t/a′t).
Conclusions
Cumulative smoking exposure was associated with a negative effect on biventricular systolic function in patients with relatively preserved cardiac function, independent of respiratory function.
Similar content being viewed by others

Background
Cigarette smoking is well established as a major cause of cardiovascular disease [1,2,3]. Smoking is not only a risk factor for coronary artery disease, but also for heart failure [4]. Although several studies have evaluated the relationship between cigarette smoking and cardiac function, their results were inconsistent [5, 6]. Nonetheless, cigarette smoking has a known negative effect on lung function [7, 8]. There is a close relationship between lung and heart function. In addition, even subclinical impairment of respiratory function has been reported to be associated with cardiac dysfunction [9]. A comprehensive assessment of both cardiac and respiratory function is important for investigating the direct effects of tobacco use on the heart. However, few previous studies examining the effects of cigarette smoking on cardiac function included an assessment of lung function. Therefore, we investigated the cross-sectional association between cigarette smoking and cardiac function independent of respiratory function in individuals who underwent simultaneous echocardiography and spirometry.
Methods
This single-hospital retrospective observational study was conducted at Hitachiomiya Saiseikai Hospital. We reviewed the medical records of all consecutive cases that underwent both spirometry and transthoracic echocardiography around the same time (within one month) in our hospital from April 2019 to March 2020. The exclusion criteria were: (1) severe valvular disease (defined and diagnosed according to the guidelines of the American Society of Echocardiography [10,11,12]) or a history of valvular surgery or cardiac surgery, (2) a clinically evident history of lung disease and/or an abnormal finding of the lung field on imaging, (3) a history of ischemic heart disease (i.e., acute myocardial infarction and/or prevalence of local wall abnormality), (4) a participant with acute disease at examination by echocardiography and/or spirometry, (5) atrial fibrillation at examination with electrocardiogram, and (6) left ventricular ejection fraction (LVEF) ≤ 40%. This study was approved by our Institutional Review Board (ID 20-02), and it was carried out in accordance with the Declaration of Helsinki for experiments involving humans. The requirement for written informed consent was waived due to the retrospective nature of the study by our Institutional Review Board.
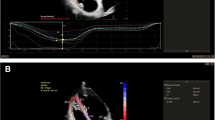
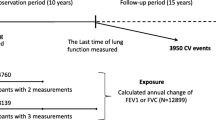
In echocardiography, data acquisition was performed by one of the expert sonographers using an EPICcv (Philips Medical Systems, Andover, MA, USA), equipped with a 5-MHz transducer, according to the established guidelines [10,11,12,13,14,15]. Echocardiography was generally performed without acute smoking exposure. Echocardiographically measured and derived variables were determined as follows: left ventricular mass (LVM) was calculated from left ventricular (LV) chamber size and wall thickness dimensions; 2-dimentional LVEF was computed from LV end-diastolic and end-systolic volumes which were calculated according to the bi-plane disk summation method in apical four- and two-chamber views; pulsed-wave Doppler was performed with the sample volume placed at the level of the mitral leaflet tips to obtain peak early (E) and late (A) diastolic transmitral inflow velocities and E-wave deceleration time; and tissue Doppler was performed to acquire mitral early (e′) and late (a′) diastolic annular velocities on the lateral side of the wall. To assess LV diastolic function, we used E/A ratio and E/e′ ratio. Right ventricular (RV) end-diastolic area was measured from an RV-focused apical four-chamber view. Right ventricular fractional area change (RVFAC), tricuspid annular plane systolic excursion (TAPSE), and RV peak systolic tissue Doppler velocity captured different dimensions of RV systolic function. RVFAC was obtained by tracing the RV endocardium from the annulus, along the free wall to the apex, back to the apex, then along the interventricular septum. To evaluate the RV diastolic function, tissue Doppler parameters were used: early diastolic peak velocity (e′t), late diastolic peak velocity (a′t) of the tricuspid annulus, and its ratio (e′t/a′t). Strain analyses were performed using a semi-automated speckle tracking technique (aCMQ, QLAB Cardiac Analysis, Philips Medical Systems, Andover, MA, USA). Three apical views were used to obtain an average global peak systolic longitudinal strain (GLS) with systole (Additional file 1: Figure 1).
The patients’ medical records were carefully reviewed in order to obtain information about their smoking history. In the instances where information on smoking status was lacking, they were interviewed directly. Cumulative smoking exposure was determined in terms of pack-years by multiplying the number of years the participant has smoked by the average number of packs per day [16]. We divided the participants into three groups according to the cumulative lifetime smoking exposure: non-smoker group including the participants who had never smoked a cigarette or other tobacco products before, low exposure group (1–20 pack-years), and high exposure group (≥ 20 pack years) [17]. Hypertension was defined as using medical treatment for hypertension and/or a history of hypertension before admission. Dyslipidemia was defined as triglyceride level ≥ 150 mg/dl, low-density lipoprotein cholesterol level ≥ 140 mg/dl, high-density lipoprotein cholesterol level ≤ 40 mg/dl, using medical treatment for dyslipidemia, or a history of dyslipidemia. Diabetes mellitus was defined as hemoglobin A1c level ≥ 6.5% (as National Glycohemoglobin Standardization Program value), using medical treatment for diabetes mellitus, or a history of diabetes mellitus. We calculated the estimated glomerular filtration rate (eGFR) from serum creatinine levels, age, weight, and gender using the following formula; eGFR (ml/min/1.73 m2) = 194 × s-Cr (− 1.094) × age (− 0.287) × 0.739 (if female) [18].. Chronic obstructive pulmonary disease (COPD) was defined as post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) < 0.70, which confirms the presence of persistent airflow limitation on spirometry or a history of medication [19].
Methods for measurement of spirometric parameters
The Berglund equation was used to predict FEV1.0 according to the following calculations: FEV1.0 (L) in males = 3.44 × height (m) – 0.033 × age − 1; FEV1.0 (L) in females = 2.67 × height (m) − 0.027 × age − 0.5 [20, 21]. The forced expiratory volume percentage in one second (FEV1.0%) = measured FEV1.0/measured FVC. The percent predicted forced expiratory volume in one second (%FEV1.0) = measured FEV1.0/predicted FEV1.0. The Baldwin equation was used to predict VC and FVC as follows: VC (L) in males = (27.63 – 0.0112 × age) × height (m); VC (L) in females = (21.78 – 0.101 × age) × height (m). The vital capacity percentage = measured VC/predicted VC [20, 21]. The percent predicted forced vital capacity = measured FVC/predicted FVC. Spirometry was performed with MICROSPIRO HI-80 (NIHON KODEN, JAPAN).
Statistical analysis
The normality was tested with the Shapiro–Wilk test. Continuous data are expressed as mean ± standard deviation (SD) for normally distributed variables and median [25th–75th percentile] for non-normally distributed variables. Normally distributed continuous variables were compared between the groups using a one-way analysis of variance (ANOVA) with a post hoc analysis with Tukey test or Games–Howell test. Non-normally distributed continuous variables were compared using a Kruskal–Wallis test with a post hoc analysis with Dann-Bonferroni method. Categorical variables are expressed as numbers (percentage) and were compared using Pearson’s χ2 test or Fisher’s exact test.
Multiple linear regression analysis was used to assess the relationship among cigarette smoking, and cardiac and respiratory functions. Dependent variables were selected from variables that could indicate the ventricular systolic and diastolic function on echocardiography as follows: LVEF, E/e′, E/A, RVFAC, e′t, and e′t/a′t. We assessed the relationship between the selected dependent variables and the lifetime pack-years in two models with a multiple linear regression analysis. First, Model 1 was adjusted for age and male sex; and Model 2 was adjusted for Model 1 plus FEV1.0% and forced vital capacity percentage (%FVC). Age and sex were selected as independent variables because they were well-known parameters which could affect the cardiac function. Meanwhile, FEV1.0% and %FVC were selected as independent variables because they were important parameters on spirometry that could clearly indicate respiratory condition [22]. Beta coefficients were interpreted as the absolute change in dependent variables per change in the pack-years intensity. A p value < 0.05 was considered statistically significant. All analyses were performed using statistical software, SPSS 26.0/Windows (SPSS, Chicago, IL).
Results
The final study population included 184 subjects (69.6% men, mean age: 70.1 ± 13.3 years old), divided into the following three groups: non-smoker group (n = 49), low smoking exposure group (n = 40), and high smoking exposure group (n = 95). Table 1 shows a comparison of clinical characteristics among the three groups. Non-smokers were significantly older, more likely to be women, and had higher cardio-thoracic ratio compared with the other two groups. The individuals with high smoking exposure were older and more likely to be men compared with those in the low exposure group. Meanwhile, body mass index was comparable among the three groups and within normal range.
Table 2 shows the comparison of cardiac function by echocardiography among the three groups. When compared with non-smokers, the participants with high smoking exposure had lower LVEF; larger LV dimension and LV volume; slower A wave velocity; higher E/A; larger RV area and tricuspid valve annular diameter; and higher e′t/a′t. The participants with low smoking exposure had larger LV dimension and LV volume; slower A wave velocity; higher E/A, larger RV area; higher e′t/a′t; and a larger inferior vena cava. There were no significant differences in echocardiographic parameters between the low and high exposure groups. The comparison of respiratory function by spirometry among the three groups is shown in Additional file 2: Table 1. Overall, non-smokers had better respiratory function than the participants with any smoking exposure. The degree of FEV1.0, FVC, and vital capacity (VC) were significantly lower in the non-smoker group than in the smoking exposure groups. Meanwhile, the degree of FEV1.0% and %FEV1.0 were significantly better in the non-smoker group than in the smoking exposure groups.
Table 3 presents the association between lifetime pack-years and cardiac function. The LVEF, RVFAC, and parameters of ventricular systolic function were negatively correlated with the number of lifetime pack-years. The LV end-systolic volume index, RV end-systolic area index, and parameters of end-systolic ventricular volume were positively associated with the pack-years intensity. The E/A, E/e′, e′t, e′t/a′t, and parameters of ventricular diastolic function were not associated with the number of pack-years. The respiratory parameter regarding airflow limitation, such as FEV1.0% and %FEV1.0, were negatively associated with the increasing number of lifetime pack-years (Additional file 2: Table 2).
Table 4 shows the effect of lifetime pack-years on ventricular systolic and diastolic function. There was a negative association between cumulative lifetime pack-years and left and right ventricular systolic functions (LVEF and RVFAC, respectively), even after adjustment for age, sex, FEV1.0%, and %FVC (Table 4); this suggests that cigarette smoking could cause biventricular systolic dysfunction independent of respiratory function. Meanwhile, there was no significant association between the lifetime pack-years and LV diastolic function (E/e′ and E/A), RV diastolic function (e′t and e′t/a′t), or other echocardiographic parameters, except for tricuspid valve annular diameter (Table 4 and Additional file 2: Table 3).
Discussion
There were two main findings of the present study: (1) the individuals with high smoking exposure had lower LV systolic function and larger LV size; and (2) the dose of lifetime cumulative smoking exposure was significantly associated with worse LV and RV systolic function independent of respiratory function. These findings reveal that cigarette smoking exposure may result in the development of cardiac dysfunction in a direct and continuous dose-dependent fashion and thus, may contribute to the heart failure epidemic.
There were several previous studies regarding the relationship between smoking exposure and worsening cardiac function [1, 6, 23,24,25]. Specifically, some studies reported that LV mass index could increase with higher exposure to smoking [5, 6]. However, in the present study, the lifetime smoking exposure had no significant association with LV mass index. Meanwhile, one previous study showed that cigarette smoking was closely related to low LV mass index [26]. One explanation was that LV mass index was reported to have an association with several factors including age, body weight, height, physical activity, and blood pressure [26]. The biased effect of the participants’ background in the present study might have affected the relationship between smoking exposure and LV mass index. In particular, the patients in the present study had evidently lower BMI compared with the previous studies [5, 6], which might have affected the ventricular morphology including LV mass index. Therefore, the result of LV mass index should also be carefully interpreted taking the participants’ background into consideration. Furthermore, the implication of the present study was to investigate the association between smoking exposure and cardiac function while considering respiratory function. Although the effects of respiratory function against cardiac function have already been reported [27,28,29], there were few studies investigating the relationship between smoking exposure and cardiac function, after adjusting for respiratory function. In the present study, the higher the participants’ smoking exposure, the larger the values of FVC and VC. Conversely, the cardio-thoracic ratio of the patients with smoking exposure was lower than that of the non-smoker patients, which could suggest the impact of the effects of smoking exposure on lung expansion. A previous study also reported that patients with severe emphysema had significantly lower stroke volume index and LV end-diastolic area index [30]. Although the interaction between heart and lung was observed (even in the present study), the present study showed that cumulative smoking exposure could be significantly related to worse LV and RV systolic function independent of respiratory function.
Cigarette smoking could have serious effects on the systemic function, especially cardiac and respiratory functions. Several mechanisms regarding smoking exposure and cardiovascular dysfunction have been suggested previously. In animal models, cigarette smoking has been shown to induce ventricular hypertrophy and remodeling with increased serum levels of norepinephrine [6]. Continuous exposure to smoking could stimulate the autonomic nervous system and induce cardiac remodeling [6]. These injury models would have effects on the RV function as well as the LV function [6]. Furthermore, cigarette smoking could cause subclinical cardiovascular damage [31]. This damage could be associated with increased blood pressures causing ventricular enlargement as well as LV systolic and diastolic dysfunction [6]. Smoking-related micro-alterations would increase myocardial oxygen demand, making the heart more susceptible to microvascular ischemic damage, which could be related to LV abnormality [6, 32]. In addition, increased sympathetic stimulation via nicotine, carbon monoxide exposure, endothelial dysfunction, direct cellular damage, and oxidative stress were considered as factors contributing to several mechanisms of cardiovascular dysfunction [6, 33, 34]. As mentioned above, cigarette smoking could result in negative effects on cardiovascular function with several mechanisms. However, the present study could not detect the worse effect of smoking exposure against cardiac diastolic function. A previous study also reported an inconclusive association between smoking exposure and cardiac diastolic function owing to the difficulty in obtaining and measuring the data on diastolic function and the effect of other confounding factors [35]. The incomplete measurement of cardiac diastolic function and small sample size might make the results indefinite in the present study. Based on the discussion, although the present study included patients with relatively well-preserved cardiac function, cigarette smoking might have a worse impact on cardiac systolic function independent of respiratory function.
The study has several limitations. First, since this study was a single-center retrospective observational study, there is a risk of selection bias. The study also had a relatively small sample size that was adjusted for variables such as age, sex and respiratory function. Therefore, we were unable to investigate whether other factor would be associated with cardiac function. The participants’ background such as age and sex were heterogeneous among the three groups. It is well known that sex was directly associated with cardiac morphology including left and right ventricular volume and area [15]. Therefore, multiple linear regression analysis included age and male sex as well as respiratory parameters and lifetime pack-years. Furthermore, age in the multiple linear regression analysis might have been a confounding factor because the non-smokers were evidently older than those in the other groups, and their cardiac function was relatively better, regardless of their old age. Second, although the present study showed that ventricular diastolic dysfunction might not be affected by cumulative smoking exposure, several parameters regarding LV and RV diastolic function were unmeasured. Therefore, the results should be carefully interpreted considering the notable relationship between diastolic function and smoking exposure. Third, the present study excluded patients with a known history of ischemic heart disease; however, we could not completely eliminate the impact of atherosclerotic disease. Fourth, the patients’ medical records lacked information about alcohol and/or caffeine exposure which has the potential to affect the echocardiographic measurement results. Furthermore, it was difficult to accurately track and measure changes in the patients’ smoking status over a long period of time, which may have influenced the results. Fifth, LV and RV global longitudinal strain had about 10% of missing values and furthermore the study population was relatively small. Therefore, there might be discrepancies between the LVEF, right ventricular fractional area change and global longitudinal strain. Finally, the present study was observational in nature, and our findings that smoking exposure could have a negative impact on cardiac function independent of lung function need to be confirmed with a larger population-based cohort study.
Conclusions
Cigarette smoking could be attributed to the worsening of systemic functions, especially cardiac and respiratory functions directly. In all models, the biventricular systolic function was mildly influenced by cumulative smoking exposure. Therefore, there was a negative effect of smoking exposure on the biventricular systolic function in patients with relatively well-preserved cardiac function independent of respiratory function.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due the study dataset contains potentially identifying clinical information but are available from the corresponding author on reasonable request.
Abbreviations
- A:
-
Late diastolic transmitral inflow peak velocity
- ANOVA:
-
Analysis of variance
- a′:
-
Mitral late diastolic annular peak velocity
- a′t:
-
Late diastolic peak velocity of the tricuspid annular velocity
- COPD:
-
Chronic obstructive pulmonary disease
- E:
-
Early diastolic transmitral inflow peak velocity
- eGFR:
-
Estimated glomerular filtration rate
- e′:
-
Mitral early diastolic annular peak velocity.
- e′t:
-
Early diastolic peak velocity of the tricuspid annular velocity
- FEV1.0:
-
Forced expiratory volume in one second
- FVC:
-
Forced vital capacity
- LV:
-
Left ventricular
- LVEF:
-
Left ventricular ejection fraction
- LVN:
-
Left ventricular mass
- RV:
-
Right ventricular
- RVFAC:
-
Right ventricular fractional area change
- SD:
-
Standard deviation
- TAPSE:
-
Tricuspid annular plane systolic excursion
- VC:
-
Vital capacity
References
Virdis A, Giannarelli C, Neves MF, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Curr Pharm Des. 2010;16:2518–25.
Kamimura D, Cain LR, Mentz RJ, White WB, Blaha MJ, DeFilippis AP, et al. Cigarette smoking and incident heart failure: Insights from the Jackson Heart Study. Circulation. 2018;137:2572–82.
Cigarette smoking and health. American Thoracic Society. Am J Respir Crit Care Med. 1996;153:861–5
Yang H, Negishi K, Otahal P, Marwick TH. Clinical prediction of incident heart failure risk: a systematic review and meta-analysis. Open Heart. 2015;10:e000222.
Nadruz W Jr, Claggett B, Gonçalves A, Querejeta-Roca G, Fernandes-Silva MM, Shah AM, et al. Smoking and cardiac structure and function in the elderly: the ARIC Study (Atherosclerosis Risk in Communities). Circ Cardiovasc Imaging. 2016;9:e004950.
Leigh JA, Kaplan RC, Swett K, Balfour P, Kansal MM, Talavera GA, et al. Smoking intensity and duration is associated with cardiac structure and function: the ECHOcardiographic study of hispanics/latinos. Open Heart. 2017;4:e000614.
Fukuchi Y, Nishimura M, Ichinose M, Adachi M, Nagai A, Kuriyama T, et al. COPD in Japan: the Nippon COPD Epidemiology study. Respirology. 2004;9:458–65.
Tantisuwat A, Thaveeratitham P. Effects of smoking on chest expansion, lung function, and respiratory muscle strength of youths. J Phys Ther Sci. 2014;26:167–70.
Baum C, Ojeda FM, Wild PS, Rzayeva N, Zeller T, Sinning CR, et al. Subclinical impairment of lung function is related to mild cardiac dysfunction and manifest heart failure in the general population. Int J Cardiol. 2016;218:298–304.
Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009;22:101–2.
Baumgartner H, Hung J, Bermejo J, Chambers JB, Edvardsen T, Goldstein S, et al. Recommendations on the echocardiographic assessment of aortic valve stenosis: a focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J Am Soc Echocardiogr. 2017;30:372–92.
Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, et al. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American Society of Echocardiography developed in collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr. 2017;30:303–71.
Nagueh SF, Smiseth OA, Appleton CP, Byrd BF 3rd, Dokainish H, Edvardsen T, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2016;29:277–314.
Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23:685–713.
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28:1–39.e14.
Lynch SM, Vrieling A, Lubin JH, Kraft P, Mendelsohn JB, Hartge P, et al. Cigarette smoking and pancreatic cancer: a pooled analysis from the pancreatic cancer cohort consortium. Am J Epidemiol. 2009;170:403–13.
Neumann T, Rasmussen M, Heitmann BL, Tønnesen H. Gold standard program for heavy smokers in a real-life setting. Int J Environ Res Public Health. 2013;10:4186–99.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195:557–82.
Berglund E, Birath G, Bjure J, Grimby G, Kjellmer I, Sandqvist L, et al. Spirometric studies in normal subjects I. Forced expirograms in subjects between 7 and 70 years of age. Acta Med Scand. 1963;173:185–92.
Baldwin ED, Cournand A, Richards DW. Pulmonary insufficiency; physiological classification, clinical methods of analysis, standard values in normal subjects. Medicine. 1948;27:243–78.
Sperandio EF, Arantes RL, Matheus AC, Silva RP, Lauria VT, Romiti M, et al. Restrictive pattern on spirometry: association with cardiovascular risk and level of physical activity in asymptomatic adults. J Bras Pneumol. 2016;42:22–8.
Yaman B, Akpınar O, Cerit L, Kemal HS, Usalp S, Yüksek Ü, et al. Effects of chronic cigarette smoking on myocardial deformation parameters by two-dimensional speckle tracking echocardiography. Echocardiography. 2019;36:2026–32.
Batista ANR, Garcia T, Franco EAT, Azevedo PS, Barbosa MF, Zornoff LAM, et al. Comparison of morphometry and ventricular function of healthy and smoking young people. BMC Cardiovasc Disord. 2020;20:66.
Farsalinos KE, Tsiapras D, Kyrzopoulos S, Savvopoulou M, Voudris V. Acute effects of using an electronic nicotine-delivery device (electronic cigarette) on myocardial function: comparison with the effects of regular cigarettes. BMC Cardiovasc Disord. 2014;14:78.
Payne JR, James LE, Eleftheriou KI, Hawe E, Mann J, Stronge A, et al. The association of left ventricular mass with blood pressure, cigarette smoking and alcohol consumption; data from the LARGE Heart study. Int J Cardiol. 2007;120:52–8.
Jankowich M, Elston B, Liu Q, Abbasi S, Wu WC, Blackshear C, et al. Restrictive spirometry pattern, cardiac structure and function, and incident heart failure in African Americans. The Jackson Heart Study. Ann Am Thorac Soc. 2018;15:1186–96.
Tavazzi G, Bergsland N, Alcada J, Price S. Early signs of right ventricular systolic and diastolic dysfunction in acute severe respiratory failure: The importance of diastolic restrictive pattern. Eur Heart J Acute Cardiovasc Care. 2019. https://doi.org/10.1177/2048872619883399.
Hilde JM, Skjørten I, Grøtta OJ, Hansteen V, Melsom MN, Hisdal J, et al. Right ventricular dysfunction and remodeling in chronic obstructive pulmonary disease without pulmonary hypertension. J Am Coll Cardiol. 2013;62:1103–11.
Jörgensen K, Houltz E, Westfelt U, Ricksten SE. Left ventricular performance and dimensions in patients with severe emphysema. Anesth Analg. 2007;104:887–92.
Lederer DJ, Enright PL, Kawut SM, Hoffman EA, Hunninghake G, van Beek EJ, et al. Cigarette smoking is associated with subclinical parenchymal lung disease: The Multi-Ethnic Study of Atherosclerosis (MESA)-lung study. Am J Respir Crit Care Med. 2009;180:407–14.
Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease: an update. J Am Coll Cardiol. 2004;43:1731–7.
Zhou X, Li C, Xu W, Chen J. Protective effects of valsartan against cigarette smoke-induced left ventricular systolic dysfunction in rats. Int J Cardiol. 2013;167:677–80.
Biondi-Zoccai G, Sciarretta S, Bullen C, Nocella C, Violi F, Loffredo L, et al. Acute effects of heat-not-burn, electronic vaping, and traditional tobacco combustion cigarettes: The Sapienza University of Rome-Vascular Assessment of Proatherosclerotic Effects of Smoking (SUR-VAPES) 2 Randomized Trial. J Am Heart Assoc. 2019;8:e010455.
Kraen M, Frantz S, Nihlén U, Engström G, Löfdahl CG, Wollmer P, et al. Echocardiographic consequences of smoking status in middle-aged subjects. Echocardiography. 2017;34:14–9.
Acknowledgements
We are grateful for the support of the entire staff of the clinical laboratory department in Hitachiomiya Saiseikai Hospital.
Funding
None.
Author information
Authors and Affiliations
Contributions
YW: Conceptualization, Methodology, Original draft preparation, Writing. KT: Editing, Supervision, Reviewing Writing. AS: Data curation, Investigation. HN: Supervision and Editing. MK: Supervision and Reviewing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Hitachiomiya Saiseikai Hospital (ID 20-02), and it was carried out in accordance with the Declaration of Helsinki for experiments involving humans. The requirement for written informed consent was waived due to the retrospective nature of the study by our Institutional Review Board.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Figure 1
. A representative of strain analyses using a semi-automated speckle tracking technique. The three apical views were used to obtain an average global peak systolic longitudinal strain with systole. Figures a, b and c are the apical long axis, 2-, 3- and 4-chamber views, respectively. Figure d shows the Bull’s eye plot of left ventricular global longitudinal strain assessed by speckle tracking technique.
Additional file 2: Supplementary Table 1
. Spirometric parameters of the participants according to smoking exposure. Supplementary Table 2. Correlation among lifetime pack-years and spirometric parameters. Supplementary Table 3. Effect of lifetime pack-years on echocardiographic parameters.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Watanabe, Y., Tajiri, K., Suzuki, A. et al. Influence of cigarette smoking on biventricular systolic function independent of respiratory function: a cross-sectional study. BMC Cardiovasc Disord 20, 451 (2020). https://doi.org/10.1186/s12872-020-01732-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-020-01732-6