
Abstract
The present study aimed to determine the correlation between controlling nutritional status (CONUT) and prognosis in resected breast cancer patients. Totally, 861 breast cancer patients with surgical resection in West China Hospital of Sichuan University between 2007 and 2010 were included. The relationship between CONUT and various clinicopathological factors as well as prognosis was evaluated. The results showed that the optimal cutoff value for CONUT to predict the 5-year survival was 3 and CONUT had a higher area under the ROC curve (AUC) for 5-year disease free survival (DFS) and overall survival (OS) prediction compared with the neutrophil lymphocyte ratio (NLR) and prognostic nutritional index (PNI). High CONUT was significantly correlated with older age, lymph node involvement, advanced T-stage, and surgery type. In the multivariate analysis, CONUT-high patients had worse DFS and OS, when compared with CONUT-low patients. In conclusion, preoperative CONUT is a useful marker for predicting long term outcomes in breast cancer patients after curative resection.
Similar content being viewed by others


Introduction
Breast cancer is one of the most commonly diagnosed malignancies in women worldwide1. Although surgery is the main treatment for breast cancer, its clinical course remains unsatisfactory since an appreciable part of patients develop local recurrence or distal metastasis after resection2. Hence, it is vital to find out potential biomarkers to accurately predict the prognosis and provide comprehensive information for selecting appropriate treatment strategies.
It has been identified that the cancer prognosis is, to some extent, related to host status, including nutrition or inflammation3. Besides, poor nutritional condition may be correlated with the metabolic elevation and the immune-compromised status in cancer patients4,5. Previous studies have reported that preoperative nutritional status, including albumin, is related with the prognosis in several malignancies4,6. Immune status is also correlated with tumor formation and recurrence7,8. Many indicators, including blood neutrophil, lymphocyte, monocyte, platelet count, neutrophilocyte-to-lymphocyte ratio (NLR), derived neutrophilcyte-to-lymphocyte ratio (dNLR), lymphocyte-to-monocyte ratio (LMR) and platelet-to-lymphocyte ratio (PLR), have been reported to be prognostic predictors in various cancers9,10,11,12,13. A meta-analysis showed that the LMR was significantly associated with long term outcomes in colorectal cancer14,15. What is more, it has also been verified that a platelet and lymphocyte-to-monocyte ratio (COP-LMR) is a novel prognosis predictor in lung cancer16.
The prognostic nutritional index (PNI), which consists of serum albumin concentration and total lymphocyte count, is used to assess the perioperative immunonutritional status and surgical risk for patients5. It has been reported that the PNI could predict postoperative complications including the intra-abdominal abscess, postoperative cardiovascular disease and pulmonary disease, pleural effusion, ascites, urinary tract infection, intraperitoneal and subcutaneous bleeding, inflammation of the intestine, obstruction of the intestine, pancreatic fistula, lymphorrhea, and numbness of limbs in patients with colorectal cancer17. Furthermore, it is corroborated to be a prognostic factor in various tumors, including breast cancer17,18,19,20,21. Based on these findings, a more comprehensive scoring system, controlling nutritional status (CONUT), consisting of serum albumin, cholesterol levels and lymphocyte count in peripheral blood, is yet to be proposed to assess patient nutritional status. Similar to PNI, CONUT could easily be calculated from blood examination data. Recently, it has been shown that CONUT is an independent prognostic marker in malignant pleural mesothelioma22, resected lung squamous cell carcinoma23, gastric cancer4, and head and neck cancer24. However, its role in breast cancer has not been reported. To our knowledge, we firstly attempted to assess the prognostic significance of CONUT in breast cancer patients who received curative resection based on a large study.
Materials and Methods
Patients and follow-up
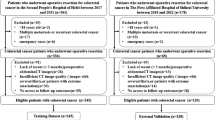
A total of 1,364 breast cancer patients who received surgical resection from 2007 to 2010 in West China Hospital of Sichuan University were recruited (Supplementary Dataset 1). The complete preoperative blood cell count was procured within seven days before surgery. The exclusion criteria were as follows: (1) patients who received chemotherapy or radiotherapy before the surgery; (2) patients with inflammatory disease or autoimmune disease; (3) patients who lacked detailed clinicopathological information; (4) male breast cancer patients. Finally, 861 cases were included in the present retrospective study. All the patients were followed up every three months in the first three years, every six months for five years, and annually within 6–10 years after the operation. Clinical check-up, laboratory examination and radiological assessment were included in the follow-up investigations.
Pathology methods and molecular subtypes
Estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2) statuses and Ki67 expression were assessed by immunohistochemical staining. The monoclonal ER antibody (clone SP1; Ventana, Tucson, AZ, USA), monoclonal PR (clone 1E2; Ventana), Ki-67 (clone 30–9; Ventana) and HER2 (clone 4B5; Roche, Sandhofer, Mannheim, Germany) were used. Positive ER or PR was defined as ≥1% of immunoreactive tumor cell nuclei, according to the American Society of Clinical Oncology and College of American Pathologists Guideline Recommendations in 2010. The cutoff value for Ki-67 was defined as ≥14%. As for HER-2, 0 or 1+ was negative, while 3+ was reported as positive. Fluorescence in situ hybridization (FISH) was performed in case of a 2+ level of staining.
The molecular subtypes were classified as Luminal A (ER+ and/or PR+, HER2−, Ki-67 < 14), Luminal B (ER+ and/or PR+, HER2+ and/or HER2-, any Ki-67), HER2-enriched (ER−, PR−, HER2+, any Ki-67), and triple-negative (ER−, PR−, HER2−, any Ki-67) breast cancer (TNBC).
Ethical approval and consent to participate
The study has been approved by the Institutional Ethical and Scientific Committee of West China Hospital of Sichuan University. Written informed consent was obtained from all participants in accordance with the policies of the committee. All methods applied within the study were performed according to the approved guidelines.
CONUT score and other scoring systems
The blood samples were investigated in one week before surgery. According to previous studies, the CONUT score was obtained based on serum albumin concentration, cholesterol level, and lymphocyte count (Table 1). The PNI was calculated by utilizing the following formula: 10 × the serum albumin value (g/dl) + 0.005 × the total lymphocyte count in peripheral blood (per mm3). The neutrophil-to-lymphocyte ratio was determined as the absolute neutrophil count divided by the absolute lymphocyte count.
Determination of the cutoff value
The receiver operating characteristic (ROC) curve was used to assess the sensitivity and specificity for 5-year survival. In addition, the Youden index was calculated to choose the best cutoff value.
Statistical analysis
OS was defined as the interval from diagnoses to death of any cause or last follow-up, whichever occurred first. DFS was calculated from the time of diagnoses to the first observation of recurrence or last follow-up without evidence of recurrence. The association between clinicopathological factors and CONUT was analyzed by X2-test. Variable was assessed on the univariate analysis, and then was calculated on the multivariable Cox proportion analysis if it was statistically significant. All statistical analyses were conducted by the SPSS (version 20.0) software pack (SPSS Inc., Chicago, IL, USA). P < 0.05 was statistically significant.
Results
ROC analysis
Using the 5-year survival as an endpoint, 3 was considered to be the best cutoff value for CONUT since the corresponding Youden index was maximal. The sensitivity and specificity for OS were 81.6% and of 35.7%, respectively (Fig. 1A,B). All the patients were classified into CONUT-low group (≤2) and CONUT-high group (≥3).

The ROC curves of CONUT, NLR and PNI for predicting DFS (A) and OS (B).
Comparison of CONUT with NLR or PNI
The prognostic accuracies of CONUT, PNI and NLR were explored by the AUC of the ROC curve for predicting the 5-year DFS and OS (Fig. 1A,B). The AUCs of CONUT, NLR and PNI for DFS were 0.622 (95% CI: 0.580–0.665), 0.590 (95% CI: 0.543–0.636), and 0.581 (95% CI: 0.539–0.624), respectively, while the AUCs of CONUT, NLR and PNI for OS were 0.621 (95% CI: 0.573–0.669), 0.579 (95% CI: 0.527–0.631), and 0.577 (95% CI: 0.530–0.625), respectively.
The correlation between CONUT and clinicopathological factors
Among the 861 breast cancer patients included in the present study, 223 patients were classified as luminal A subtype (25.9%), 407 patients were Luminal B subtype (47.3%), 135 patients were HER2 subtype (15.7%), and 96 patients were TNBC subtype (11.1%). The median age was 55 years old, with a median follow-up of 61.7 months. 206 patients developed tumor relapsed and154 patients died. The clinical and pathologic characteristics of the 861 patients in the present study were presented in Table 2. A high CONUT was significantly related with age, lymph node involvement, advanced T-stage and surgery type, but not related with Ki-67 status, high tumor grade, ER status, PR status, or HER2 over expression.
Correlations of the CONUT score with survival
The results revealed that a high CONUT was a poor prognostic factor for both DFS and OS in breast cancer patients. The 5-year OS rates were 68.7% in the COUNT-high group and 77.9% in the COUNT-low group (P = 0.013, Fig. 2A). In addition, the 5-year DFS rates were 76.6% in the COUNT-high group and 84.6% in the COUNT-low group (P = 0.006, Fig. 2B). After adjusting for p-stage, CONUT-high was still associated with worse DFS and OS in these three subgroups (Fig. 3A–F).

Kaplan-Meier survival analyses of the correlation between CONUT and survival among breast cancer patients: DFS (A) and OS (B).

Kaplan-Meier survival analyses of DFS and OS, according to CONUT, among patients in the stage I, stage II and stage III subgroups.
In the univariate analysis, high CONUT, patient age, PR status, tumor grade, T-stage, lymph node involvement and histological grade were related with DFS and OS. In the multivariate analysis, high CONUT (P = 0.07), patient age (P = 0.037), PR status (P = 0.041), tumor grade (P = 0.009), T-stage (P = 0.001) and lymph node involvement post-surgery (P = 0.002) were independent predictors of DFS, while high CONUT (P = 0.027), patient age (P = 0.042), tumor grade (P = 0.003), T-stage (P = 0.031) and lymph nodes (P = 0.002) were correlated with OS (Tables 3 and 4).
Since there are four molecular subtypes for breast cancer, the prognostic value of CONUT was subsequently analyzed in these four subgroups. The results revealed obvious associations of high CONUT score and worse outcomes in the luminal B subgroup (Tables 5 and 6).
Discussion
Studies have recently demonstrated the impact of CONUT on prognosis in several malignancies. In the present study, the prognostic value of CONUT in female breast cancer was initially assessed. Our results showed that CONUT was more accurate in prognosis prediction, when compared with previously reported prognostic scoring systems, PNI or NLR. Furthermore, the results indicated that CONUT was associated with age, tumor size and invasion. Importantly, CONUT independently predicted the prognosis of breast cancer patients, regardless of the tumor stage. Patients with high CONUT predicted the shorter DFS and OS, when compared with patients with low CONUT. Overall, these results suggested that CONUT might be a prognostic factor in breast cancer patients undergoing potentially curative resection. To our knowledge, our study firstly demonstrated the association between preoperative CONUT and clinicopathological factors or survival in breast cancer patients who underwent resection.
CONUT was originally reported as an efficient tool for the early detection and continuous control of hospital undernutrition25. Forward studies have demonstrated that CONUT has a prognostic impact on patients with severely decompensated acute heart failure26,27. Since CONUT was based on the serum albumin level, total cholesterol level and total lymphocyte count, the CONUT score could reflect the malnutrition and systemic inflammation status. Besides, tumor progression and treatment tolerance have been revealed to be closely correlated with the nutritional and inflammation status. Thus, CONUT could theoretically be a comprehensive prognostic factor. In the present study, the results show that CONUT is associated with both DFS and OS for all the included patients, and a high CONUT score might be associated with a poor prognosis.
PNI and NLR are both reported scoring systems for the evaluation of the general condition of patients and have been demonstrated to be related with cancer survival, including breast cancer2,28,29. Comparisons between CONUT and PNI, previous results suggested that CONUT tended to be more superior to the PNI scoring systems for the prediction of survival in various cancer patients. In the present study, our results suggested that CONUT was proved to be superior to both PNI and LNR for the prognosis prediction in resected breast cancer patients.
Among the three components of CONUT, serum albumin concentration is the most important parameter, which is twice the weight of the other two. It is a reliable indicator not only for nutritional status but also for systemic inflammation30,31. Studies demonstrated that low serum albumin was associated with poor survival and increased risk of cancer-related death in breast cancer patients32,33. Besides, pro-inflammatory cytokines (such as IL-6 or TNF-α) and CRP could also cause decreased serum albumin concentration and modulate albumin synthesis via hepatocytes34,35,36. As cholesterol plays a crucial role in forming cell membranes, cholesterol is related with numerous biochemical pathways which are potentially correlated immune response besides tumorigenesis37,38,39. It has also been reported that low cholesterol level is correlated with poor prognosis in various malignancies as the cholesterol may affect the caloric intake and cell membrane formation40,41. What is more, low peripheral lymphocyte count is an indicator for the inadequate host immune response and is correlated to undesirable prognosis in various cancers, including breast cancer9,42,43. Thus, the combination of these three parameters could integrate the accuracy of each parameter to assess for the general condition.
Conclusion
The present study indicates that CONUT is a useful prognostic factor for breast cancer patients undergoing curative resection, and a high CONUT score might be associated with a poor prognosis.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Torre, L. A. et al. Global cancer statistics, 2012. CA: a cancer journal for clinicians 65, 87–108, https://doi.org/10.3322/caac.21262 (2015).
Chen, J. et al. Meta-analysis of prognostic value of inflammation parameter in breast cancer. Journal of cancer research and therapeutics 14, S85–S89, https://doi.org/10.4103/0973-1482.160917 (2018).
Elinav, E. et al. Inflammation-induced cancer: crosstalk between tumours, immune cells and microorganisms. Nature reviews. Cancer 13, 759–771, https://doi.org/10.1038/nrc3611 (2013).
Kuroda, D. et al. Controlling Nutritional Status (CONUT) score is a prognostic marker for gastric cancer patients after curative resection. Gastric cancer: official journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association 21, 204–212, https://doi.org/10.1007/s10120-017-0744-3 (2018).
Migita, K. et al. The prognostic nutritional index predicts long-term outcomes of gastric cancer patients independent of tumor stage. Annals of surgical oncology 20, 2647–2654, https://doi.org/10.1245/s10434-013-2926-5 (2013).
Sakurai, K. et al. Predictive Potential of Preoperative Nutritional Status in Long-Term Outcome Projections for Patients with Gastric Cancer. Annals of surgical oncology 23, 525–533, https://doi.org/10.1245/s10434-015-4814-7 (2016).
Huang, Y. et al. Impacts of Preoperative Serum Albumin Level on Outcomes of Cytoreductive Surgery and Perioperative Intraperitoneal Chemotherapy. Annals of surgical oncology 23, 2411–2418, https://doi.org/10.1245/s10434-016-5172-9 (2016).
Prado, C. M. et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. The Lancet. Oncology 9, 629–635, https://doi.org/10.1016/s1470-2045(08)70153-0 (2008).
Karantanos, T., Karanika, S., Seth, B. & Gignac, G. The absolute lymphocyte count can predict the overall survival of patients with non-small cell lung cancer on nivolumab: a clinical study. Clinical & translational oncology: official publication of the Federation of Spanish Oncology Societies and of the National Cancer Institute of Mexico, https://doi.org/10.1007/s12094-018-1908-2 (2018).
Lee, J. S., Kim, N. Y., Na, S. H., Youn, Y. H. & Shin, C. S. Reference values of neutrophil-lymphocyte ratio, lymphocyte-monocyte ratio, platelet-lymphocyte ratio, and mean platelet volume in healthy adults in South Korea. Medicine 97, e11138, https://doi.org/10.1097/md.0000000000011138 (2018).
Mellor, K. L., Powell, A. & Lewis, W. G. Systematic Review and Meta-Analysis of the Prognostic Significance of Neutrophil-Lymphocyte Ratio (NLR) After R0 Gastrectomy for Cancer. Journal of gastrointestinal cancer, https://doi.org/10.1007/s12029-018-0127-y (2018).
Mizuguchi, S., Izumi, N., Tsukioka, T., Komatsu, H. & Nishiyama, N. Neutrophil-lymphocyte ratio predicts recurrence in patients with resected stage 1 non-small cell lung cancer. Journal of cardiothoracic surgery 13, 78, https://doi.org/10.1186/s13019-018-0763-0 (2018).
Zhang, L. X., Wei, Z. J. & Xu, A. M. Can the neutrophil-lymphocyte ratio and platelet-lymphocyte ratio be beneficial in predicting lymph node metastasis and promising prognostic markers of gastric cancer patients? Tumor maker retrospective study. International journal of surgery (London, England), https://doi.org/10.1016/j.ijsu.2018.06.037 (2018).
Tan, D., Fu, Y., Tong, W. & Li, F. Prognostic significance of lymphocyte to monocyte ratio in colorectal cancer: A meta-analysis. International journal of surgery (London, England) 55, 128–138, https://doi.org/10.1016/j.ijsu.2018.05.030 (2018).
Rosin, R. D. International Journal of Surgery. Editor’s perspectives–June 2015. International journal of surgery (London, England) 18, 245–246, https://doi.org/10.1016/j.ijsu.2015.05.031 (2015).
Lim, J. U. et al. Prognostic value of platelet count and lymphocyte to monocyte ratio combination in stage IV non-small cell lung cancer with malignant pleural effusion. PloS one 13, e0200341, https://doi.org/10.1371/journal.pone.0200341 (2018).
Tokunaga, R. et al. Prognostic Nutritional Index Predicts Severe Complications, Recurrence, and Poor Prognosis in Patients With Colorectal Cancer Undergoing Primary Tumor Resection. Diseases of the colon and rectum 58, 1048–1057, https://doi.org/10.1097/dcr.0000000000000458 (2015).
Mori, S. et al. The Significance of the Prognostic Nutritional Index in Patients with Completely Resected Non-Small Cell Lung Cancer. PloS one 10, e0136897, https://doi.org/10.1371/journal.pone.0136897 (2015).
Qiu, C. et al. Evaluation of Prognostic Nutritional Index in Patients Undergoing Radical Surgery with Nonsmall Cell Lung Cancer. Nutrition and cancer 67, 741–747, https://doi.org/10.1080/01635581.2015.1032430 (2015).
Sun, K., Chen, S., Xu, J., Li, G. & He, Y. The prognostic significance of the prognostic nutritional index in cancer: a systematic review and meta-analysis. Journal of cancer research and clinical oncology 140, 1537–1549, https://doi.org/10.1007/s00432-014-1714-3 (2014).
Yao, Z. H. et al. Prognostic nutritional index predicts outcomes of malignant pleural mesothelioma. Journal of cancer research and clinical oncology 139, 2117–2123, https://doi.org/10.1007/s00432-013-1523-0 (2013).
Takamori, S. et al. The Controlling Nutritional Status Score Is a Significant Independent Predictor of Poor Prognosis in Patients With Malignant Pleural Mesothelioma. Clinical lung cancer 18, e303–e313, https://doi.org/10.1016/j.cllc.2017.01.008 (2017).
Toyokawa, G. et al. Prognostic impact of controlling nutritional status score in resected lung squamous cell carcinoma. Journal of thoracic disease 9, 2942–2951, https://doi.org/10.21037/jtd.2017.07.108 (2017).
Kono, T., Sakamoto, K., Shinden, S. & Ogawa, K. Pre-therapeutic nutritional assessment for predicting severe adverse events in patients with head and neck cancer treated by radiotherapy. Clinical nutrition (Edinburgh, Scotland) 36, 1681–1685, https://doi.org/10.1016/j.clnu.2016.10.021 (2017).
Ignacio de Ulibarri, J. et al. CONUT: a tool for controlling nutritional status. First validation in a hospital population. Nutricion hospitalaria 20, 38–45 (2005).
Shirakabe, A. et al. The prognostic impact of malnutrition in patients with severely decompensated acute heart failure, as assessed using the Prognostic Nutritional Index (PNI) and Controlling Nutritional Status (CONUT) score. Heart and vessels 33, 134–144, https://doi.org/10.1007/s00380-017-1034-z (2018).
Lopez-Larramona, G., Lucendo, A. J. & Tenias, J. M. Association between nutritional screening via the Controlling Nutritional Status index and bone mineral density in chronic liver disease of various etiologies. Hepatology research: the official journal of the Japan Society of Hepatology 45, 618–628, https://doi.org/10.1111/hepr.12395 (2015).
Qiu, X., Song, Y., Cui, Y. & Liu, Y. Increased neutrophil-lymphocyte ratio independently predicts poor survival in non-metastatic triple-negative breast cancer patients. IUBMB life 70, 529–535, https://doi.org/10.1002/iub.1745 (2018).
Zhu, M. et al. Pretreatment neutrophil-lymphocyte and platelet-lymphocyte ratio predict clinical outcome and prognosis for cervical Cancer. Clinica chimica acta; international journal of clinical chemistry 483, 296–302, https://doi.org/10.1016/j.cca.2018.05.025 (2018).
Cengiz, O., Kocer, B., Surmeli, S., Santicky, M. J. & Soran, A. Are pretreatment serum albumin and cholesterol levels prognostic tools in patients with colorectal carcinoma? Medical science monitor: international medical journal of experimental and clinical research. 12, CR240–247 (2006).
de Ulibarri Perez, J. I., Fernandez, G., Rodriguez Salvanes, F. & Diaz Lopez, A. M. Nutritional screening; control of clinical undernutrition with analytical parameters. Nutricion hospitalaria 29, 797–811, https://doi.org/10.3305/nh.2014.29.4.7275 (2014).
Lis, C. G., Grutsch, J. F., Vashi, P. G. & Lammersfeld, C. A. Is serum albumin an independent predictor of survival in patients with breast cancer? JPEN. Journal of parenteral and enteral nutrition 27, 10–15, https://doi.org/10.1177/014860710302700110 (2003).
Cui, L. et al. Pituitary tumor transforming gene: a novel therapeutic target for glioma treatment. Acta Biochim Biophys Sin (Shanghai) 47, 414–421, https://doi.org/10.1093/abbs/gmv026 (2015).
Mohri, Y. et al. Prognostic nutritional index predicts postoperative outcome in colorectal cancer. World journal of surgery 37, 2688–2692, https://doi.org/10.1007/s00268-013-2156-9 (2013).
Peters, S. J. et al. Co-culture of primary rat hepatocytes with rat liver epithelial cells enhances interleukin-6-induced acute-phase protein response. Cell and tissue research 340, 451–457, https://doi.org/10.1007/s00441-010-0955-y (2010).
Honda, H. et al. Serum albumin, C-reactive protein, interleukin 6, and fetuin a as predictors of malnutrition, cardiovascular disease, and mortality in patients with ESRD. American journal of kidney diseases: the official journal of the National Kidney Foundation 47, 139–148, https://doi.org/10.1053/j.ajkd.2005.09.014 (2006).
Strasak, A. M. et al. Time-dependent association of total serum cholesterol and cancer incidence in a cohort of 172,210 men and women: a prospective 19-year follow-up study. Annals of oncology: official journal of the European Society for Medical Oncology 20, 1113–1120, https://doi.org/10.1093/annonc/mdn736 (2009).
Ko, K. et al. Influence of nutritional deficiency on prognosis of renal cell carcinoma (RCC). BJU international 112, 775–780, https://doi.org/10.1111/bju.12275 (2013).
Iribarren, C., Reed, D. M., Chen, R., Yano, K. & Dwyer, J. H. Low serum cholesterol and mortality. Which is the cause and which is the effect? Circulation 92, 2396–2403 (1995).
Kang, R. et al. Apolipoprotein E epsilon 2 allele and low serum cholesterol as risk factors for gastric cancer in a Chinese Han population. Scientific reports 6, 19930, https://doi.org/10.1038/srep19930 (2016).
Niendorf, A., Nagele, H., Gerding, D., Meyer-Pannwitt, U. & Gebhardt, A. Increased LDL receptor mRNA expression in colon cancer is correlated with a rise in plasma cholesterol levels after curative surgery. International journal of cancer 61, 461–464 (1995).
Vicente Conesa, M. A. et al. Predictive value of peripheral blood lymphocyte count in breast cancer patients treated with primary chemotherapy. Breast (Edinburgh, Scotland) 21, 468–474, https://doi.org/10.1016/j.breast.2011.11.002 (2012).
Hoskin, P. J., Rojas, A. M., Peiris, S. N., Mullassery, V. & Chong, I. Y. Pre-treatment haemoglobin and peripheral blood lymphocyte count as independent predictors of outcome in carcinoma of cervix. Clinical oncology (Royal College of Radiologists (Great Britain)) 26, 179–184, https://doi.org/10.1016/j.clon.2013.11.023 (2014).
Acknowledgements
We thank all practitioners who participated in the documentation of the data. This study was supported by the Grants from Science and Technology Bureau of Sichuan province (No. 2017RZ0045).
Author information
Authors and Affiliations
Contributions
Q.H.Z. conceived the study. W.L., M.L., T.W., Y.F.D., G.Z.M. and Z.K.L., were responsible for data curation and approval of the manuscript. G.Z.M., Q.W., X.J.L. and D.P. performed the analyses and prepared figure and tables. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, W., Li, M., Wang, T. et al. Controlling Nutritional Status (CONUT) score is a prognostic factor in patients with resected breast cancer. Sci Rep 10, 6633 (2020). https://doi.org/10.1038/s41598-020-63610-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-63610-7
- Springer Nature Limited