
Abstract
Background
With the increase in the prevalence of cancer, cancer-related issues also deserve more attention especially in developing countries where there is already limited access to high-quality healthcare. Cancer-related pain, the most common and the most annoying one, is not only a symptom but also an important subspecialty and its management is still challenging.
Objectives
To assess the level of pain and cancer pain knowledge in Iran in comparison with the whole world.
Materials and Method
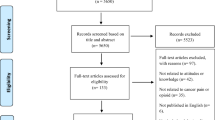
A search of the literature including papers published in PubMed before March 2016 was carried out.
Results
There have been an increasing number of publications on pain since 1842 and a growing number of publications on cancer pain since 1929. There has also been remarkable growth in our understanding of cancer pain, particularly since 2010. More than one-third of studies on pain and cancer-related pain were published after 2010.
Conclusion
There is a need to be more inventive with the management of cancer-related issues, especially pain in developing countries, to maximize the quality and quantity of healthcare delivery to cancer-stricken patients. It seems that non-governmental organizations like MAHAK can play a significant role in this goal.
Similar content being viewed by others


Introduction
Cancer is a relatively neglected disease, as declared by Soyannwo [1], that is still an overriding cause of pain and suffering, especially in developing countries [1–4]. According to the World Health Organization (WHO), 8.2 million people die from more than 100 types of cancer each year [3]. More than half of all new cancer cases occur in developing countries [3, 4], and the incidence of new cancer cases is expected to increase by a further 70% in the next two decades [3–6].
Of all the symptoms experienced by cancer patients, pain is the most common complaint and, at times, patients can find it intense and unbearable [7, 8]. Cancer-related pain on average affects as many as 50–75% of patients worldwide [9–11]. According to a systematic review by van den Beuken-van Everdingen et al. evaluating 54 related articles, 59% of patients undergoing cancer treatment and 64–75% of patients with advanced disease were affected by pain [9]. As such, cancer-related pain is a greater problem during the advanced stages of the disease, which can become the predominant problem for both the patients and their families [10–12].
On the basis of van den Beuken-van Everdingen et al.’s systematic review, more than one-third of cancer patients graded their pain as moderate to severe with a visual analogue scale (VAS) greater than 4 [9]. Likewise, of 258 hospitalized cancer patients interviewed about their pain in a study by Ripamonti et al., more than half experienced it in the 24 h prior to their admission with 27.1% of them regarding it as high degree [11]. Cancer pain of this intensity is highly prevalent in resource-poor countries and this adversely impacts different aspects of sufferers’ lives including psychological, social, cultural, and spiritual facets [13]. Female gender, young age, and prolonged hospitalizations have been associated with increased pain severity [12].
Since the early 1950s, when John Bonica highlighted the importance of pain relief, pain has been recognized, not just as a symptom or sensation but as a disease in itself [14]. With the development of pain medicine as a subspecialty of medical practice in 1989, this domain gained further popularity. Today, failure in the adequate treatment of pain is not only unethical but also illegal [14–16].
Based on WHO guidelines, and depending on the extremity of pain, step by step management begins with oral non-opioid analgesics and progresses through to parenteral opioids, anticonvulsant agents, or local anesthetics [17]. There are also diverse interventional techniques such as spinal analgesia, nerve block, or destructive modalities (like radiofrequency ablation reserved for a minority of patients) [18].
Despite the fact that cost-effective methods for pain care are available, acute and chronic pain is still undertreated in developing countries [13, 19]. There seems to be a large and widening gap between the increasingly sophisticated knowledge of pain and the application of this knowledge to effectively treat patients [16, 18]. Besides the lack of pain management training at both undergraduate and postgraduate levels [20], there are several other barriers to desirable pain alleviation in resource-limited settings, including timely access to healthcare [21] or economic impediments [22]. However, given the overwhelming need to treat cancer-related pain, local advocates have a pivotal role in developing and implementing innovative measures, despite the limited resources available [10, 16, 23, 24]. To overcome the challenges in the management of cancer-related pain in developing countries, it is vital that pain control is embedded in different models of healthcare delivery. The quality of care given must also be strengthened. Both of these needs can be met through the establishment of regional and educationally oriented research centers [10, 16]. This paper offers a concise summary of the studies that have been performed in the field of cancer pain and its management in Iran as one of the developing countries.
Materials and Methods
To assess the level of pain and cancer pain knowledge in Iran, a brief search of the literature including papers published in PubMed before March 2016 (using keywords “pain”, “cancer pain” with/without “Iran”) was carried out. This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Results
The findings illustrated in Figs. 1 and 2 indicate a significant annual progression in studies related to pain and cancer pain. There have been an increasing number of publications on pain since 1842 and a growing number of publications on cancer pain since 1929. In very recent years, there has been remarkable growth our understanding of cancer pain, particularly since 2010. In fact, more than one-third of studies on pain and cancer-related pain were published after 2010.

Progression in pain research, especially in the recent decade

Progression of pain and cancer pain-related knowledge annually. About one-third of pain knowledge was developed since 2010
Discussion
Iran’s contribution to both pain and cancer-related pain research has increased in the last decade. Of the total number of papers originating from Iran, at least according to the PubMed database, 91.8% are related to the last 10 years and more than half (61.7%) are related to the last 5 years. On top of that, the ratio of cancer pain-related papers to the total papers about pain has been around 8% which is slightly less than the corresponding ratio globally (13%). This significant upward trend once more highlights the importance of this topic particularly in developing countries. As a limitation of our study, we knew that there are many databases (Google Scholar, Scopus, EMBASE, etc.) which should be included in a more comprehensive literature review; however, we selected PubMed as one of the most referred to databanks globally. We suggest that new projects be undertaken to write an original or review article in the field of pain research development.
The growing tendency among Iranian anesthesiologists to study and practice in pain medicine spurred the establishment of the Iranian Society of Regional Anesthesia and Pain Medicine (ISRAPM) in November 2006. This society aimed to improve and support scientific and educational activities within this field, and in the last decade, there has been an improvement in pain education and clinical practice in Iran. This has been achieved by providing training through pain fellowships and publishing pain guidelines in Anesthesiology and Pain Medicine.
Pain relief is a human right [17, 18] and as such Iranian pain physicians are now concentrating on performing more native research projects, publishing research articles, and managing pain departments and pain research centers. For example, one of the most distinguished and successful pain departments is at MAHAK hospital, which focuses on pediatric cancer pain. Many different types of cancer have been reported in children admitted to MAHAK’S Pediatric Cancer Treatment and Research Center (MPCTRC) including acute lymphocytic leukemia (ALL), acute myelocytic leukemia (AML) [25], central nervous system tumors such as primitive neuroectodermal tumor (PNET) [26], and soft and hard tissue tumors [27].
MPCTRC is equipped with a wide range of facilities including an operating room, ultrasound, and laser and ozone therapy units. Acute and chronic pain control has become achievable with the help of transcutaneous electrical nerve stimulation (TENS), peripheral and central neural blockade, or epiduroscopy (diagnosis and treatment of epidural space adhesions resulting from spine surgery or tumor invasion). Other interventional pain management techniques accessible at this center include the use of radiofrequency and microwave for modulation, ablation, and coagulation of pain pathways, implantable analgesic pumps in the epidural or intrathecal space, along with botulinum toxin injection therapy (for headaches, muscle pains, and spasms), photodynamic therapy, aromatherapy, and music therapy [28]. There are many disease-based projects undertaken at this center [25–28]. There are also a number of ongoing projects investigating the follow-up of cancer patients since 2014, which are due to be completed by 2020. The number of cancer patients referred to MAHAK since 2008 is shown in Table 1.
Overall, the establishment of MPCTRC has been successful in improving the quality of life in children affected by cancer [28]. As stated by recent studies, each cancer center should be supplied with a specific pain department in order to reduce cancer patients’ distress. This is of significant importance among physicians [28]. MAHAK supports the treatment of cancer-stricken children by providing them with specialized services that still allow them to enjoy their childhood whilst undergoing treatment. This allow the patients to have the highest possible quality of life in accordance with international standards [23, 28].
Conclusion
There is a need to be more inventive with the management of cancer-related issues in developing countries to maximize the use of available tools. With regard to the paucity of knowledge and limited resources in this area, the critical role of the non-governmental organizations, such as MAHAK, should not be overlooked.
References
Soyannwo OA. Cancer pain management for developing countries. IASP. 2009;17(1):1–4.
Hortobagyi GN, El-Saghir NS, Cufer T, et al. The American Society of Clinical Oncology’s efforts to support global cancer medicine. J Clin Oncol. 2016;34(1):76–82.
Stewart BW, Wild CW. World cancer report 2014. Geneva: IARC/World Health Organization; 2014.
Shin HR, Carlos MC, Varghese C. Cancer control in the Asia Pacific region: current status and concerns. Jpn J Clin Oncol. 2012;42(10):867–81.
Lynch T, Connor S, Clark D. Mapping levels of palliative care development: a global update. J Pain Symptom Manage. 2013;45(6):1094–106.
Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Dicker D, et al. The global burden of cancer 2013. JAMA Oncol. 2015;1(4):505–27.
Lee SH, Kim JY, Yeo S, Kim SH, Lim S. Meta-analysis of massage therapy on cancer pain. Integr Cancer Ther. 2015;14(4):297–304.
Atasoy A, Bogdanovic G, Aladashvili A, et al. An international survey of practice patterns and difficulties in cancer pain management in Southeastern Europe: A Turkish & Balkan Oncology Group common initiative. J BUON. 2013;18(4):1082–7.
Van den Beuken-van Everdingen MH, de Rijke JM, Kessels AG. Prevalence of pain in patients with cancer: a systematic review of the past 40 years. Ann Oncol. 2007;18(9):1437–49.
Hearn J, Higginson I. Epidemiology of cancer pain—a systematic review. In: Bruera E, Portenoy RK, editors. Cancer pain: assessment and management. Cambridge: Cambridge University Press; 2003. p 19–37.
Ripamonti C, Zecca E, Brunelli C, et al. Pain experienced by patients hospitalized at the National Cancer Institute of Milan: research project “towards a pain-free hospital”. Tumori. 2000;86(5):412–8.
Melotti RM, Samolsky-Dekel BG, Ricchi E, et al. Pain prevalence and predictors among inpatients in a major Italian teaching hospital. A baseline survey towards a pain free hospital. Eur J Pain. 2005;9(5):485–95.
Namukwaya E, Leng M, Downing J, Katabira E. Cancer pain management in resource-limited settings: a practice review. Pain Res Treat. 2011;2011:393404.
Day M. Pain medicine: a medical specialty? Pain Pract. 2004;4(1):1–6 (discussion 6–10).
Brennan F, Carr DB, Cousins M. Pain management: a fundamental human right. Anesth Analg. 2007;105(1):205–21.
Cousins MJ, Brennan F, Carr DB. Pain relief: a universal human right. Pain. 2004;112(1–2):1–4.
Prommer EE. Pharmacological management of cancer-related pain. Cancer Control. 2015;22(4):412–25.
de Courcy JG. Interventional techniques for cancer pain management. Clin Oncol (R Coll Radiol). 2011;23(6):407–17.
Dohlman LE, Warfield CA. Pain management in developing countries. Am Soc Anesthesiol. 2012;76(6):18–20.
Fullen BM, Baxter GD, O’Donovan BG, Doody C, Daly L, Hurley DA. Doctors’ attitudes and beliefs regarding acute low back pain management: a systematic review. Pain. 2008;136(3):388–96.
Lynch ME, Campbell F, Clark AJ, et al. A systematic review of the effect of waiting for treatment for chronic pain. Pain. 2008;136(1–2):97–116.
Loeser JD. Economic implications of pain management. Acta Anaesthesiol Scand. 1999;43(9):957–9.
World Health Organization. Cancer pain relief and palliative care in children. E-book collection. Geneva: World Health Organization; 1998.
Davis MP, Walsh D. Epidemiology of cancer pain and factors influencing poor pain control. Am J Hosp Palliat Med. 2004;21:137–42.
Mehrvar A, Faranoush M, Hedayati AA, et al. Epidemiological features of childhood acute leukemia at MAHAK’s Pediatric Cancer Treatment and Research Center (MPCTRC), Tehran, Iran. Basic Clin Cancer Res. 2015;7(1):9–15.
Mehrvar A, Faranoush M, Hedayati AA, et al. Epidemiological features of central nervous system tumors at MAHAK Pediatric Cancer Treatment and Research Center. Iran J Blood Cancer. 2011;4(1):19–23.
Alebouyeh M. Current status of pediatric oncology in Iran. Arch Iran Med. 2003;6(3):160–2.
Gharehdaghi FA. Inauguration of the 1st pediatric cancer pain and palliative care unit in the Middle East. J Anesth Crit Care. 2016;4(2):00130.
Acknowledgments
No funding or sponsorship was received for this study or publication of this article. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
F. A. Gharehdaghi, M. Gorginzadeh, and S. Safari declare no conflict of interest.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/59E4F0605AB96738.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Gharehdaghi, F.A., Gorginzadeh, M. & Safari, S. Encountering a Neglected Area of a Healthcare System: A Decade of Improvement in Cancer Pain Clinical Practice in Iran. Pain Ther 5, 135–141 (2016). https://doi.org/10.1007/s40122-016-0055-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40122-016-0055-0