
Abstract
Background
Expenditure on medicines is a readily identifiable element of health service costs. It is the focus of much attention by payers, not least in the UK even though the cost of medicines represents less than 10 % of total UK National Health Service (NHS) expenditure. Projecting future medicines spending enables the likely cost pressure to be allowed for in planning the scale and allocation of NHS resources. Simple extrapolations of past trends in expenditure fail to account for changes in the rate and mix of new medicines becoming available and in the scope for windfall savings when some medicines lose their patent protection. The objective of this study is to develop and test an improved method to project NHS pharmaceutical expenditure in the UK for the period 2012–2015.
Methods
We have adopted a product-by-product, bottom-up approach, which means that our projections are built up from individual products to the total market. Our projections of the impact of generic and biosimilars entry on prices and quantities of medicines sold, and of the rate of uptake of newly launched medicines, have been obtained from regression analysis of UK data. To address uncertainty, we have created a baseline and two other illustrative scenarios. We have compared our projections with actual expenditure for 2012.
Results
Our projections estimate that, between 2011 and 2015, with no change in policy or price regulation, the UK total medicines bill would increase at an average compound annual growth rate (CAGR) of between 3.1 and 4.1 %. Total NHS spending on branded medicines and total NHS spending on generics are projected to increase at average CAGRs of 0.5–1.8 and 10.0–11.0 %, respectively, over the same time period. For the total market, the actual growth rate for 2012 lay within our projected range.
Conclusions
Our methodology provides a useful framework for projecting UK NHS medicines expenditure over the medium term and captures the impacts of existing medicines losing exclusivity and of new medicines being launched onto the market.






Similar content being viewed by others


Notes
Authors’ analysis based on IMS (IMS BPI and HPAI).
Authors’ analysis based on IMS (IMS BPI and HPAI).
A paediatric investigation plan (PIP) is a development plan aimed at ensuring that the necessary data are obtained through studies in children, when it is safe to do so, to support the authorisation of a medicine for children.
Details are available on request.
Easy formulations are tablets, capsules, pastilles, retard tabs, dispersible tabs, soluble tabs, solutions, bottles. Difficult formulations were all other formulations, e.g. syringes, vials, cartridges, pens, patches, ampoules, creams, ointments, gels, suspensions, eye drops, diskhalers, accuhalers, inhalers, powders. These were determined using expert input from companies that manufacture medicines.
References
Hawe E, Yuen P, Baillie L. OHE guide to UK health and health care statistics. London: Office of Health Economics; 2011.
EFPIA. Statistics tables. Brussels: The European Federation of Pharmaceutical Industries and Associations; 2013.
Mason A. New medicines in primary care: a review of influences on general practitioner prescribing. J Clin Pharm Therap. 2008;33(1):1–10.
Chauhan D, Mason A. Factors affecting the uptake of new medicines in secondary care – a literature review. J Clin Pharm Therap. 2008;33(4):339–48.
Richards M (2012) Extent and causes of international variations in drug usage. A report for the Secretary of State for Health, London.
Puig-Junoy J. The impact of European pharmaceutical price regulation on generic price competition. Pharmacoeconomics. 2010;28(8):649–63.
Reiffen D, Ward M. Generic drug industry dynamics. Rev Econ Stat. 2005;87(1):37–49.
Saha A, Grabowski H, Birnbaum H, Greenberg P, Bizan O. Generic competition in the US pharmaceutical industry. Int J Econ Bus. 2006;13(1):15–38.
Grabowski H, Kyle M. Generic competition and market exclusivity periods in pharmaceuticals. Manag Dec Econ. 2007;28(4–5):491–502.
Mestre-Ferrandiz J. El mercado de medicamentos genéricos: regulación ‘versus’ competencia. ¿Qué podemos aprender de la experiencia internacional? Spanish. J Health Econ. 2007;6(1):33–6.
Thiébaut SP, Barnay T, Ventelou B. Ageing, chronic conditions and the evolution of future drugs expenditure: a five-year micro-simulation from 2004 to 2029. Appl Econ. 2013;45(13):1663–72.
Keehan SP, Sisko AM, Truffer CJ, Poisal JA, Cuckler GA, Madison AJ, Lizonitz JM, Smith SD. National health spending projections through 2020: economic recovery and reform drive faster spending growth. Health Affairs. 2011;30(8):1594–605.
Connor P, Alldus C, Ciapparelli C, Kirby L. Long-term pharmaceutical forecasting: IMS Health’s experience. J Bus Forecast. 2003;22(4):10–5.
Hoffman JM, Li E, Doloresco F, Matusiak L, Hunkler RJ, Shah ND, Vermeulen LC, Schumock GT. Projecting future drug expenditures. Am J Health Syst Pharm. 2012;69(5):405–21.
Wettermark B, Persson ME, Wilking N, Kalin M, Korkmaz S, Hjerndahl P, Godman B, Petzold M, Gustafson LL. Forecasting drug utilization and expenditure in a metropolitan health region. BMC Health Serv Res. 2010;10:128.
IMS (2013) World review executive. London: IMS Health.
Lloyd D. Prescriptions dispensed in the community: England, statistics for 2001 to 2011. London: The Health and Social Care Information Centre; 2011.
Duerden M, Hughes D. Generic and therapeutic substitutions in the UK: are they a good thing? Br J Clin Pharmacol. 2010;70(3):335–41.
Bennie M, Godman B, Bishop I, Campbell S. Multiple initiatives continue to enhance the prescribing efficiency for the proton pump inhibitors and statins in Scotland. Exp Rev Pharmacoecon Outcomes Res. 2012;12:125–30.
ABPI and DH (The Association of the British Pharmaceutical Industry and Department of Health) (2008) The Pharmaceutical Price Regulation Scheme 2009. London: Department of Health. http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_098498.pdf. Accessed 20 March 2013.
Department of Health (2011) A new value-based approach to the pricing of branded medicines—government response to consultation. London: Department of Health.
DH (Department of Health) (2012) The cancer drugs fund—guidance to support operation of the cancer drugs fund in 2012–13. London: Department of Health. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_133682. Accessed 20 March 2013.
Chauhan D, Towse A, Mestre-Ferrandiz J (2008) The market for biosimilars: evolution and policy options. OHE briefing (45). London: Office of Health Economics.
Rickwood S, Iervolino A. Shaping the biosimilars opportunity: a global perspective on the evolving biosimilars landscape. London: IMS Health; 2011.
Rovira J, Espin J, Garcia L, Orly de Labry A (2011) The impact of biosimilars’ entry in the EU market. Report prepared for the EC (DG Enterprise and Industry). http://ec.europa.eu/enterprise/sectors/healthcare/files/docs/biosimilars_market_012011_en.pdf. Accessed 9th July 2011.
Simoens S. Biosimilar medicines and cost-effectiveness. ClinicoEcon Outcomes Res. 2011;3:29–36.
Höer C, Häussler B, Haustein R. Saving money in the European healthcare systems with biosimilars. Gen Biosimilars Initiative J (GaBI J). 2012;1(3–4):120–6.
Paul S, Mytelka D, Dunwiddie C, Persinger C, Munos B, Lindborg S, Schacht A. How to improve R&D productivity: the pharmaceutical industry’s grand challenge. Nature Rev Drug Discov. 2010;9(3):203–14.
DH and ABPI (Department of Health and The Association of the British Pharmaceutical Industry) (2002) PPRS: the study into the extent of competition in the supply of branded medicines to the NHS, component 3: competition in the out-of-patent sector. London: Department of Health. http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/Browsable/DH_5024085. Accessed 20 March 2013.
Dranitsaris G, Amir E, Dorward K. Biosimilars of biological drug therapies: regulatory, clinical and commercial considerations. Drugs. 2011;71(12):1527–36.
Mellstedt H. The future of biosimilars. Hosp Pharm Europe. 2010;49:33–3.
Blackstone E, Fuhr J. Biopharmaceuticals: the economic equation. Biotechnol Healthc. 2007;4(6):41–5.
Rovira J, Espin J, Garcia L, Orly de Labry A (2011) The impact of biosimilars’ entry in the EU market. Report prepared for the EC (DG Enterprise and Industry. Granada: Andalusian School of Public Health. http://ec.europa.eu/enterprise/sectors/healthcare/files/docs/biosimilars_market_012011_en.pdf. Accessed 10th Dec 2012.
Acknowledgments
We are grateful to IMS for permission to use their data. We are also grateful to Geoff Bailey, Alison Clough, Rob Day, Ayesha Kanji, John Kearney, Sol Magaz, Pedro Pita-Barros, Tricia Porter and Tim Williams for helpful feedback and comments on earlier drafts and on the methodology used. PO was in charge of extracting the raw IMS data, created the excel spreadsheet with all the calculations, was involved in the discussions with the experts and led the writing of the manuscript; JM-F project managed the entire project, took the lead in liaising with the experts and contributed to the writing; RP-P did the historical analysis for LOE and uptake, was involved in the discussions with the experts and contributed to the writing; JS reviewed related academic and policy literature, contributed to the writing and provided overall quality assurance to the project. The overall guarantor is JM-F.
Financial disclosure
The Office of Health Economics (OHE) receives research and consulting funding from the Association of the British Pharmaceutical Industry (ABPI). No separate funding was received for this study and manuscript. PO, JM-F and JS are all employees of the OHE. RP-P is a former employee of the OHE and now is an employee of CRES, Barcelona.
Author information
Authors and Affiliations
Corresponding author
Projecting Expenditure on Medicines in the UK NHS: Technical Appendix
Projecting Expenditure on Medicines in the UK NHS: Technical Appendix
1.1 Introduction
This technical appendix provides more detail on the methodology used for our projections for expenditure on medicines in the UK NHS for 2012–2015. As highlighted in the main article, a number of analyses were undertaken. Before explaining them, we provide the framework used for our analysis. We then outline our methodology for the following key components of the model: identification of core therapy areas; new medicines projected to become available between 2012 and 2015; medicines launched between 2007 and 2011; and products expected to face generic and biosimilar competition between 2012 and 2015.
1.2 Framework: Factors Affecting Prices and Use of Medicines
A number of identifiable supply and demand factors affect usage and degree of price competition between medicines across their life cycles. Figure 7 shows the underlying structure of these factors.

Factors affecting prices and use of medicines: structure
At a general level, major demand-side aspects in the UK are assumed constant, as we do not directly model price demand elasticity and income demand elasticity (i.e. what happens to quantity demanded when the price of a medicine changes and when income changes, respectively). On the supply side, and in particular with respect to how pharmaceutical companies interact, the importance of having more or fewer competitors, and the impacts of marketing and detailing efforts, are not modelled directly. However, as described below, all of these interactions are incorporated indirectly when trying to project sales at individual product level.
1.3 Core Therapeutic Areas
To identify core therapeutic areas, we extracted primary and secondary care sales for 2010 and 2011 by ATC4 class from IMS data. The ATC Classification System is used for the classification of drugs. In this system, drugs are classified into groups at five different levels. ATC1 is the first level of the code and indicates the anatomical main group and consists of one letter. The second level of the code indicates the therapeutic main group and consists of two digits. The third level of the code indicates the therapeutic/pharmacological subgroup and consists of one letter. The fourth level of the code (ATC4) indicates the chemical/therapeutic/pharmacological subgroup and consists of one letter. The fifth level of the code indicates the chemical substance and consists of two digits. ATC1 classes that experienced growth or shrinkage greater than ±10 % in 2011 compared with 2010, or that had greater than a 10 % market share by value in 2011, were nominated as core classes.
These threshold percentages were chosen so that the core areas cover around 80 % of the market to make the analysis reliable while still being manageable. In 2011, core classes comprised more than 80 % of the UK NHS medicines bill by value. Table 6 shows the core (with a ‘y’ in the second column) and non-core therapeutic areas (with an ‘n’ in the second column).
1.4 New Products
To project expenditure on medicines launched onto the UK market during the projection period, two key elements are essential:
-
1.
Identify which drugs should be expected to be launched in the UK between 2012 and 2015.
-
2.
Place them in uptake curves, i.e. how fast use of them will grow.
For the second step, we carried out a historical analysis looking at uptake of products launched in the UK for the period 2003–2010.
The data supporting the analysis for point (1) are based on the IMS Lifecycle R&D Focus, which is a proprietary comprehensive database that tracks progress of R&D of medicines by molecule and indication. It provides data on the current phase of the R&D process of the medicine and indication and the ATC therapeutic area for that indication. An extract of the complete database was taken in March 2012. The number of projects at each stage of the R&D pipeline was collected and matched to an ATC therapeutic area. In order to estimate the number of new products launched per projection year per therapeutic area, we used information provided by Paul et al. [28] on attrition rates and development times by phase. By applying these to the collated pipeline data, we estimated the number of launches for each therapeutic area per year for the forecast period. These projected launch rates then were compared with recent rates of launches and further validated by our industry experts. Table 7 shows our estimates of new launches per projection year.
To generate assumed uptake curves for these future launches, we analysed IMS data for past new launches in the period 2003–2010. Uptake curves were estimated both across the whole sample and at therapeutic level for particular core therapeutic areas and subsets: alimentary, anti-infectives HIV, cancer, cardiovascular, central nervous system and respiratory. Disease-specific uptake curves for key classes were also validated with experts, but none was changed as a result. Table 8 details the numbers of products included in the analysis by therapeutic area. In total, we analysed the uptake of 367 new medicines that were launched in the UK between 2003 and 2010.
Uptake curves represent the ratio of each subsequent year’s sales (by value) with respect to the first year of sales after launch. For instance, the ratio in year 2 (denoted as r 2), would be equal to year 2 sales divided by year 1 sales; the ratio in year 3 would be equal to year 3 sales divided by year 1 sales, and so forth. Thus, if the ratio r 2 = 2, this indicates that year 2 sales are twice as high as year 1 sales. We calculated these ratios up to year 6.
The results of this analysis are plotted in Figs. 8 and 9. Figure 8 identifies classes where the ratios were greater than the average rates for the total sample of products. Figure 9 shows classes where uptake was slower than the average for the total sample.

2003–2010 average UK uptake curves for all new products and for those classes where relative uptake was greater than the average for all new products. Source: authors’ estimates from IMS BPI and HPAI 2002–2011 data

2003–2010 average UK uptake curves for all new products and for those classes where relative uptake was less than the average for all new products. Source: authors’ estimates from IMS BPI and HPAI 2002–2011 data
Note that for a number of classes (cancer in Fig. 8 and anti-infectives and alimentary in Fig. 9), we can observe some declines in years 5 and 6. We have not explored the reasons for these. However, we do not use the results for these years in our analysis as we only use up to year 4 for the new product launches in 2012, because our projections go to 2015.
Given that our uptake analyses uses year 1 sales as the anchor point, the final component of the new product analysis was to estimate the (average) first year sales of recent historical launches, by therapeutic area. This was achieved using the data generated to calculate uptake curves. These first year figures were also validated by therapeutic area experts; as a result of their feedback, some subclasses were excluded from the analysis as they were deemed outliers, and including them would skew the results for future launches. The values used in the model are detailed in Table 9.
We also explored whether sales of new products wholly or partially replace sales of existing medicines, i.e. whether they substitute for older medicines or are additional sales. To explore this substitution effect, we undertook a historical analysis in four therapeutic areas that have had few new launches in recent years: HIV, diabetes, multiple sclerosis and epilepsy. We followed the same methodology across these four areas to explore whether sales of new products can be deemed to be fully additive or to, at least partly, replace older products. For each disease area, we estimated the average annual growth rate for the period 2003–2006 for branded medicines. Using this linear growth rate, we projected 2007–2011 sales as if new launches did not happen for this period and held all other things constant. We then compared our ‘projected’ sales with actual sales (for the period 2007–2011) to explore the degree of additional sales caused by new launches; in essence, the difference between the two curves could be thought of as the effect of new launches between 2007 and 2011.
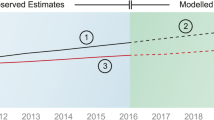
For brevity, we only include below the specific analysis for HIV and epilepsy, as these are the two extremes (results for diabetes and multiple sclerosis lie in between these two areas). Figures 10 and 11 show the analysis for HIV and epilepsy, respectively.

Net impact of new launches: HIV case study. Source: authors’ calculations from IMS BPI and HPAI 2002–2011 data
The blue line represents the projections for 2007–2011 assuming no new launches in this period, based on the average annual growth rate for the period 2003–2006. The red line shows actual sales for this period. Three new products were launched in the UK between 2007 and 2011 for the treatment of HIV. Summing across 2007 and 2011, the difference between actual and projected sales was £82 million, which represents 4.6 % of the total projected sales. In this case, it seems that the impact of launches had a small net effect on the HIV market. Indeed, we can observe that by in 2011 ‘actual’ branded sales are below ‘projected branded sales’ so under this approach there is even more than complete substitution of new medicines for old for this year (i.e. a negative effect).
Figure 11 should be read in the same way as Fig. 10. Four new products were launched in the UK between 2007 and 2011 for the treatment of epilepsy. Summing across 2007–2011, the difference between actual and projected sales over this period was £219 million, which represents 84 % of the total projected sales. In this case, new products for epilepsy had an important net effect on the size of this market.

Net impact of new launches: epilepsy case study. Source: authors’ calculations from IMS BPI and HPAI 2002–2011 data
For diabetes and multiple sclerosis (details not shown here), the respective percentages were 23 and 33 %. The unweighted average across the four therapeutic areas analysed is 36 %, which is the same as the weighted average by 2011 actual sales. Weighting by 2007 actual sales decreases the average to 33 %.
1.5 LOE Products: Impact of Loss of Patent Expiry and Generic Competition
We have constructed four (price and volume) erosion curves, depending on manufacturing complexity (‘easy’ or ‘difficult’) and channel (primary or secondary care), based on historical analysis of the UK market.
For the purposes of our analysis, LOE was defined as occurring (1) when an on-patent medicine loses legal protection to benefit exclusively from the intellectual property rights associated with all patents related to the medicine; and (2) when at least one other manufacturer is supplying a generic equivalent to the market.
To model the future impact of LOE for medicines expected to face generic entry between 2012 and 2015, each medicine by formulation was assigned an LOE date and a price and volume erosion curve. Total (branded plus generic) volumes for each product were trended through the projection period.
The second condition is necessary to identify actual, rather than potential, generic entry. We have detailed patent expiry dates between 2012 and 2015, based on IMS BPI and HPAI. As part of the validation process of patent expiry dates, we also asked our industry experts to validate these dates. Our patent expiry dates include paediatric investigation plan (PIP) extensionsFootnote 3 awarded up to September 2012.Footnote 4 We have used the observed impact of generic competition in the UK in recent years to project the impact of future patent expiries.
1.5.1 Primary Care
For primary care medicines, patent expiries over the period 2002–2011 were modelled and grouped by ATC1 class. Formulations were identified as being either difficult or easy to manufactureFootnote 5 because this is a key determinant of the degree of competition from generic alternatives—higher in the case of easy-to-manufacture formulations [29]. Indeed, as shown in Figs. 12 and 13, the erosion curves are different.
For some cardiovascular and anti-Alzheimer’s drugs that will lose their exclusivity in the projection period, alternative curves have been applied, based on historical analysis and expert input. In particular, for these two therapeutic areas, we used more aggressive erosion curves; for cardiovascular, this was based on the actual degree of generic competition faced by simvastatin, which was the first statin to face generic competition. Simvastatin became off-patent in 2002, providing information on the effect of generic entry in the UK. For anti-Alzheimer’s drugs, and in particular cholinesterase inhibitors, the first of which came off patent in late 2011, we were able to monitor the actual degree of generic competition and found it to be significantly more aggressive than the average erosion curves estimated above. As a result, we have used more aggressive erosion curves. These specific erosion curves are shown in Table 11.
The price of a counting unit for each product in primary care is estimated by dividing the value of sales in pounds sterling by volumes in counting units. We then estimated the price erosion curve for each branded product and type of formulation (easy and difficult) as the average price of generic product(s) for a given year with respect to the price of the branded product the year before a generic enters the market. Algebraically:
We then estimated the weighted average price erosion curve in our sample. As weights we use sales of the branded products the year before generic entry to account for the fact that the sample is populated by products with very different levels of sales. In this way, the products with greater sales have a heavier weight in the average price erosion curve.
Volume curves are estimated for each branded product and type of formulation (easy and difficult) as the proportion of sales in counting units of that molecule that is retained by the branded product for each year until year 6 of sales:
We then estimate the weighted average volume erosion curve in our sample using the same weights as in the price erosion curve. Table 10 and Fig. 12 show our results.

Volume and price erosion curves in primary care. Source: authors’ calculations from IMS BPI and HPAI (2002–2011)
Based on Fig. 12, the off-patent, easy-to-manufacture, branded medicine keeps 51 % of the market share in year 1, on average; the remaining 49 % will go to generic equivalents. By year 5 after patent expiry, the market share retained by the originator falls to 10 % (and 30 % when it is a ‘difficult-to-manufacture’ molecule).
Figure 12 also shows how the price of generics relative to the originator brand’s price pre-LOE evolves. For instance, for easy formulations, we estimate that in year 1 of generic competition, the generic price is 10 % lower than the originator price was pre-LOE. By year 5, this discount is 86 %. Table 11 shows the specific erosion curves for cardiovascular and some medicines for Alzheimer’s.
For the purposes of our modelling, we have assumed that the price of the branded medicine does not change post-LOE. To validate this assumption, we explored the evolution of prices of branded medicines going off patent since 2008. Figure 13 below plots the price of the 33 medicines that moved off patent since 2008 relative to the price at patent expiry for the first 24 months post-patent expiry. These medicines were on average 97.9 % of the price at patent expiry 24 months post-expiry. This was in the context of a period when companies were required to modulate prices to reduce prices across their portfolio by 5.8 %. As part of the 2009 PPRS agreement, there are regulations governing prices for medicines moving off patent, restricting the amount they can be adjusted in the context of modulation. Figure 13 supports our assumption that prices of branded medicines do not change post-LOE.

Average price change in price of originator medicine post-LOE [33 medicines moved LOE since 2008 (103 formulations)] LOE loss of exclusivity. Source: authors’ calculations from IMS BPI and HPAI (2008–2012)
1.5.2 Secondary Care
We used a different approach for the historical analysis of secondary care medicines facing generic competition because IMS data do not capture accurately what happens to prices post-LOE in secondary care markets. We constructed two case studies representing respectively:
-
An ‘easy to manufacture’ product.
-
A ‘difficult to manufacture’ product.
In each case we asked the respective manufacturer of a branded medicine to provide us with data on real transaction prices and volumes for the off-patent brand and generics in hospitals, based on the manufacturers’ own internal data. Based on this information, we then constructed (anonymised) price and volume erosion curves.
We then used a panel of four NHS hospital pharmacists to validate our case studies via a Delphi-type process, as follows. In the first round, we provided them with our preliminary erosion curves for the two case studies and asked them the following question: “In your view, are these two case studies a reasonable representation of generic competition in the hospital market?” Based on the feedback received in the first round, we then went back to them with revised curves and asked them to validate the curves. For the ‘easy to manufacture’ curves, the volume erosion curves were unchanged, while the price erosion curve was slightly modified (they argued for more aggressive price competition in the first year than our original estimate and relative stability thereafter). For the ‘difficult to manufacture’ volume erosion curve, no change was required, as they thought our original curve was a good representation. However, regarding the price erosion curve, they argued, relatively to our original curve, for less aggressive price competition in the first 3 years after patent expiry, but more aggressive in the last 2 years.
Figure 14 illustrates the price and volume erosion curves resulting. It should be interpreted similarly to Fig. 12.

Volume and price erosion curves in secondary care. Source: authors’ calculations based on expert input
1.5.3 Biosimilars
Two specific classes of biological medicines in secondary care, anti-TNFs, and MAbs for use in treating cancer, provided specific challenges for forecasting the impact of LOE as they give rise to ‘biosimilars’ rather than exact-copy chemical generics. For biosimilars, we lacked suitable historical parallel examples from which to develop analogues. Even after seeking expert input, we found uncertainty about the future evolution of biosimilar competition in these markets. Although markets exists where biotechnology medicines have faced biosimilar competition—including granulocyte-colony-stimulating-factor medicines, EPOs and growth hormones—expert opinion was that these would not be suitable analogues for the two classes above. The regulatory environment is evolving and investment in biosimilar production capacity by large pharmaceutical producers is growing along with both the size of the markets involved and greater familiarity with biosimilars among prescribers. In total, the value of UK sales for anti-TNFs and MAbs in 2011 was £1 billion (based on IMS sales).
Development costs for biosimilars have been estimated to be considerably higher than for chemical generics, because biosimilars need to conduct pre-clinical and clinical studies. Average cost estimates for biosimilars range from US$100–250 million if plant development is included or US$20–100 million for non-plant cost [24]. For more complex MAbs, costs of up to US$500 million have been projected [30]. Traditional generics’ costs are around US$1–4 million [24]. The developmental time for a generic medicine is around 3 years, whereas this period increases from 6 to 9 years for a biosimilar [31].
In addition, there are some manufacturing issues to consider. While the cost barriers to developing a biosimilars manufacturing capability are not prohibitive, the development of biosimilars involves sophisticated technologies and processes, raising the riskiness of the investment [24].
We cannot therefore expect similar levels of price discounting for biosimilars as for standard chemical generics because of these cost issues. There are three further issues [23]: (1) manufacturers will have to carry out post-authorisation studies, so it would be unrealistic to expect the same rapid speed of adoption as observed with generics following patent expiry of a chemical reference product; (2) manufacturers will need to invest in communicating with prescribers as well as pharmacists as prescribing is by brand name and physician (and pharmacist) concerns about comparability will need to be addressed in post-launch studies [32]; and (3) the number of entrants is a key factor driving price competition in the generics market—the more entrants, the greater the competition [7–9]. Based on the comments above, we can expect fewer biosimilar entrants (relative to generics). These factors help to explain why price differentials (to date) between biosimilars and their originator reference products have not been as substantial as experienced in the traditional, small molecule generic medicine market. Price discounts for biosimilars relative to the originators in Europe between 2007 and 2009 have been between 10–35 % for biosimilars [33]. This is in line with [24]; price reductions in the region of 30 % (measured from average ex-manufacturer list price) have been observed.
Figure 15 plots the volume and price erosion curves for anti-TNFs and MAbs used in our model. They are based on the limited evidence available to date discussed in the previous paragraph on the potential impact of biosimilars for anti-TNFs and MAbs. Anticipated LOE dates for these medicines occur at the end of the projection period (in 2014 and 2015) but, given the size of these markets, any significant changes in prices for these medicines could potentially have a considerable impact on rates of growth for the medicines bill as a whole, especially after 2015.

Anti-TNFs and monoclonal antibodies for cancer: quantity and price erosion curves. Anti-TNF tumour necrosis factor inhibitor. Source: authors’ calculations based on expert input
1.6 Recent Products
All medicines that were launched in the last 5 years, i.e. between 2007 and 2011 inclusive, were placed on relevant uptake curves using the results of the analysis that generated the new product uptake curves (explained above). We use the year-on-year growth rates for values shown in Table 12, which are based on the numbers underpinning our uptake curve across the full sample (i.e. the average). As an illustration, for a product launched in 2009, sales in 2012 (which will be year 3 after launch) will be projected by growing 2011 sales by the year 3 growth rate, 2013 sales by applying year 4 growth rate to 2012 sales, and so forth.
Rights and permissions
About this article
Cite this article
O’Neill, P., Mestre-Ferrandiz, J., Puig-Peiro, R. et al. Projecting Expenditure on Medicines in the UK NHS. PharmacoEconomics 31, 933–957 (2013). https://doi.org/10.1007/s40273-013-0082-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40273-013-0082-1