
Abstract
The aim of this study was to systematically review and meta-analyze published data on the diagnostic accuracy of positron emission tomography (PET) using fluorine-18-dihydroxyphenylalanine ([18F]DOPA) in patients with neuroendocrine tumors (NETs). A comprehensive computer literature search of the PubMed/MEDLINE, Embase and Scopus databases was conducted to identify studies on the use of [18F]DOPA PET or PET/computed tomography (PET/CT) in patients with proven or suspected NETs. Pooled sensitivity and specificity of [18F]DOPA PET and PET/CT on a per patient-based analysis were calculated. The area under the ROC curve was calculated to measure the accuracy of [18F]DOPA PET or PET/CT. Eight articles on gastroenteropancreatic and thoracic NETs, 13 on pheochromocytoma/paraganglioma (Pheo/PGL) and eight on recurrent medullary thyroid carcinoma (MTC) were included in our meta-analysis. The pooled sensitivity and specificity of [18F]DOPA PET or PET/CT in patients with thoracic and gastroenteropancreatic NETs were 77% (95% CI 71–82) and 95% (95% CI 87–98), respectively. The area under the ROC curve was 0.94. The pooled sensitivity and specificity of [18F]DOPA PET or PET/CT in patients with Pheo/PGL were 92% (95% CI 88–95) and 92% (95% CI 85–97), respectively. The area under the ROC curve was 0.95. The pooled sensitivity of [18F]DOPA PET or PET/CT in patients with recurrent MTC was 62% (95% CI 54–69). Heterogeneity was found between the studies with regard to the sensitivity of [18F]DOPA PET or PET/CT. Evidence-based data show that [18F]DOPA PET and PET/CT are accurate methods in patients with proven or suspected NETs. Large multicenter studies are necessary to substantiate the diagnostic accuracy of [18F]DOPA PET and PET/CT in this setting.
Similar content being viewed by others

Introduction
Neuroendocrine tumors (NETs) are rare neoplasms that arise from neuroendocrine cells which are present not only in the endocrine glands but also diffusely in all body tissues. Neuroendocrine cells share common features, such as having special secretory granules and often producing biogenic amines and polypeptide hormones. Both normal and tumoral neuroendocrine cells may uptake and decarboxylate amine precursors (such as l-DOPA and 5-hydroxytryptophan) to produce biogenic amines, such as catecholamines and serotonin [1–3].
Although NETs share some pathological and clinical features, significant differences do exist between different tumor types and locations [1–3]. Correct classification of NETs according to the various locations, on the basis of the recently published WHO classification, is important for appropriate treatment in each group [2, 3]. As regards their origin and location, NETs may arise from different regions, such as the gastrointestinal tract, the pancreatic islet cells, the lung and the thymus.
Furthermore, medullary thyroid carcinoma (MTC), arising from parafollicular cells of the thyroid, pheochromocytoma and paraganglioma (Pheo/PGL), arising from chromaffin cells of the adrenal glands (Pheo) and sympathetic or parasympathetic paraganglia (PGL), are also considered NETs [1].
Functional imaging methods are useful for providing accurate staging and extent of the disease in patients with NETs. Information obtained by combining conventional and functional imaging methods may influence the management of these patients [4, 5].
Recently, the use of positron emission tomography (PET) imaging in NETs has been growing rapidly and different positron-emitting radiopharmaceuticals (with different uptake mechanisms) have been developed [4, 5]. In particular, fluorine-18-dihydroxyphenylalanine ([18F]DOPA) has been proposed as a useful PET tracer for the imaging of NETs, because these tumors have the ability to accumulate and decarboxylate biogenic amines such as l-DOPA [6]. After intracellular uptake through the large amino acid transporter, [18F]DOPA is decarboxylated by DOPA decarboxylase to [18F]DOPAmine, which is transported into storage granules by vesicular monoamine transporter and trapped intracellularly [6].
Several single-center studies have evaluated the diagnostic performance of [18F]DOPA PET or PET/CT in patients with proven or suspected NETs, reporting different values of sensitivity and specificity; the purpose of our article is to systematically review and meta-analyze published data on the diagnostic accuracy of [18F]DOPA PET or PET/CT in patients with NETs, in order to add more evidence-based data in this setting.
Methods
Search strategy
A comprehensive computer literature search of the PubMed/MEDLINE, Embase and Scopus databases was conducted to find published articles on the diagnostic performance of [18F]DOPA PET and PET/CT in patients with NETs, including patients with gastroenteropancreatic and thoracic NETs, Pheo/PGL, neuroblastoma, MTC, and ectopic adrenocorticotropin-secreting tumors. We used a search algorithm that was based on a combination of the terms: (a) “DOPA” or “dihydroxyphenylalanine” and (b) “PET” or “positron emission tomography”. No start date limit was used; the search was updated till 23 October 2012. No language restriction was used. To expand our search, references of the retrieved articles were also screened for additional studies.
Study selection
Studies (or subsets in studies) investigating the diagnostic accuracy of [18F]DOPA PET or PET/CT in patients with NETs were eligible for inclusion. The exclusion criteria were: (a) articles not within the field of interest of this review; (b) review articles, editorials or letters, comments, conference proceedings; (c) case reports or small case series; (d) overlap of patient data (in such cases the most complete article was included); (e) insufficient data to calculate sensitivity or specificity from individual studies on a per patient-based analysis.
Two researchers (VR and GT) independently reviewed the titles and abstracts of the retrieved articles, applying the inclusion and exclusion criteria mentioned above. Articles were rejected if they were clearly ineligible. The same two researchers then independently reviewed the full-text versions of the remaining articles to determine their eligibility for inclusion. Disagreements were resolved in a consensus meeting.
Data extraction
For each included study, information was collected concerning the basic study (authors, journal, year of publication, country of origin, study design), patient characteristics (population evaluated, number of patients performing PET, mean age, sex), other functional imaging performed and technical aspects (device used, [18F]DOPA injected dose, time between [18F]DOPA injection and image acquisition, carbidopa pretreatment, image analysis, applied reference standard). For each study, the numbers of true-positive, false-positive, true-negative and false-negative findings for [18F]DOPA PET or PET/CT on a per patient-based analysis were recorded.
Quality assessment
Two independent reviewers evaluated the methodology of the selected studies using QUADAS, a tool for the quality assessment of diagnostic accuracy studies [7].
Statistical analysis
Sensitivity and specificity of [18F]DOPA PET or PET/CT in patients with NETs were obtained on a per patient-based analysis from individual studies. A random effect model was used for statistical pooling of the data taking into account heterogeneity between the studies. Pooled data were presented with 95% confidence intervals (95% CI). An I 2 statistic was also performed to test for heterogeneity between studies. The area under the ROC curve was calculated to measure the accuracy of [18F]DOPA PET or PET/CT in patients with NETs. Statistical analyses were performed using Meta-DiSc statistical software version 1.4 (Unit of Clinical Biostatistics, Ramón y Cajal Hospital, Madrid, Spain) [8].
Results
Literature search
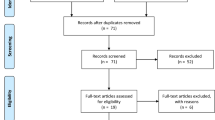
The comprehensive computer literature search of the PubMed/MEDLINE, Embase and Scopus databases revealed 1,218 articles. On reviewing the titles and abstracts, 1,166 articles were excluded as case reports, reviews, editorials or articles not within the field of interest of this review.
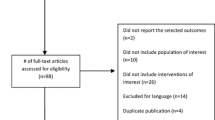
Fifty-two articles were selected and retrieved in full-text version; no additional study was found on screening the references of these articles. The full texts of these 52 articles potentially eligible for inclusion were then reviewed and four were excluded as case series, eight because of possible data overlap and nine due to insufficient data to calculate sensitivity or specificity of [18F]DOPA PET. The number of retrieved articles dealing with neuroblastoma [9, 10] and ectopic adrenocorticotropin-secreting tumors [11] was not sufficient to perform a meta-analysis.
Finally, eight articles on gastroenteropancreatic and thoracic NETs, 13 on Pheo/PGL and eight on recurrent MTC met all the inclusion and none of the exclusion criteria, and were included in our meta-analysis [12–39] (Fig. 1). The characteristics of the included studies are presented in Tables 1, 2, 3, 4, 5, and 6.

Flow chart of the search for eligible studies on the diagnostic accuracy of [18F]DOPA PET and PET/CT in patients with NETs
Quality assessment
Overall, the studies included in this systematic review showed moderate methodological quality, as assessed using QUADAS. The studies scored between 7/14 and 11/14 with a median score of 9/14. The index test and the reference standard were often interpreted without blinding, and this was the most critical issue with regard to the methodological quality of the included studies.
Diagnostic performance
The diagnostic performance results of [18F]DOPA PET or PET/CT in the included studies were divided into three groups.
The sensitivity and specificity of [18F]DOPA PET or PET/CT in patients with thoracic and gastroenteropancreatic NETs ranged from 56 to 95% and from 89 to 100%, with pooled estimates of 77% (95% CI 71–82) and 95% (95% CI 87–98), respectively (Fig. 2a, b). The included studies were statistically quite heterogeneous in their estimates of sensitivity (I 2 61%) and homogeneous in their estimates of specificity (I 2 0%). The area under the ROC curve was 0.94 (Fig. 2c).

Plot of individual studies and pooled sensitivity (a) and specificity (b) of [18F]DOPA PET and PET/CT in patients with thoracic and gastroenteropancreatic NETs on a per patient-based analysis. The size of the circles indicates the weight of each study. Pooled sensitivity and specificity were 77% (95% CI 71–82) and 95% (95% CI 87–98), respectively. Summary ROC curve of diagnostic accuracy of [18F]DOPA PET and PET/CT in patients with thoracic and gastroenteropancreatic NETs on a per patient-based analysis (c). The area under the ROC curve was 0.94
The sensitivity and specificity of [18F]DOPA PET or PET/CT in patients with Pheo/PGL ranged from 77 to 100% and from 75 to 100%, with pooled estimates of 92% (95% CI 88–95) and 92% (95% CI 85–97), respectively (Fig. 3a, b). The included studies were statistically quite heterogeneous in their estimates of sensitivity (I 2 52.7%) and homogeneous in their estimates of specificity (I 2 0%). The area under the ROC curve was 0.95 (Fig. 3c).

Plot of individual studies and pooled sensitivity (a) and specificity (b) of [18F]DOPA PET and PET/CT in patients with Pheo/PGL on a per patient-based analysis. The size of the circles indicates the weight of each study. Pooled sensitivity and specificity were 92% (95% CI 88–95%) and 92% (95% CI 85–97%), respectively. Summary ROC curve of diagnostic accuracy of [18F]DOPA PET and PET/CT in patients with Pheo/PGL on a per patient-based analysis (c). The area under the ROC curve was 0.95
The sensitivity of [18F]DOPA PET or PET/CT in patients with recurrent MTC ranged from 44 to 83% with pooled estimates of 62% (95% CI 54–69) (Fig. 4). The included studies were statistically quite heterogeneous in their estimates of sensitivity (I 2 49.2%). The pooled specificity of [18F]DOPA PET or PET/CT in patients with recurrent MTC could not be calculated from the included studies due to lack of data on false-positive and true-negative findings.

Plot of individual studies and pooled sensitivity of [18F]DOPA PET and PET/CT in patients with recurrent MTC on a per patient-based analysis. The size of the circles indicates the weight of each study. Pooled sensitivity was 62% (95% CI 54–69)
Discussion
Several single-center studies have used [18F]DOPA PET or PET/CT in patients with proven or suspected NETs, reporting different values of sensitivity and specificity [12–39]. However, many of these studies have limited power, analyzing only relatively small numbers of patients. In order to derive more robust estimates of the diagnostic accuracy of [18F]DOPA PET or PET/CT in this setting, we pooled published studies, adopting a systematic review process to identify studies.
Overall, the studies included in this meta-analysis showed moderate quality according to QUADAS [7]. However, this tool has some limitations given that it is not meant to be used as a scale. In fact, the items have different relevance in the assessment of quality: the quality of a study achieving a very high score, with almost all the items fulfilled, could still be debatable if it does not meet one of the most important items, such as the use of the same reference standard in all the patients. Another drawback of QUADAS is that it does not take into consideration sample size, which determines the precision of the study and its validity too. On the other hand, it is important to remember that the low quality could also be due to limitations in carrying out these kinds of studies in the real clinical setting, where it might be difficult to confirm the final diagnosis in all patients.
The pooled results of our meta-analysis indicate that [18F]DOPA PET and PET/CT are accurate diagnostic methods in patients with thoracic and gastroenteropancreatic NETs (the area under the ROC curve was 0.94), demonstrating a good pooled specificity (95%) and a moderate sensitivity (77%).
Nevertheless, possible sources of false-negative results of these functional imaging methods should be kept in mind; these could be related to several factors, such as small size of the neuroendocrine lesion, location of the tumor near organs with high physiological [18F]DOPA uptake (such as the pancreas, biliary and urinary systems), or loss of [18F]DOPA uptake due to tumor dedifferentiation.
The sensitivity of these methods could also be related to the location and type of NET. [18F]DOPA PET and PET/CT have a very high sensitivity in midgut NETs, much better than the pooled value of 77%, but a low sensitivity in foregut NETs (including bronchial, gastric, duodenal and pancreatic NETs) [40]. In some articles, patients with NETs were divided into two populations (carcinoid and non-carcinoid tumors). A higher sensitivity of [18F]DOPA PET and PET/CT in patients with carcinoid tumors compared to non-carcinoid tumors (i.e. pancreatic NETs) was reported [13, 17, 40].
The high specificity of [18F]DOPA PET and PET/CT in patients with NETs can be explained by the fact that only neuroendocrine cells are able to take up, decarboxylate, and store amino acids and their amines. With regard to this high specificity, an important advantage over other PET tracers (such as Gallium-68-somatostatin analogs and fluorine-18-fluorodeoxyglucose) is that [18F]DOPA is not taken up in a significant proportion by inflammatory cells.
The pooled results of our meta-analysis indicate that [18F]DOPA PET and PET/CT are accurate diagnostic methods in patients with Pheo/PGL (the area under the ROC curve was 0.95), demonstrating a good pooled specificity (92%) and sensitivity (92%). The possible sources of false-negative results are the ones previously mentioned. Furthermore, discordant results regarding the influence of genetic factors in the diagnostic accuracy of these methods are reported. Timmers et al. [25] reported that succinate dehydrogenase B (SDHB) gene mutations may result in extra-adrenal PGLs which, compared with non-SDHB-related lesions, show a lower sensitivity of [18F]DOPA PET. Recently, Rischke et al. [31] reported that [18F]DOPA PET is a sensitive and specific imaging modality for the detection and staging of Pheo/PGL in various genotypes, including SDHD-mutation carriers, and in patients with no germline mutation.
According to the literature data, [18F]DOPA PET and PET/CT seem to be accurate methods in both adrenal and extra-adrenal, sympathetic and parasympathetic, functioning and non-functioning, and metastatic and non-metastatic Pheo/PGL [16, 20–31]. In particular, [18F]DOPA PET and PET/CT seem to be the most sensitive imaging methods for detecting head and neck PGLs, usually parasympathetic-derived tumors, probably because of the high tracer avidity of these neoplasms and the favorable lesion-to-background ratio in the head and neck [21, 30].
Evidence-based data from our meta-analysis suggest that [18F]DOPA PET and PET/CT are associated with a moderate sensitivity in the evaluation of recurrent MTC (62%). On the other hand, this pooled sensitivity should be considered significant, because [18F]DOPA PET and PET/CT are often performed in patients with suspected recurrent MTC after negative findings on conventional imaging studies. In fact, in most cases, patients are referred for [18F]DOPA PET or PET/CT because of rising levels of calcitonin, a very sensitive and specific tumor marker for MTC, in a context of occult biochemical recurrence where all the other imaging modalities have failed. In this context, a sensitivity of over 50% means a successful modality.
Furthermore, [18F]DOPA PET and PET/CT may affect the management of a significant number of patients with recurrent MTC [32–39, 41].
Possible causes of false-negative results of [18F]DOPA PET and PET/CT could be related to small MTC lesions or to dedifferentiation. Furthermore, according to the literature data, the sensitivity of these methods in detecting recurrent MTC increases in patients with higher calcitonin levels and lower calcitonin doubling times [41].
This meta-analysis had some limitations related to possible publication bias and heterogeneity between the studies. Publication bias is a major concern in all forms of pooled analysis, because studies reporting significant findings are more likely to be published than those reporting non-significant results. Indeed, it is not unusual for small-sized early studies to report positive relationships that subsequent larger studies fail to replicate. We cannot exclude a publication bias in our analysis, but we tried to minimize such a bias by excluding case reports and small case series from the analysis.
Heterogeneity between studies may be a potential source of bias; the studies included were statistically heterogeneous in their estimates of sensitivity but homogeneous with regard to specificity. Because systematic reviews bring together studies that are different both clinically and methodologically, heterogeneity in their results is to be expected. For example, heterogeneity is likely to arise through diversity in methodological aspects, study quality, inclusion criteria and differences between the patients included. However, such variability was accounted for in the random effect model.
As regards the methodological heterogeneity between the included studies, some authors used carbidopa pretreatment before [18F]DOPA PET examination; this drug, decreasing decarboxylation and subsequent renal clearance of DOPA, may be used to increase the tumor-to-background uptake ratio in patients with NETs [42].
Hybrid PET/CT imaging is usually superior to PET alone in terms of diagnostic accuracy of tumor imaging; our analysis did not evaluate a possible advantage of PET/CT versus PET alone because the numbers were too small to allow the detection of a significant difference. Furthermore, some studies performed both PET and PET/CT and separate data could not be retrieved.
At present, besides [18F]DOPA PET/CT, the most widely used PET technique for NET imaging is somatostatin receptor (SSR) PET/CT using Gallium-68-somatostatin analogs (DOTA-NOC, DOTA-TOC or DOTA-TATE), which shows high diagnostic accuracy in this setting, as demonstrated by a recent meta-analysis [43]; in fact, the use of F-18-FDG should be limited to poorly differentiated tumors [4, 44, 45]. The real problem for the physician is how to select an appropriate radiopharmaceutical in clinical practice. [18F]DOPA and Gallium-68-somatostatin analogs selectively depict different functional characteristics of neuroendocrine cells; thus, for well-differentiated NETs, the decision should be guided by the biology of NETs. The peculiar features of NETs, taking up and decarboxylating l-DOPA and transforming it into dopamine, make [18F]DOPA particularly suited to visualizing tumors with high metabolic activity such as Pheo/PGL and carcinoid tumors with elevated serotonin levels. In the case of Gallium-68-somatostatin analogs, the receptor-based uptake mechanism allows NET lesions to be visualized independently of their functional activity. Moreover, Gallium-68-somatostatin analogs allow patients to be selected prior to peptide receptor radionuclide therapy. The few studies comparing SSR and [18F]DOPA PET/CT in patients with gastroenteropancreatic and thoracic NETs showed an overall superiority of SSR PET/CT compared to [18F]DOPA [14, 15, 46]. Nevertheless, separate comparison studies taking into account the different location of gastroenteropancreatic and thoracic NETs are needed to confirm the superiority of SSR PET/CT over [18F]DOPA in this setting.
To date, there are no significant data on the comparison of SSR and [18F]DOPA PET/CT in patients with Pheo/PGL; instead, there is one study comparing SSR and [18F]DOPA PET/CT in patients with recurrent MTC, which showed the superiority of [18F]DOPA over SSR PET/CT in this setting [38]. More head-to-head comparison studies between SSR and [18F]DOPA PET/CT are needed to address the choice of PET radiopharmaceuticals for evaluating NETs in clinical practice.
Conclusions
Evidence-based data from our analysis show that [18F]DOPA PET and PET/CT are accurate methods in patients with proven or suspected NETs, taking into account the histological type of NET and the clinical setting. Large prospective multicenter studies are necessary to substantiate the diagnostic accuracy of [18F]DOPA PET and PET/CT in the different types of NETs.
References
Solcia E, Kloppel G, Sobin L (2000) Histological typing of the endocrine tumours, 2nd edn. Springer, Berlin
Volante M, Righi L, Berruti A, Rindi G, Papotti M (2011) The pathological diagnosis of neuroendocrine tumors: common questions and tentative answers. Virchows Arch 458:393–402
Rindi G (2010) The ENETS guidelines: the new TNM classification system. Tumori 96:806–809
Rufini V, Calcagni ML, Baum RP (2006) Imaging of neuroendocrine tumors. Semin Nucl Med 36:228–247
Wong KK, Arabi M, Zerizer I, Al-Nahhas A, Rubello D, Gross MD (2011) Role of positron emission tomography/computed tomography in adrenal and neuroendocrine tumors: fluorodeoxyglucose and nonfluorodeoxyglucose tracers. Nucl Med Commun 32:764–781
Jager PL, Chirakal R, Marriott CJ, Brouwers AH, Koopmans KP, Gulenchyn KY (2008) 6-l-18F-fluorodihydroxyphenylalanine PET in neuroendocrine tumors: basic aspects and emerging clinical applications. J Nucl Med 49:573–586
Whiting PF, Weswood ME, Rutjes AW, Reitsma JB, Bossuyt PN, Kleijnen J (2006) Evaluation of QUADAS, a tool for the quality assessment of diagnostic accuracy studies. BMC Med Res Methodol 6:9
Zamora J, Abraira V, Muriel A, Khan K, Coomarasamy A (2006) Meta-DiSc: a software for meta-analysis of test accuracy data. BMC Med Res Methodol 6:31
Lopci E, Piccardo A, Nanni C, Altrinetti V, Garaventa A, Pession A, Cistaro A, Chiti A, Villavecchia G, Fanti S (2012) 18F-DOPA PET/CT in neuroblastoma: comparison of conventional imaging with CT/MR. Clin Nucl Med 37:e73–78
Piccardo A, Lopci E, Conte M, Garaventa A, Foppiani L, Altrinetti V, Nanni C, Bianchi P, Cistaro A, Sorrentino S, Cabria M, Pession A, Puntoni M, Villavecchia G, Fanti S (2012) Comparison of 18F-dopa PET/CT and 123I-MIBG scintigraphy in stage 3 and 4 neuroblastoma: a pilot study. Eur J Nucl Med Mol Imaging 39:57–71
Zemskova MS, Gundabolu B, Sinaii N, Chen CC, Carrasquillo JA, Whatley M, Chowdhury I, Gharib AM, Nieman LK (2010) Utility of various functional and anatomic imaging modalities for detection of ectopic adrenocorticotropin-secreting tumors. J Clin Endocrinol Metab 95:1207–1219
Hoegerle S, Altehoefer C, Ghanem N, Koehler G, Waller CF, Scheruebl H, Moser E, Nitzsche E (2001) Whole-body 18F dopa PET for detection of gastrointestinal carcinoid tumors. Radiology 220:373–380
Koopmans KP, Neels OC, Kema IP, Elsinga PH, Sluiter WJ, Vanghillewe K, Brouwers AH, Jager PL, de Vries EG (2008) Improved staging of patients with carcinoid and islet cell tumors with 18F-dihydroxy-phenyl-alanine and 11C-5-hydroxy-tryptophan positron emission tomography. J Clin Oncol 26:1489–1495
Ambrosini V, Tomassetti P, Castellucci P, Campana D, Montini G, Rubello D, Nanni C, Rizzello A, Franchi R, Fanti S (2008) Comparison between 68Ga-DOTA-NOC and 18F-DOPA PET for the detection of gastro-entero-pancreatic and lung neuro-endocrine tumours. Eur J Nucl Med Mol Imaging 35:1431–1438
Haug A, Auernhammer CJ, Wängler B, Tiling R, Schmidt G, Göke B, Bartenstein P, Pöpperl G (2009) Intraindividual comparison of 68Ga-DOTA-TATE and 18F-DOPA PET in patients with well-differentiated metastatic neuroendocrine tumours. Eur J Nucl Med Mol Imaging 36:765–770
Kauhanen S, Seppänen M, Ovaska J, Minn H, Bergman J, Korsoff P, Salmela P, Saltevo J, Sane T, Välimäki M, Nuutila P (2009) The clinical value of [18F]fluoro-dihydroxyphenylalanine positron emission tomography in primary diagnosis, staging, and restaging of neuroendocrine tumors. Endocr Relat Cancer 16:255–265
Montravers F, Kerrou K, Nataf V, Huchet V, Lotz JP, Ruszniewski P, Rougier P, Duron F, Bouchard P, Grangé JD, Houry S, Talbot JN (2009) Impact of fluorodihydroxyphenylalanine-18F positron emission tomography on management of adult patients with documented or occult digestive endocrine tumors. J Clin Endocrinol Metab 94:1295–1301
Schiesser M, Veit-Haibach P, Muller MK, Weber M, Bauerfeind P, Hany T, Clavien PA (2010) Value of combined 6-[18F]fluorodihydroxyphenylalanine PET/CT for imaging of neuroendocrine tumours. Br J Surg 97:691–697
Yakemchuk VN, Jager PL, Chirakal R, Reid R, Major P, Gulenchyn KY (2012) PET/CT using 18F-FDOPA provides improved staging of carcinoid tumor patients in a Canadian setting. Nucl Med Commun 33:322–330
Hoegerle S, Nitzsche E, Altehoefer C, Ghanem N, Manz T, Brink I, Reincke M, Moser E, Neumann HP (2002) Pheochromocytomas: detection with 18F DOPA whole body PET–initial results. Radiology 222:507–512
Hoegerle S, Ghanem N, Altehoefer C, Schipper J, Brink I, Moser E, Neumann HP (2003) 18F-DOPA positron emission tomography for the detection of glomus tumours. Eur J Nucl Med Mol Imaging 30:689–694
Taïeb D, Tessonnier L, Sebag F, Niccoli-Sire P, Morange I, Colavolpe C, De Micco C, Barlier A, Palazzo FF, Henry JF, Mundler O (2008) The role of 18F-FDOPA and 18F-FDG-PET in the management of malignant and multifocal phaeochromocytomas. Clin Endocrinol 69:580–586
Imani F, Agopian VG, Auerbach MS, Walter MA, Imani F, Benz MR, Dumont RA, Lai CK, Czernin JG, Yeh MW (2009) 18F-FDOPA PET and PET/CT accurately localize pheochromocytomas. J Nucl Med 50:513–519
Fiebrich HB, Brouwers AH, Kerstens MN, Pijl ME, Kema IP, de Jong JR, Jager PL, Elsinga PH, Dierckx RA, van der Wal JE, Sluiter WJ, de Vries EG, Links TP (2009) 6-[F-18]Fluoro-l-dihydroxyphenylalanine positron emission tomography is superior to conventional imaging with (123)I-metaiodobenzylguanidine scintigraphy, computer tomography, and magnetic resonance imaging in localizing tumors causing catecholamine excess. J Clin Endocrinol Metab 94:3922–3930
Timmers HJ, Chen CC, Carrasquillo JA, Whatley M, Ling A, Havekes B, Eisenhofer G, Martiniova L, Adams KT, Pacak K (2009) Comparison of 18F-fluoro-L-DOPA, 18F-fluoro-deoxyglucose, and 18F-fluorodopamine PET and 123I-MIBG scintigraphy in the localization of pheochromocytoma and paraganglioma. J Clin Endocrinol Metab 94:4757–4767
Luster M, Karges W, Zeich K, Pauls S, Verburg FA, Dralle H, Glatting G, Buck AK, Solbach C, Neumaier B, Reske SN, Mottaghy FM (2010) Clinical value of 18F-fluorodihydroxyphenylalanine positron emission tomography/computed tomography (18F-DOPA PET/CT) for detecting pheochromocytoma. Eur J Nucl Med Mol Imaging 37:484–493
Fottner C, Helisch A, Anlauf M, Rossmann H, Musholt TJ, Kreft A, Schadmand-Fischer S, Bartenstein P, Lackner KJ, Klöppel G, Schreckenberger M, Weber MM (2010) 6-18F-fluoro-l-dihydroxyphenylalanine positron emission tomography is superior to 123I-metaiodobenzyl-guanidine scintigraphy in the detection of extraadrenal and hereditary pheochromocytomas and paragangliomas: correlation with vesicular monoamine transporter expression. J Clin Endocrinol Metab 95:2800–2810
Charrier N, Deveze A, Fakhry N, Sebag F, Morange I, Gaborit B, Barlier A, Carmona E, De Micco C, Garcia S, Mancini J, Palazzo FF, Lavieille JP, Zanaret M, Henry JF, Mundler O, Taïeb D (2011) Comparison of [¹¹¹In]pentetreotide-SPECT and [18F]FDOPA-PET in the localization of extra-adrenal paragangliomas: the case for a patient-tailored use of nuclear imaging modalities. Clin Endocrinol (Oxf) 74:21–29
Rufini V, Treglia G, Castaldi P, Perotti G, Calcagni ML, Corsello SM, Galli G, Fanti S, Giordano A (2011) Comparison of 123I-MIBG SPECT-CT and 18F-DOPA PET-CT in the evaluation of patients with known or suspected recurrent paraganglioma. Nucl Med Commun 32:575–582
King KS, Chen CC, Alexopoulos DK, Whatley MA, Reynolds JC, Patronas N, Ling A, Adams KT, Xekouki P, Lando H, Stratakis CA, Pacak K (2011) Functional imaging of SDHx-related head and neck paragangliomas: comparison of 18F-fluorodihydroxyphenylalanine, 18F-fluorodopamine, 18F-fluoro-2-deoxy-d-glucose PET, 123I-metaiodobenzylguanidine scintigraphy, and 111In-pentetreotide scintigraphy. J Clin Endocrinol Metab 96:2779–2785
Rischke HC, Benz MR, Wild D, Mix M, Dumont RA, Campbell D, Seufert J, Wiech T, Rössler J, Weber WA, Neumann HP (2012) Correlation of the genotype of paragangliomas and pheochromocytomas with their metabolic phenotype on 3,4-dihydroxy-6-18F-fluoro-l-phenylalanine PET. J Nucl Med 53:1352–1358
Hoegerle S, Altehoefer C, Ghanem N, Brink I, Moser E, Nitzsche E (2001) 18F-DOPA positron emission tomography for tumour detection in patients with medullary thyroid carcinoma and elevated calcitonin levels. Eur J Nucl Med 28:64–71
Beuthien-Baumann B, Strumpf A, Zessin J, Bredow J, Kotzerke J (2007) Diagnostic impact of PET with 18F-FDG, 18F-DOPA and 3-O-methyl-6-[18F]fluoro-DOPA in recurrent or metastatic medullary thyroid carcinoma. Eur J Nucl Med Mol Imaging 34:1604–1609
Beheshti M, Pöcher S, Vali R, Waldenberger P, Broinger G, Nader M, Kohlfürst S, Pirich C, Dralle H, Langsteger W (2009) The value of 18F-DOPA PET-CT in patients with medullary thyroid carcinoma: comparison with 18F-FDG PET-CT. Eur Radiol 19:1425–1434
Marzola MC, Pelizzo MR, Ferdeghini M, Toniato A, Massaro A, Ambrosini V, Fanti S, Gross MD, Al-Nahhas A, Rubello D (2010) Dual PET/CT with (18)F-DOPA and (18)F-FDG in metastatic medullary thyroid carcinoma and rapidly increasing calcitonin levels: Comparison with conventional imaging. Eur J Surg Oncol 36:414–421
Luster M, Karges W, Zeich K, Pauls S, Verburg FA, Dralle H, Glatting G, Buck AK, Solbach C, Neumaier B, Reske SN, Mottaghy FM (2010) Clinical value of 18-fluorine-fluorodihydroxyphenylalanine positron emission tomography/computed tomography in the follow-up of medullary thyroid carcinoma. Thyroid 20:527–533
Kauhanen S, Schalin-Jäntti C, Seppänen M, Kajander S, Virtanen S, Schildt J, Lisinen I, Ahonen A, Heiskanen I, Väisänen M, Arola J, Korsoff P, Ebeling T, Sane T, Minn H, Välimäki MJ, Nuutila P (2011) Complementary roles of 18F-DOPA PET/CT and 18F-FDG PET/CT in medullary thyroid cancer. J Nucl Med 52:1855–1863
Treglia G, Castaldi P, Villani MF, Perotti G, de Waure C, Filice A, Ambrosini V, Cremonini N, Santimaria M, Versari A, Fanti S, Giordano A, Rufini V (2012) Comparison of 18F-DOPA, 18F-FDG and 68Ga-somatostatin analogue PET/CT in patients with recurrent medullary thyroid carcinoma. Eur J Nucl Med Mol Imaging 39:569–580
Verbeek HH, Plukker JT, Koopmans KP, de Groot JW, Hofstra RM, Muller Kobold AC, van der Horst-Schrivers AN, Brouwers AH, Links TP (2012) Clinical relevance of 18F-FDG PET and 18F-DOPA PET in recurrent medullary thyroid carcinoma. J Nucl Med 53:1863–1871
Montravers F, Grahek D, Kerrou K, Ruszniewski P, de Beco V, Aide N, Gutman F, Grangé JD, Lotz JP, Talbot JN (2006) Can fluorodihydroxyphenylalanine PET replace somatostatin receptor scintigraphy in patients with digestive endocrine tumors? J Nucl Med 47:1455–1462
Treglia G, Rufini V, Salvatori M, Giordano A, Giovanella L (2012) PET imaging in recurrent medullary thyroid carcinoma. Int J Mol Imaging 2012:324686
Timmers HJ, Hadi M, Carrasquillo JA, Chen CC, Martiniova L, Whatley M, Whatley M, Ling A, Eisenhofer G, Adams KT, Pacak K (2007) The effects of carbidopa on uptake of 6-18F-fluoro-l-DOPA in PET of pheochromocytoma and extraadrenal abdominal paraganglioma. J Nucl Med 48:1599–1606
Treglia G, Castaldi P, Rindi G, Giordano A, Rufini V (2012) Diagnostic performance of Gallium-68 somatostatin receptor PET and PET/CT in patients with thoracic and gastroenteropancreatic neuroendocrine tumours: a meta-analysis. Endocrine 42:80–87
Binderup T, Knigge U, Loft A, Federspiel B, Kjaer A (2010) 18F-fluorodeoxyglucose positron emission tomography predicts survival of patients with neuroendocrine tumors. Clin Cancer Res 16:978–985
Rufini V, Baum RP, Castaldi P, Treglia G, De Gaetano AM, Carreras C, Kaemmerer D, Hommann M, Hörsch D, Bonomo L, Giordano A (2012) Role of PET/CT in the functional imaging of endocrine pancreatic tumors. Abdom Imaging 37:1004–1020
Putzer D, Gabriel M, Kendler D, Henninger B, Knoflach M, Kroiss A, Vonguggenberg E, Warwitz B, Virgolini IJ (2010) Comparison of (68)Ga-DOTA-Tyr(3)-octreotide and (18)F-fluoro-l-dihydroxyphenylalanine positron emission tomography in neuroendocrine tumor patients. Q J Nucl Med Mol Imaging 54:68–75
Acknowledgments
The authors thank Professor Jean-Noël Talbot MD, PhD (of the Department of Nuclear Medicine, Tenon Hospital of Paris, France) for his valuable suggestions and the critical revision of this manuscript.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rufini, V., Treglia, G., Montravers, F. et al. Diagnostic accuracy of [18F]DOPA PET and PET/CT in patients with neuroendocrine tumors: a meta-analysis. Clin Transl Imaging 1, 111–122 (2013). https://doi.org/10.1007/s40336-013-0005-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40336-013-0005-3