
Abstract
Objective
This study aimed to assess the association between exposure to the Great Chinese Famine (1959–1961) during early life and hypertension in adulthood.
Methods
From July to September 2009, 1224 eligible adults were recruited in a cross-sectional survey using a multi-stage stratified random sampling method in Chongqing China. A questionnaire was used to collect information of hypertension and sociodemographic factors. Participants were categorized as childhood, fetal, and none exposure to famine based on the date of birth.
Results
Of the sample, 12.3% reported having hypertension. The prevalence of hypertension varied by famine status: 11.9% in childhood exposure, 16.1% in fetal exposure, and 10.2% in non-exposure group. After adjusting for sociodemographic and lifestyle factors, compared with non-exposure group, fetal exposure group had an increased likelihood of having hypertension with odds ratio of 1.79 (95%CI 1.13-2.84). Although there was no significant gender and famine interaction, the positive association between famine exposure and hypertension was stronger among women than men.
Conclusion
Fetal exposure to the Chinese famine may be associated with an increased risk of arthritis in adulthood in women.
Similar content being viewed by others


Background
Hypertension is one of the most important risk factors of cardiovascular diseases as well as other chronic diseases. Hypertension causes a significant burden to the families and the [1]. According to the 2015 China Health and Family Planning Statistical Yearbook, the prevalence of hypertension among adults in China increased from 25.0% in 2002 to 38% in 2012 [2]. Among adults aged above 60 years, 58.9% had hypertension in 2012 [3]. On the contrary, among adults aged 45 to 59 years the prevalence of control, treatment and awareness of hypertension was only 13.1%, 38.0% and 44.2%, respectively [3]. The direct medical cost of hypertension was estimated to be 5.7 billion dollars in 2005 in China [4]. In addition to the known risk factors of hypertension (e.g. aging, smoking, obesity, alcohol drinking, lack of physical activity and poor quality of diet), early life malnutrition may also affect hypertension.
Previous research suggests that the risk factors of chronic diseases in adulthood may originate from adverse exposures or undernutrition during fetal period [5, 6]. The Great Chinese Famine of 1959–1961 is the most extensive in human history leading to approximately over 30 million deaths [7, 8]. Emerging evidence suggests that exposure to Chinese famine in early life is related to increased risk of diabetes [9], short height [10], metabolic syndrome [5], and weight gain [11] among adults. However, the findings are criticized by a recent review as most of the findings from the published Chinese famine studies may be confounded by age [12]. Thus, there is a need to explore the association with a robust methodology.
The gender difference of hypertension in the general population is well documented but the cause is not fully understood [13]. A recent study demonstrates that women exposed to famine during fetal stage and infancy had a higher mean systolic blood pressure than those did not expose to the famine [14]. However, this finding has not been validated by other studies.
It has hypothesized that the recent rapid increase of chronic disease in China may be due to the Chinese famine in 1959–1961 [15]. As the people born during the Chinese famine are at their 50’s, a better understanding of the link between famine exposure in early life and hypertension among adults is warranted in order to manage and prevent the high burden of NCDs in China. Thus, this study aimed to assess the association of famine exposure in early life and hypertension in middle-aged population. Following the review by Li C and Lumey LH [12], we aimed to address the age related confounding by comparing fetal/infant exposure with non-exposure/childhood exposure.
Methods
Study design and participants
The study was conducted in Chongqing City in July 2009. A three-stage stratified random sampling method was used to recruit participants. Eligible participants were those born between 1956 and 1964 and were aged 45–53 years during time of the survey. At stage 1, 10 districts and counties were randomly selected in Chongqing City. Stage 2 involved listing eligible villages within the selected districts and counties. Approximately 8–10 villages were selected (stage 2) in each selected district/county, and 10–15 participants were randomly selected in each village (stage 3). In total, 1250 participated in the survey with a response rate of 98.4%. Of the 1250 participants, owing to missing data, six were excluded in the analysis. Detailed descriptions of the study design and methods were previously reported [16]. The study protocol was approved by the Ethics Committee of Chongqing Medical University, and its methods were carried out in accordance with the approved current guidelines. Written informed consent was obtained from all participants. All subjects were Chongqing residents who were born in 1956–1964.
Instrument
A questionnaire survey was employed to interview people who experienced famine and were born in a specific situation of nutritional health and quality of life. The questionnaire was divided into two sections.
Sociodemographic factors
The first section determined the general basic information of the participants, including their gender. We collected their self-reported height and weight to calculate BMI. The education level was categorized as ≤ primary school, junior middle school (basic education), ≥ senior high school (including vocational/technical secondary school and junior college), secondary education, and ≥ senior college and university (higher education). Job conditions were categorized as unemployed, employed, and stay at home, feeding procedure, and marital status was categorized as unmarried, married or cohabitation, divorce or separated, and widowed. The average monthly income was categorized as low (<¥850), medium (¥850– ¥1600) and high (>¥1601) (1 USD = ¥ 6.86 in February 2017).
Lifestyle factors
Smoking status and alcohol drinking were categorized as yes or no. Regular physical activity and regular daily life were categorized as seldom, sometimes, or often. Sleep status was categorized as good, average, or poor. Participants were classified into low weight, normal–overweight, and obesity–BMI groups as follows: low (BMI <18.5), normal (18.5 ≤ BMI <24), overweight (24 ≤ BMI <28), and obesity (BMI ≥28) [17].
Chinese famine exposure status
Participants were categorized into three groups based on their date of birth: (1) childhood exposure (1956–1958), (2) fetal exposure (1959–1961, 3) non-exposure: (1962–1964). Such classification was used in previous Chinese famine studies [11].
Outcome variable
Hypertension and other health conditions were assessed by the question “Have you ever been told by a doctor or other health professional that you have (disease or condition)?” [16].
Statistical analyses
Chi-square were used to compare differences between categorical variables. The association between famine exposure and hypertension was assessed using multivariable logistic regression. In addition to unadjusted model (model 1), two multivariable models were used. The first multivariable model adjusted for gender, education, smoking, and alcohol drinking, physical activity, sleep status, breast-feeding and diabetes. The second multivariable further adjusted for BMI. Odds ratio (OR) for hypertension was calculated for fetal exposure and childhood exposure group using non-exposure as reference group. As the non-exposure group was three years younger than the fetal group, to adjust for the potential age effect, we combined non-exposure and childhood exposure as reference group in the logistic regression to calculate the OR for hypertension among those fetal exposure group, similar to the one in International Journal of Epidemiology [12]. The statistical tests contained a two-sided test with the statistical significance set to p < 0.05. All data analyses were performed using statistical software (SAS version 9.1.3; SAS Institute, Cary, NC, USA).
Results
A total of 1224 eligible respondents participated in the study. Of the participants, 150 (12.3%) reported having hypertension. Significant differences were observed on gender (p < 0.001), marital status (p = 0.0440), smoking (p < 0.001), alcohol drinking (p < 0.001), and BMI (p < 0.001) between individuals with and without hypertension (Table 1).
Across famine exposure groups, there were significant differences on educational level (p < 0.001), job conditions (p < 0.001), average monthly income (p = 0.001), and feeding practice (p = 0.035) (Table 2). Fetal exposure group had the lowest rate of breast-feeding in early life (75.3%) as compared with childhood (81.1%) or non-exposure group (84.7%).
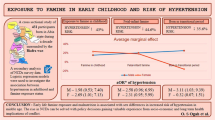
Fetal exposure to famine had the highest prevalence of self-reported hypertension. The prevalence of self-reported hypertension was 11.9% in childhood exposure group, 16.1% in fetal exposure group and 10.2% in non-exposure group, respectively. In multivariable logistic regression model adjusting for sociodemographic and lifestyle factors as well as BMI (model 3), compared with non-exposure group, fetal exposure group had 80% increased risk of hypertension (OR 1.79, 95% CI 1.13-2.84) (Table 3). The increased risk was seen in both genders although it was stronger in women (OR 2.34, 95% CI 1.01-5.42) than men (OR 1.67, 95% CI 0.95-2.92). Using non-exposure and childhood exposure as reference, fetal exposure group had an OR of 1.62 (95%CI 1.09-2.39) for hypertension. There was no significant increase of the likelihood of hypertension for the childhood exposure group as compared with non-exposure group.
Discussion
In this population-based study, we found that fetal exposure but not childhood exposure to Chinese famine was associated with an elevated risk of self-reported hypertension in women. The findings are partly in line with previous studies. Although the relationship between early life exposure to Dutch and Leningrad Siege famine and hypertension risk is inconclusive [18,19,21], several studies found a positive link. Several studies in China have shown a positive association between early life famine exposure and hypertension [6, 14, 22, 23]. However, these studies have been criticized by not being adjusted the effect of age [12]. Based on the meta-analysis, Chinese famine is not associated with elevated risk of hypertension. To address the potential age confounding, we combined childhood famine exposure and non-exposure as the reference group to assess the effect of fetal famine exposure. Our finding may suggest that fetal famine exposure is associated with an increased risk of hypertension in women. The China Health and Retirement Longitudinal Study (CHARLS) indicate that nearly 40% of the adults aged 45 years and above had hypertension [24]. However, more than 40% of hypertensive patients are unaware that they are suffered from hypertension [24].
The gender difference of early life famine exposure and hypertension in our study is consistent with other studies in China. For example, the China Health and Nutrition Survey 2002 indicated that the association between famine exposure and hypertension prevalence risk was seen only among women [14]. Exposure to famine during fetal stage or early childhood exerts greater deleterious effects on female adults than male ones [14], like worsen glucose and lipid metabolism [25]. Animal studies also indicate that malnutrition may exert more adverse effects in females than males [26]. The cause of the gender difference is unknown. It could be speculated that female may suffer more than males during the famine because of son preference culture in China. More quantitative studies of larger sample are needed to further examine the relationship between fetal famine exposure and risk of hypertension among different gender.
Our study shows significant differences of educational achievement, job status, income, and early life feeding practice according to famine exposure. Early life famine exposure was associated with a lower education, income than those unexposed. This phenomenon has been shown in previous studies [27]. Negative long-term effects of impaired fetal development are not only related to health but also to educational level, employment opportunities, and income [28, 29]. Socioeconomic status is known to be associated with hypertension. It may partly explain the association between fetal exposure to famine and hypertension among adults.
The beneficial effect of breastfeeding is well known. Breastfeeding in early life can reduce the risk of hypertension in adults [30]. In the fetal exposure to famine group, the prevalence of breastfeeding is lower than other group. This may also partly explain the increase of hypertension risk among those fetal exposures to famine.
This study bears certain limitations. First, the severity of famine exposure for each individual is not known. Potentially, not all respondents’ families were equally affected by the famine. Second, we used self-reported hypertension as outcome measure. The prevalence of awareness of hypertension is low in China. This may cause serious bias. Third, the sample size was relatively small and limits the power to conduct subgroup analyses. Fourth, the cross-sectional survey data hindered the researchers to determine direct causal inferences, explore if other factors may provide better explanations on the observed relationships, and determine the direction of causal relationship. Fifth, the study sample used in the investigation was relatively homogeneous regarding race/ethnicity. Future investigations with more heterogeneous samples are warranted. In our study, the prevalence of self-reported doctor diagnosed diabetes (1.88%) was much lower than the prevalence from the 2010 Chinese national study (~11.6%) [31]. It was also lower than the prevalence of diabetes from a local study in Chongqing (4.09%) [32]. Finally, this study did not include family history of hypertension, and we were not able to adjust for factors like diabetes and dyslipidemia.
Conclusions
Approximately 12.3% of the respondents self-reported their diagnoses of hypertension. This study suggests that fetal exposure to famine may be positively associated with hypertension in adulthood especially in women. More quantitative studies of larger sample are needed to further examine the association between fetal famine exposure and risk of hypertension among different gender.
Change history
15 March 2018
The ‘Conclusion’ section in the Abstract was published incorrectly in the original publication of the article [1] and is corrected with this erratum as below: “Fetal exposure to the Chinese famine may be associated with an increased risk of hypertension in adulthood in women.”
Abbreviations
- CI:
-
Confidence intervals
- OR:
-
Odds ratio
References
Zhang JT, Chen KP, Guan T, Zhang S. Effect of aliskiren on cardiovascular outcomes in patients with prehypertension: a meta-analysis of randomized controlled trials. Drug Des Devel Ther. 2015;9:1963–71. doi:10.2147/DDDT.S75111.eCllection.
World Health Organization. MEDIA CENTRE. Health conditions aggravate Southern Africa famine. See http://www.who.int/mediacentre/news/releases/who63/en.
Bureau of Disease Prevention and Control (Office of the National Patriotic Health Campaign Committee). 2015 report on Chinese resident’s chronic disease and nutrition. (People’s Medical Publishing House, 2015).
Hypertension Prevention Guide Revision Committee. Guidelines for prevention and control for hypertension in China (2005 revision). Chin J Hypertens. 132; 39 (2005).
Wang N, Wang X, Li Q, Han B, Chen Y, Zhu C, et al. The famine exposure in early life and metabolic syndrome in adulthood. Clin Nutr. 2015; doi:10.1016/j.clnu.2015.11.010.
Wang Z, Li C, Yang Z, Zou Z, Ma J. Infant exposure to Chinese famine increased the risk of hypertension in adulthood: results from the China Health and Retirement Longitudinal Study. BMC Public Health. 2016;16:435. doi:10.1186/s12889-016-3122-x.
Smil V. China’s great famine: 40 years later. BMJ. 1999;319(7225):1619–21.
Huang C, Guo C, Nichols C, Chen S, Martorell R. Elevated levels of protein in urine in adulthood after exposure to the Chinese famine of 1959–61 during gestation and the early postnatal period. Int J Epidemiol. 2014;43(6):1806–14. doi:10.1093/ije/dyu193. Epub 2014 Oct 8
Li Y, He Y, Qi L, Jaddoe VW, Feskens EJ, Yang X, et al. Exposure to the Chinese famine in early life and the risk of hyperglycemia and type 2 diabetes in adulthood. Diabetes. 2010;59(10):2400–6. doi:10.2337/db10-0385. Epub 2010 Jul 9
Chen Y, Zhou LA. The long-term health and economic consequences of the 1959-1961 famine in China. J Health Econ. 2007;26(4):659–81. doi:10.1016/j.jhealeco.2006.12.006. Epub 2007 Jan 11
Wang Y, Wang X, Kong Y, Zhang JH, Zeng Q. The Great Chinese Famine leads to shorter and overweight females in Chongqing Chinese population after 50 years. Obesity. 2010;18(3):588–92. doi:10.1038/oby.2009.296. Epub 2009 Sep 24
Li C, Lumey LH. Exposure to the Chinese famine of 1959-61 in early life and long-term health conditions: a systematic review and meta-analysis. Int J Epidemiol. 2017; doi:10.1093/ije/dyx013. [Epub ahead of print]
Everett B, Zajacova A. Gender differences in hypertension and hypertension awareness among young adults. Biodemography Soc Biol. 2015;61(1):1–17. doi:10.1080/19485565.2014.929488.
Chen H, Nembhard WN, Stockwell HG. Sex-specific effects of fetal exposure to the 1959-1961 Chinese famine on risk of adult hypertension. Matern Child Health J. 2014;18(3):527–33. doi:10.1007/s10995-013-1268-z.
Zimmet PZ. Diabetes and its drivers: the largest epidemic in human history? Clin Diabetes Endocrinol. 2017;3(1) doi:10.1186/s40842-016-0039-3.
Xu X, Rao Y, Shi Z, Liu L, Chen C, Zhao Y. Hypertension Impact on Health-Related Quality of Life: A Cross-Sectional Survey among Middle-Aged Adults in Chongqing, China. Int J Hypertens. 2016;7404957 doi:10.1155/2016/7404957. Epub 2016 Aug 17
National Health and Family Planning Commission of the People’s Republic of China. Criteria of weight for adults. Available at: http://www.moh.gov.cn/ewebeditor/uploadfile/2013/08/20130808135715967.pdf. Accessed May 6, 2016.
de Rooij SR, Painter RC, Holleman F, Bossuyt PM, Roseboom TJ. The metabolic syndrome in adults prenatally exposed to the Dutch famine. Am J Clin Nutr. 2007;86(4):1219–24.
Stein AD, Zybert PA, van der Pal-de Bruin K, Lumey LH. Exposure to famine during gestation, size at birth, and blood pressure at age 59 y: evidence from the Dutch Famine. Eur J Epidemiol. 2006;21(10):759–65. doi:10.1007/s10654-006-9065-2. Epub 2006 Nov 3
Stanner SA, Bulmer K, Andrès C, Lantseva OE, Borodina V, Poteen VV, et al. Does malnutrition in utero determine diabetes and coronary heart disease in adulthood? Results from the Leningrad siege study, a cross sectional study. BMJ. 1997;315(7119):1342–8. doi:10.1136/bmj.315.7119.1342.
Roseboom TJ, van der Meulen JH, Ravelli AC, van Montfrans GA, Osmond C, Barker DJ, et al. Blood pressure in adults after prenatal exposure to famine. J Hypertens. 1999;17(3):325–30. doi:10.1097/00004872-199917030-00004.
Wang PX, Wang JJ, Lei YX, Xiao L, Luo ZC. Impact of fetal and infant exposure to the Chinese Great Famine on the risk of hypertension in adulthood. PLoS One. 2012;7(11):e49720. doi:10.1371/journal.pone.0049720. Epub 2012 Nov 21
Yu C, Wang J, Li Y, Han X, Hu H, Wang F, et al. Exposure to the Chinese famine in early life and hypertension prevalence risk in adults. J Hypertens. 2017;35(1):63–8.
Feng XL, Pang M, Beard J. Health system strengthening and hypertension awareness, treatment and control: data from the China Health and Retirement Longitudinal Study. Bull World Health Organ. 2014;92(1):29–41. doi:10.2471/BLT.13.124495. Epub 2013 Sep 10
Mu R, Zhang X. Why does the Great Chinese Famine affect the male and female survivors differently? Mortality selection versus son preference. Econ Hum Biol. 2011;9(1):92–105. doi:10.1016/j.ehb.2010.07.003. Epub 2010 Aug 3
Khanal P, Johnsen L, Axel AM, Hansen PW, Kongsted AH, Lyckegaard NB, et al. Long-Term Impacts of Foetal Malnutrition Followed by Early Postnatal Obesity on Fat Distribution Pattern and Metabolic Adaptability in Adult Sheep. PLoS One. 2016;11(6):e0156700. doi:10.1371/journal.pone.0156700. eCollection 2016
Neelsen S, Stratmann T. Effects of prenatal and early life malnutrition: evidence from the Greek famine. J Health Econ. 2011;30(3):479–88. doi:10.1016/j.jhealeco.2011.03.001. Epub 2011 Apr 2
Case A, Lubotsky D, Paxson C. Economic status and health in childhood: the origins of the gradient. AER. 2002;92(5):1308–34.
Almond D. Is the 1918 influenza pandemic over? Long-term effects of in utero influenza exposure in the post-1940 U.S. Population. J Polit Econ. 2006;114(4):672–711.
Stuebe AM, Schwarz EB, Grewen K, Rich-Edwards JW, Michels KB, Foster EM, et al. Duration of lactation and incidence of maternal hypertension: A longitudinal cohort study. Am J Epidemiol. 2011;174:1147–58.
Xu Y, Wang L, He J, Bi Y, Li M, Wang T, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310(9):948–59. doi:10.1001/jama.2013.168118.
Wang WX, Qu ZJ, Zhu AD. Epidemiologic analysis of diabetes among 10932 common residents in Chongqing Communities. Chongqing Med. 2013;42:26. (In Chinese)
Acknowledgments
Thanks Yong-Hong Wang, Hong Wang, Ji-Bin Li, Yong Zhang, Yi Zhang, Yong-Fang Liu, Da-Mei Liu, Jing-Lin Yang, Ling-Li Han, Xiao-Qin Zong, Ting-Yu Li in Chongqing Medical University for their actively participation.
Funding
This study was supported by Humanity and Social Science Foundation for the Youth Scholars of China's Ministry of Education (No.08JC840021).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
XLX was responsible for analysis, literature searches, the interpretation of the results, and writing the manuscript. LLL contributed to the interpretation of the results, and writing the manuscript. HZ, YZ, FZ, XQC, ZMS, YJ X, CR, and YZ contributed to the drafting of the manuscript. YZ was responsible for the conception of the study and overall supervision of the data collection and analysis, the interpretation of the results, and manuscript preparation. All authors have read and approved of the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional information
A correction to this article is available online at https://doi.org/10.1186/s12199-018-0698-z.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Liu, L., Xu, X., Zeng, H. et al. Increase in the prevalence of hypertension among adults exposed to the Great Chinese Famine during early life. Environ Health Prev Med 22, 64 (2017). https://doi.org/10.1186/s12199-017-0671-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12199-017-0671-2