
Abstract
Purpose
The role of regional nodal irradiation (RNI) in patients with clinically positive axillary nodes (cN1) who demonstrate a pathologic complete response (CR) in the axilla following neoadjuvant chemotherapy remains unclear and is currently under study. The present study used the National Cancer Data Base (NCDB) to evaluate patterns of care and characteristics associated with receipt of RNI in this population of patients.
Methods and materials
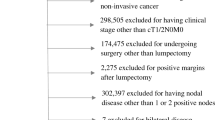
The NCDB was queried for women diagnosed with breast cancer from 2006 to 2012. Patients with nonmetastatic-invasive ductal or lobular carcinoma with clinically positive nodes who underwent neoadjuvant chemotherapy with a pathologic CR in the axilla and known RNI status were included in our analysis.
Results
A total of 4381 patients met inclusion criteria. Within this cohort, 1997 (45.6%) patients received RNI and 2384 (54.4%) did not. On multivariable analysis, factors significantly associated with treatment with RNI included younger age (p = 0.02), shorter distance from hospital (p = 0.01), higher clinical T stage (p < 0.001), presence of lymphovascular space invasion (LVSI) (p = 0.001), greater number of examined nodes (p < 0.001), and use of adjuvant systemic therapy (p < 0.001). RNI was used in 51.8% of patients ages 18–29, 47.6% for ages 30–49, 45.0% for ages 50–69, and 29.9% for ages >69 years. Among patients who received adjuvant systemic therapy, RNI was used in 51.0% of cases, compared with 43.0% for those not receiving adjuvant systemic therapy.
Conclusions
In this large cancer database study, we observed substantial variation in the use of RNI in clinically node-positive patients with pathologic CR following neoadjuvant chemotherapy based on patient-, tumor-, and treatment-related factors.



Similar content being viewed by others


References
Whelan TJ, Olivotto IA, Parulekar WR et al (2015) Regional nodal irradiation in early-stage breast cancer. N Engl J Med 373:307–316
Poortmans PS, Collette S, Kirkove C et al (2015) Internal mammary and medial supraclavicular irradiation in breast cancer. N Engl J Med 373:317–327
Nielsen HM, Overgaard M, Grau C et al (2006) Study of failure pattern among high-risk breast cancer patients with or without postmastectomy radiotherapy in addition to adjuvant systemic therapy: long-term results from the Danish breast cancer cooperative group DBCG 82b and c randomized studies. J Clin Oncol 24:2268–2275
Ragaz J, Olivotto IA, Spinelli JJ et al (2005) Locoregional radiation therapy in patients with high-risk breast cancer receiving adjuvant chemotherapy: 20-year results of the British Columbia randomized trial. J Natl Cancer Inst 97:116–126
Mougalian SS, Soulos PR, Killelea BK et al (2015) Use of neoadjuvant chemotherapy for patients with stage I to II breast cancer in the United States. Cancer 121:2544–2552
Buchholz TA, Lehman CD, Harris JR et al (2008) Statement of the science concerning locoregional treatments after preoperative chemotherapy for breast cancer: a National Cancer Institute conference. J Clin Oncol 26:791–797
Rastogi P, Anderson SJ, Bear HD et al (2008) Preoperative chemotherapy: updates of the National Surgical Adjuvant Breast and bowel project protocols B-18 and B-27. J Clin Oncol 26:778–785
National Comprehensive Cancer Network. Breast Cancer: Version 1 2016. Available at: http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf. Accessed March 11, 2016.
McGuire SE, Gonzalez-Angula AM, Huang EH et al (2007) Postmastectomy radiation improves the outcome of patients with locally advanced breast cancer who achieve a pathologic complete response to neoadjuvant chemotherapy. Int J Radiat Oncol Biol Phys 68:1004–1009
Huang EH, Tucker SL, Strom EA et al (2005) Predictors of locoregional recurrence in patients with locally advanced breast cancer treated with neoadjuvant chemotherapy, mastectomy, and radiotherapy. Int J Radiat Oncol Biol Phys 62:351–357
Huang EH, Tucker SL, Strom EA et al (2004) Postmastectomy radiation improves local-regional control and survival for selected patients with locally advanced breast cancer treated with neoadjuvant chemotherapy and mastectomy. J Clin Oncol 22:4691–4699
Mamounas EP, Anderson SJ, Dignam JJ et al (2012) Predictors of locoregional recurrence after neoadjuvant chemotherapy results from combined analysis of National Surgical Adjuvant Breast and bowel project B-18 and B-27. J Clin Oncol 30:3960–3966
Marks LB, Prosnitz LR (2014) Reducing local therapy in patients responding to preoperative systemic therapy: are we outsmarting ourselves? J Clin Oncol 32:491–493
National Surgical Adjuvant Breast and Bowel Project Protocol B51/Radiation Therapy Oncology Group 1304. Available at www.ctsu.org. Accessed March 11, 2016.
Burstein HJ, Morrow M (2015) Nodal irradiation after breast-cancer surgery in the era of effective adjuvant therapy. N Engl J Med 373:379–381
American College of Surgeons. National Cancer Data Base. Available at: www.facs.org/quality-programs/cancer/ncdb. Accessed March 11, 2016
Recht A, Edge SB, Solin LJ et al (2001) Postmastectomy radiotherapy: clinical practice guidelines of the American Society of Clinical Oncology. J Clin Oncol 19:1539–1569
Lin CC, Bruinooge SS, Kirkwood MK et al (2016) Association between geographic access to cancer care and receipt of radiation therapy for rectal cancer. Int J Radiat Onc Biol Phys 94:719–728
Rusthoven CG, Rabinovitch RA, Jones BL, et al. (2016) The impact of postmastectomy and regional nodal radiation after neoadjuvant chemotherapy for clinically lymph node positive breast cancer: a National Cancer Database (NCDB) analysis. Ann Oncol
Darby SC, Ewertz M, McGale P et al (2013) Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med 368:987–998
Henson KE, Jagsi R, Cutter D et al (2016) Inferring the effects of cancer treatment: divergent results from early breast cancer trialists’ collaborative group meta-analyses of randomized trials and observational data from SEER registries. J Clin Oncol 34:803–809
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding source
No funding support is associated with this study.
Conflict of interest
Dr. Grover declares that she has no conflict of interest. Dr. Badiyan declares that he has no conflict of interest. Dr. Trifiletti declares that he has no conflict of interest. Dr. Showalter declares that she has no conflict of interest. Dr. Pham declares that she has no conflict of interest. Dr. Vicini declares that he has no conflict of interest. Dr. Juloori declares that he has no conflict of interest. Dr. Freedman declares that he has no conflict of interest. Dr. Tendulkar declares that he has no conflict of interest. Dr. Swisher-McClure declares that he has no conflict of interest. Dr. Nichols declares that she has no conflict of interest. Dr. Feigenberg declares that he has no conflict of interest. Dr. Shah declares that he is a consultant for Impedimed.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Grover, S., Badiyan, S.N., Trifiletti, D.M. et al. Regional nodal irradiation following pathologic complete response in the axilla to neoadjuvant chemotherapy: patterns of treatment. J Radiat Oncol 6, 81–92 (2017). https://doi.org/10.1007/s13566-016-0290-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13566-016-0290-3