
Abstract
Three main surveillance systems (laboratory-confirmed, influenza-like illness (ILI) and nationwide Notifiable Infectious Diseases Reporting Information System (NIDRIS)) have been used for influenza surveillance in China. However, it is unclear which surveillance system is more reliable in developing influenza early warning system based on surveillance data. This study aims to evaluate the similarity and difference of the three surveillance systems and provide practical knowledge for improving the effectiveness of influenza surveillance. Weekly influenza data for the three systems were obtained from March 2010 to February 2015. Spearman correlation and time series seasonal decomposition were used to assess the relationship between the three surveillance systems and to explore seasonal patterns and characteristics of influenza epidemics in Gansu, China. Our results showed influenza epidemics appeared a single-peak around January in all three surveillance systems. Time series seasonal decomposition analysis demonstrated a similar seasonal pattern in the three systems, while long-term trends were observed to be different. Our research suggested that a combination of the NIDRIS together with ILI and laboratory-confirmed surveillance is an informative, comprehensive way to monitor influenza transmission in Gansu, China. These results will provide a useful information for developing influenza early warning systems based on influenza surveillance data.
Similar content being viewed by others


Introduction
Influenza is associated with considerable mortality and morbidity worldwide. Influenza surveillance systems are important tools for monitoring and evaluating transmission of influenza1,2,3,4,5. Gansu is relatively poor province, which public health capacity is backward compared with the economically developed provinces. The influenza incidence rates in Gansu were similar to the national average level. Influenza epidemics in Gansu exhibit strong seasonal winter peaks. In 2009, an extended influenza surveillance system for influenza-like illness (ILI) and virologic data was established in Gansu Province5. The extended influenza system aimed to better understand the epidemiologic trend of influenza epidemic and virus variation, and eventually develop an influenza early warning system that could provide advantage for improving the timeliness of epidemic control and formulating scientific prevention strategy. Currently there are three main systems used for influenza surveillance in Gansu Province, China: laboratory-confirmed (i.e., detection of influenza virus nucleic acid), ILI and nationwide Notifiable Infectious Diseases Reporting Information System (NIDRIS). This study aims to evaluate and compare effectiveness of the three influenza surveillance systems and provide practical knowledge for improving the performance of influenza surveillance in Gansu, China.
Results
Patterns of seasonality
There was a distinct seasonality in influenza occurrence in Gansu Province (Tables 1–3, Fig. 1). Both four series of monitoring data were highest in winter, followed by spring.

Influenza activity in different seasons in Gansu, 2010–2015. (a) Influenza-like illness (ILI) from Chinese Influenza Surveillance Information System. (b) ILI consultation rate (ILI%) from Chinese Influenza Surveillance Information System. (c) Influenza virus positive rate from Chinese Influenza Surveillance Information System. (d) Weekly influenza reported cases from nationwide Notifiable Infectious Diseases Reporting Information System (NIDRIS).
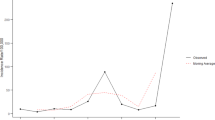
Our results showed an influenza epidemic to appear as a typical single-peak, around January, in all three surveillance systems. Time series seasonal decomposition analysis demonstrated a similar seasonal pattern in the three systems (Fig. 2). However, long-term trends were observed to differ between the three systems.

Seasonal decomposition of influenza in Gansu, 2010–2015. (a) Influenza-like illness (ILI) from Chinese Influenza Surveillance Information System. (b) ILI consultation rate (ILI%) from Chinese Influenza Surveillance Information System. (c) Influenza virus positive rate from Chinese Influenza Surveillance Information System. (d) Weekly influenza reported cases from nationwide Notifiable Infectious Diseases Reporting Information System (NIDRIS).
Correlation analysis
Fitted lines with scatter plots were shown for positive correlation between any two sets of data (Fig. 3). Spearman correlation indicated that influenza cases of NIDRIS correlated significantly with ILI (r = 0.741, p < 0.01), ILI% (r = 0.442, p < 0.01), and positive rate (r = 0.486, p < 0.01) (Table 4).

Correlation between different surveillance data in Gansu, 2010–2015. ILI: Influenza-like illness from Chinese Influenza Surveillance Information System. ILI%: ILI consultation rate from Chinese Influenza Surveillance Information System. Positive rate: Influenza virus positive rate from Chinese Influenza Surveillance Information System. Influenza cases: Weekly influenza reported cases from nationwide Notifiable Infectious Diseases Reporting Information System (NIDRIS).
Comparison of advantages and disadvantages
Table 5 summarized the advantages and disadvantages for the three surveillance systems (Table 5).
Discussion
There is a high correlation among the three influenza surveillance systems data, suggesting that all three influenza surveillance systems in Gansu Province reflect the epidemic characteristics of influenza. The three influenza surveillance systems indicated that there were epidemics peaks in winter and similar seasonal pattern. The influenza epidemics typically appeared as a single-peak around January in Gansu; this finding is consistent with other northern provinces in China1,6. Seasonal decomposition, however, showed differences in long-term trends of the three systems. The increase in ILI cases may be due to surveillance sensitivity improvement, while the downward trend of Influenza-like illness consultation rate (ILI%) may be due to the increase in total visits to outpatient and/or emergency departments. At the same time, the increase in monitoring sensitivity, and the increase in laboratory-confirmed influenza cases resulted in an increase in reported cases of influenza from NIDRIS. Influenza virus positive rate, the percentage of swabs that are positive for influenza by real-time Polymerase Chain Reaction (PCR), can provide accurate information about influenza virus activity, while its monitoring results indicated that influenza epidemic peak didn’t occur in the very same time (Fig. 2c), so it’s very necessary to carry out continuous monitoring of influenza and set up a suitable early warning technology7,8,9,10.
Each of the three surveillance systems has its own advantages and disadvantages. Laboratory surveillance can provide more accurate information about the activity of influenza virus serotypes, so influenza virus positive rate could be used as an indicator for influenza epidemic; it is, however, time consuming and resource intensive and thus may delay the early warning and control of influenza epidemics11. By contrast, ILI and ILI% are better indicators for use in early warning systems as they tend to be more time efficient in the generation of data. Sentinel systems, however, rely upon individual doctors or clinics to collate data and report it to the relevant authority, this may introduce compliance or bias issues. Furthermore, illnesses other than influenza may present with ILI12; sentinel hospitals report ILI by age group, without case information; increases in ILI and ILI% may be the result of increased healthcare-seeking behavior in response to media reports or the circulation of non-influenza respiratory viruses13,14. ILI, ILI% and positive rate are based on the sentinel surveillance network which is built on data sourced from urban areas; as such, this system may not detect influenza virus activity in rural areas2,4,11,15,16. By contrast, influenza cases of NIDRIS are reported by all medical institutions in Gansu Province, including secondary, tertiary, pediatric hospitals in urban areas, and primary hospitals and village clinics in rural areas. Weekly influenza data from the NIDRIS were observed to have larger fluctuations and during the long vacation (especially Chinese New Year), influenza cases greatly reduced (Fig. 2d) and data stability were affected because of an obvious decrease of patients’ visits. Some influenza patients may be misdiagnosed, because it’s hard to differentiate influenza from other respiratory viruses without laboratory testing, especially in the non-epidemic season; in addition, as passive surveillance, influenza cases may also be misreported to NIDRIS. This demonstrated the need to improve mechanisms for sharing information between influenza surveillance systems4,17, to enhance capacities.
This study was the first attempt to compare performance of all the three influenza surveillance systems in Gansu Province. The results of this study provide practical knowledge for developing early warning systems for influenza based on surveillance system with climate and socio-environmental data18.
As the influenza surveillance systems were extended in 2009, only five-year data time series were available. This limited analysis of long-term epidemiological characteristics19,20.
Conclusion
A combination of the NIDRIS together with ILI and laboratory-confirmed surveillance is an informative, comprehensive way to monitor influenza transmission in Gansu, China. We should consider combining the three surveillance systems in developing influenza early warning systems.
Methods
Located in the northwest of China, Gansu Province covers an area of 453,700 square kilometers, with a population of 25.91 million (2014). The climate is cold and dry in Gansu Province and exhibits large fluctuations in temperature between day and night. The annual average temperature ranges from 0 degrees Celsius in the northwest to 14 degrees Celsius in the southeast; mean annual rainfall is about 300 millimeters, however this differs greatly across regions.
Weekly ILI data were obtained from the national sentinel hospital-based influenza surveillance network. This network consists of 19 sentinel hospitals in Gansu, dispersed through 18 counties and districts, including all 14 cities of Gansu. These 19 sentinel hospitals are the larger comprehensive hospitals, located in the densely populated districts of these cities, and are recognized by the National Ministry of Health to represent the medical-seeking people in Gansu. Each week, participating doctors in the outpatient and emergency departments of internal medicine and pediatrics were required to report the number of patients with ILI by age group (i.e., 0–4 years, 5–14 years, 15–24 years, 25–59 years, and >60 years), and total visits to outpatient and/or emergency departments to the Chinese Influenza Surveillance Information System, which is a centralized online system. Identification of patients with ILI was based on a standard case definition, including body temperature ≥38 °C with either cough or sore throat, in the absence of other laboratory-confirmed evidence21. In this study, surveillance data for the period of March 2010 (2010 week 10) to February 2015 (2015 Week 9) was used. ILI consultation rate (ILI%) = ILI/total visits to outpatient and emergency departments * 100%.
Laboratory-confirmed influenza cases were collected for same period from the Chinese Influenza Surveillance Information System. In each sentinel hospital, nasopharyngeal swabs were collected from patients who presented within 3 days of ILI onset. The specimens were transported in viral transport media at 4 °C to the diagnostic laboratories within 48 h of collection. Analysis for influenza virus nucleic acid was performed by real-time Polymerase Chain Reaction (PCR) within 1 week. Taking swabs is a mandatory practice for all sentinel hospitals. Each hospital was required to provide 5 to 15 specimens per month from April to September and 10 to 15 specimens per week from October to next March21. Participating doctors chose the patients with typical ILI symptom to collect their swabs, and ensure that the specimen was evenly distributed every week or month.
Influenza is a notifiable infectious disease in China22. Case definitions for influenza and diagnostic criteria are outlined by the National Health and Family Planning Commission of the People’s Republic of China, which includes clinically diagnosed cases and laboratory-confirmed cases. Notifications of cases are made to NIDRIS, by all medical institutions in Gansu Province, including secondary, tertiary and pediatric hospitals in urban areas, primary hospitals and village clinics in rural areas. Weekly data for reported cases of influenza were obtained from NIDRIS for the period of March 2010 (2010 week 10) to February 2015 (2015 Week 9).
The three systems were used to validate the influenza surveillance quality each other, especially in epidemic period.
Four sets of monitoring data were obtained from the three influenza surveillance systems: ILI, ILI%, positive rate of nucleic acid detection and influenza cases of NIDRIS. The sets of ILI and ILI% were taken from influenza-like illness surveillance of Chinese Influenza Surveillance Information Systems, the set of positive rate came from the laboratory testing results of Chinese Influenza Surveillance Information Systems, while the set of influenza cases was obtained from reported influenza numbers of NIDRIS, including all the clinically diagnosed cases and laboratory-confirmed cases. All four series data were collected continuously from March 2010 (2010 week 10) to February 2015 (2015 week 9). Each series of data was up to five years.
Spearman correlation was used to assess the relationship between the three surveillance systems, as the data appeared to have non-normally distributed pattern. A seasonal decomposition analysis was conducted to assess whether there was a distinct seasonality in each series. In this analysis, each time series was decomposed into seasonality, long-term trend, and irregular factors. The long-term trend showed progression of the influenza series (secular variation). A trend exists when there was a persistent increasing or decreasing direction in the surveillance data23.
We confirm that all methods were performed in accordance with the relevant guidelines and regulations by including a statement in the methods section.
Ethics approval and consent to participate
The study was approved by the Research Ethics Committee of Gansu Provincial Center for Disease Control and Prevention. Informed consent is not relevant to the study as this study used aggregated data without personal information.
Availability of data and material
Please contact author for data requests.
References
Zou, J. et al. Geographic Divisions and Modeling of Virological Data on Seasonal Influenza in the Chinese Mainland during the 2006–2009 Monitoring Years. Plos One 8, e58434–e58434, https://doi.org/10.1371/journal.pone.0058434 (2013).
Yu, H. et al. Regional variation in mortality impact of the 2009 A(H1N1) influenza pandemic in China. Influenza & Other Respiratory Viruses 7, 1350–1360, https://doi.org/10.1111/irv.12121 (2013).
Yu, H. et al. The substantial hospitalization burden of influenza in central China: surveillance for severe, acute respiratory infection, and influenza viruses, 2010–2012. Influenza & Other Respiratory Viruses, https://doi.org/10.1111/irv.12205 (2013).
Jing, Z., Shi, G. Q. & Shu, Y. L. Strategies on Enhancing Capacities of Influenza Surveillance in China. Chinese Journal of Vaccines & Immunization (2005).
Ren, Y. H. et al. Research on influenza surveillance systems in China and abroad. Disease Surveillance, https://doi.org/10.3784/j.issn.1003-9961.2010.10.020 (2010).
Yu, H. et al. Characterization of regional influenza seasonality patterns in China and implications for vaccination strategies: spatio-temporal modeling of surveillance data. Plos Medicine 10, e1001552–e1001552, https://doi.org/10.1371/journal.pmed.1001552 (2013).
Meng, L. et al. Dynamic prediction on the number of influenza-like cases in Gansu province based on data from the influenza sentinel surveillance program, from 2006 to 2011. Chinese Journal of Epidemiology 33, 1155–1158, https://doi.org/10.3760/cma.j.issn.0254-6450.2012.11.013 (2012).
Peng, Y. et al. Review of an influenza surveillance system, Beijing, People’s Republic of China. Emerging Infectious Diseases 15, 1603–1608, https://doi.org/10.3201/eid1510.081040 (2009).
Yang, X. T. et al. Study on early warning method for influenza epidemic in Gansu province. Chinese Journal of Epidemiology 37, https://doi.org/10.3760/cma.j.issn.0254-6450.2016.03.029 (2016).
Cao, P. et al. Spatial-temporal variations of influenza activity in two subtropical cities. British Journal of Nutrition 87, 253–260 (2012).
Jia-Bing, W. U. et al. Analysis of influenza surveillance quality in sentinel hospitals of Anhui,2010. Anhui Journal of Preventive Medicine (2012).
Yang, L. et al. Synchrony of Clinical and Laboratory Surveillance for Influenza in Hong Kong. Plos One 3, e1399, https://doi.org/10.1371/journal.pone.0001399 (2008).
Zhang, Y., Arab, A., Cowling, B. J. & Stoto, M. A. Characterizing Influenza surveillance systems performance: application of a Bayesian hierarchical statistical model to Hong Kong surveillance data. Bmc Public Health 14, 850–850 (2014).
Xu, C. et al. Monitoring avian influenza A(H7N9) virus through national influenza-like illness surveillance, China. Emerging Infectious Diseases 19, 1289–1292, https://doi.org/10.3201/eid1908.130662 (2013).
Huang, Z. Y., Zhang, Q. L., Zhong, X. G., Zhang, M. & Rao, F. Evaluation of influenza surveillance system in Dongguan,Guangdong province. Disease Surveillance, https://doi.org/10.3784/j.issn.1003-9961.2012.1.022 (2012).
Zhang, Y. et al. Influenza Surveillance and Incidence in a Rural Area in China during the 2009/2010 Influenza Pandemic. Plos One 9, e115347–e115347, https://doi.org/10.1371/journal.pone.0115347 (2014).
Tan, Y. et al. Increasing similarity in the dynamics of influenza in two adjacent subtropical Chinese cities following the relaxation of border restrictions. Journal of General Virology 95, 531–538, https://doi.org/10.1099/vir.0.059998-0 (2014).
Yang, W. et al. A nationwide web-based automated system for outbreak early detection and rapid response in China. Western Pac Surveill Response J 2, 10–15, https://doi.org/10.5365/WPSAR.2010.1.1.009 (2011).
Cheng, X. et al. Epidemiological dynamics and phylogeography of influenza virus in southern China. Journal of Infectious Diseases 207, 106–114, https://doi.org/10.1093/infdis/jis526 (2013).
Yan, L. et al. Geographical Epidemiology Comparative Study on Influenza Surveillance Systems at Home and Abroad. Journal of Geo-Information Science 12, 410–418 (2010).
National Health and Family Planning Commission of the People’s Republic of China (2010) Influenza sentinel surveillance protocol, http://www.nhfpc.gov.cn/jkj/s3577/201009/3fa356d0f4834d408fde6c12891a6482.shtml (2010).
Standing Committee of the National People’s Congress (2004) Law of the People's Republic of China on the Prevention and Treatment of Infectious Diseases.
E. S. G. Jr. Forecasting: Methods and applications (Second Edition), Makridakis, S., Wheelwright, S. C. and McGee, V. E., New York: Wiley, 1983. Journal of Forecasting 3, 457–460 (1984).
Acknowledgements
We gratefully acknowledge the support of the “Chinese Influenza Surveillance Information System”. We also thank all the sentinel hospitals and network laboratories in Gansu Province. This work was supported by grants from the Research Management for Health of Gansu Province (Grant No. GWGL2014-83) and the major project of “Infectious Diseases Prevention and Control” of Science and Technology Monitoring Platform (Grant No. 2012ZX10004-208). W.H was supported by an Australian Research Council Future Fellowship (FT140101216).
Author information
Authors and Affiliations
Contributions
X.Y. and D.L. contributed equally to this study. W.H. and J.H. conceptualized the idea and revised the study protocol, especially the research design. X.Y. and D.L. analyzed the data and drafted the manuscript. K.W. and X.L. helped drafting the manuscript and drew the figures for the article. W.H., L.M., D.Y., H.L. and B.L. provided interpretation of the results. All of the authors contributed to the writing. All of the authors have read and approved the article.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, X., Liu, D., Wei, K. et al. Comparing the similarity and difference of three influenza surveillance systems in China. Sci Rep 8, 2840 (2018). https://doi.org/10.1038/s41598-018-21059-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-21059-9
- Springer Nature Limited
This article is cited by
-
Forecasting and analyzing influenza activity in Hebei Province, China, using a CNN-LSTM hybrid model
BMC Public Health (2024)
-
Epidemiological features of seasonal influenza transmission among 11 climate zones in Chinese Mainland
Infectious Diseases of Poverty (2024)
-
Influenza A and B outbreaks differed in their associations with climate conditions in Shenzhen, China
International Journal of Biometeorology (2022)
-
Spatiotemporal Analysis of Influenza in China, 2005–2018
Scientific Reports (2019)