
Abstract
Introduction
Atopic dermatitis (AD) is related to other atopic diseases asthma and allergic rhinitis. It is known that those with asthma or allergic rhinitis have impaired immune responses that may predispose them to infections. This study sought to determine whether adult AD is associated with systemic infections, and whether association is strengthened in those with AD plus another atopic disease.
Methods
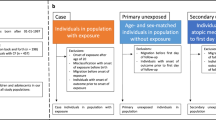
This cross-sectional study obtained information from adults in the 2010 and the 2012 National Health Interview Survey (NHIS). The primary exposure was history of AD without or with an additional atopic disease, asthma or allergic rhinitis. Self-reported systemic infections were the primary outcomes. Survey logistic regression was performed and adjusted odds ratios (aOR) reported.
Results
AD in NHIS 2010 was associated with increased risk of sinusitis [aOR (95% CIs): 1.65 (1.42, 1.91), P < 0.001], head or chest cold [1.31 (1.12, 1.52), P < 0.001], and gastrointestinal illness [2.39 (1.97, 2.89), P < 0.001], and in NHIS 2012, pneumonia/influenza [1.73 (1.54, 1.95), P < 0.001], strep throat/tonsillitis [1.72 (1.54, 1.92), P < 0.001], sinusitis [1.77 (1.54, 2.02), P < 0.001], head or chest cold [1.49 (1.33, 1.67), P < 0.001], and infectious disease [2.66 (2.20, 3.21), P < 0.001]. An increase in atopic disease mirrored an increase in number of infectious outcomes and was statistically significant in the combined dataset (P < 0.001).
Conclusion
The associations between AD and AD plus another atopic disease with systemic infections suggest that an underlying immune defect may be contributing to microbial susceptibility. Further studies are warranted to understand the burden of infectious disease in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Atopic dermatitis (AD), also known as eczema, is a chronic inflammatory skin disease characterized by pruritic, scaly, and crusted lesions, typically on flexor surfaces. Symptoms usually develop in childhood and follow a chronic relapsing course over a person’s lifetime [1]. A significant proportion of the United States population is affected by AD, with a prevalence ranging from 8.7% to 18.1% in children [2]. While it was previously thought that AD resolves as one reaches adulthood, a recent US population estimate of 10% in adults [3] suggests that the prevalence may be higher than expected [4]. AD is associated with significant comorbidities, including high blood pressure [5], mental health disorders [6], and sleep disturbance [7]. The incidence of AD is actually increasing in industrialized countries, representing a major healthcare cost [8].
A multitude of factors are implicated in the pathogenesis of AD, including a skin barrier defect due to filaggrin mutations, environmental sensitization, decreased production of antimicrobial peptides [9], and alterations in the balance of the skin microbiome [1]. It is well-established that patients with AD have increased susceptibility to skin infections, including Staphylococcus aureus, molluscum contagiosum, and herpes simplex [10, 11]. This predisposition to pathogenic colonization has been linked to a defective skin barrier, but it is being recognized that defective innate and cell-mediated immunity may also be a significant factor.
Studies have demonstrated aberrant T-helper-2 (Th2) lymphocyte predominance over T-helper-1 (Th1) lymphocyte immune responses in patients with AD. Th2 lymphocytes secrete factors that downregulate anti-inflammatory cytokines, inhibit Toll-like 2 receptor-mediated signal transduction, and ultimately inhibit the ability to mount an immune response against bacteria and viruses [12, 13]. Similar immune system skewing is seen in other atopic diseases such as asthma and allergic rhinitis [14]. The triad of asthma, allergic rhinitis, and atopic dermatitis share common genetic and pathophysiologic characteristics, and 50% of AD patients develop one of these other atopic disorders [8, 15]. Many studies have found an increased risk for infections, particularly respiratory, in those with asthma [14]. These explorations even led to the implementation of national ACIP guidelines to give a single dose of the pneumococcal vaccine to adult patients with asthma [16].
Although the underlying immune defect is similar in asthma and AD, only a few studies have investigated infectious complications in AD on a systemic level. Many of the studies were in the pediatric population [17–21], while the same risk in adult AD patients has not been thoroughly examined [14, 22, 23]. This study seeks to determine whether adult AD alone or AD with comorbid atopic disease is associated with higher odds of systemic infections compared to the general adult population in two large population-based observational surveys.
Methods
National Health Interview Survey
This population-based cross-sectional study extracted pre-existing, publically available data from participants of the 2010 and 2012 National Health Interview Survey (NHIS), a database collected by the National Center for Health Statistics. The NHIS annually samples households based on the Bureau of the Census to provide an accurate representation of the civilian non-institutionalized population. One adult 18 years of age or older from each household was randomly selected to complete the questionnaire. Trained United States Census Bureau interviewers conducted NHIS interviews, which consisted of in-person household interviews, as well as telephone follow-up or computer-assisted personal interviewing. The population was weighted based on age, sex, and race/ethnicity using United States Bureau of the Census data. All numeric population counts represent raw values, and prevalence estimates and statistical analyses include population weights. This study was approved by the Institutional Review Board at the University of California, San Diego. This article does not contain any new studies with human or animal subjects performed by any of the authors. The NHIS questions corresponding to the study variables of interest are shown in Table S1.
Statistical Analysis
Statistical analyses were performed using R Statistical Software v.3.2.2. Complete data analysis was performed, meaning those with missing values were excluded. All analyses were performed using the survey design package to assign population weights. The primary aim was to determine the risk of infections in participants with AD versus those without AD. The secondary aim was to analyze the subset of individuals with AD to determine the risk of systemic infections in those with AD alone versus those with AD plus another atopic disease. Survey logistic regression was performed with those with a 1-year history of AD and AD plus other atopic disease as the independent variables, and the following binary outcomes as the dependent variables: history of pneumonia/influenza, history of strep throat/tonsillitis, 1-year history of sinusitis, 1-year history of head/chest cold, 2-week history of gastrointestinal (GI) illness, and 1-year history of overall infectious disease. One-year history of overall infectious disease was a separate variable in the questionnaire (Table S1). Multivariable survey logistic regression was performed using backwards model selection for the following potential confounders or independent predictors: age, gender, race/ethnicity, Hispanic origin, smoking status, body mass index (BMI), history of asthma, 1-year history of allergic rhinitis, diabetes, hypertension, chronic obstructive pulmonary disease (COPD), and history of malignancy. Two-way interactions between AD, asthma, and allergic rhinitis were also tested for significance and included in the multivariable analysis if the P value <0.05. Unadjusted odds ratios (OR) and adjusted odds ratios (aORs) with 95% confidence intervals were calculated using the multivariable logistic regression models. Two-sided P values less than 0.05 were considered statistically significant.
For NHIS 2010, a response of “don’t know” or refusal to answer the question was seen in the following cases: 18 for AD (0.07%), 20 for asthma (0.07%), 22 for allergic rhinitis (0.08%), 16 for head/chest cold (0.06%), 23 for sinusitis (0.09%), 13 for GI illness (0.04%), 185 for smoking status (0.68%), 16 for diabetes (0.06%), 46 for hypertension (0.17%), 28 for COPD (0.10%), and 20 for malignancy (0.08%). For NHIS 2012, a response of “don’t know” or refusal to answer the question was seen in the following cases: 25 for AD (0.07%), 20 for asthma (0.05%), 25 for allergic rhinitis (0.07%), 46 for head/chest cold (0.13%), 33 for infectious diseases (0.12%), 29 for sinusitis (0.09%), 43 for pneumonia/influenza (0.13%), 86 for strep throat/tonsillitis (0.25%), 258 for smoking status (0.75%), 25 for diabetes (0.07%), 12 for hypertension (0.09%), 34 for COPD (0.10%), and 20 for malignancy (0.06%).
Results
Population Demographics
This study analyzed data from 26,815 adults in NHIS 2010 and 33,918 adults in NHIS 2012, representing all ages, genders, and races. The 1-year prevalence of atopic dermatitis was 10.1% (9.7–10.6%) in the NHIS 2010 population and 7.2% (6.8–7.6%) in the NHIS 2012 population. The prevalence of asthma was 12.6% (12.1–13.2%) and 12.6% (12.1–13.1%) and allergic rhinitis was 7.8% (7.4–8.2%) and 7.5% (7.1–7.8%) in NHIS 2010 and NHIS 2012, respectively.
In both datasets, individuals with AD had higher prevalence of many comorbid medical conditions, including hypertension (2010: 36.0% vs. 29.6%, P < 0.001; 2012: 36.5% vs. 29.1%, P < 0.001), COPD (2010: 3.1% vs. 1.7%, P < 0.001; 2012: 6.2% vs. 2.6%, P < 0.001), and history of malignancy (2010: 13.9% vs. 7.8%, P < 0.001; 2012: 11.5% vs. 8.2%, P < 0.001). Additionally, individuals with AD had a greater prevalence of asthma (2010: 25.0% vs. 11.6%, P < 0.001; 2012: 25.0% vs. 11.6%, P < 0.001) and allergic rhinitis (2010: 15.7% vs. 6.9%, P < 0.001; 2012: 14.0% vs. 7.0%, P < 0.001) (Tables S2, S3).
Prevalence of Infectious Outcomes
In NHIS 2010, the prevalence of 1-year history of sinusitis was 13.0% (12.4–13.5%), 2-week history of head or chest cold was 11.1% (10.7–11.7%), and 2-week history GI illness was 5.0% (4.7–5.3%). In NHIS 2012, the prevalence of pneumonia/influenza was 23.7% (22.9–24.6%), strep throat/tonsillitis was 33.8% (33.0–34.7%), 1-year history of sinusitis was 12.1% (11.6–12.6%), 1-year history of head or chest cold was 42.9% (42.1–43.7%), and 1-year history of any infectious disease was 3.1% (2.9–3.4%).
Association Between AD and Systemic Infections
In NHIS 2010, history of AD in the past year was associated with significantly higher odds of all infectious outcomes in univariate models. This association remained significant in multivariate survey logistic regression models that adjusted for age, sex, race, Hispanic origin, BMI, diabetes, hypertension, COPD, and history of malignancy. AD was associated with higher odds of sinusitis [aOR (95% CIs): 1.65 (1.42, 1.91), P < 0.001], head or chest cold [1.31 (1.12, 1.52), P < 0.001], and GI illness [2.39 (1.97, 2.89), P < 0.001] (Table 1).
Similarly, AD for the past year in the NHIS 2012 dataset was associated with higher odds of all infectious outcomes in multivariate models. AD was associated with higher odds of sinusitis [1.77 (1.54, 2.02), P < 0.001], head or chest cold [1.49 (1.33, 1.67), P < 0.001], pneumonia/influenza [aOR (95% CIs): 1.73 (1.54, 1.95), P < 0.001], strep throat/tonsillitis [1.72 (1.54, 1.92), P < 0.001], and infectious disease [2.66 (2.20, 3.21), P < 0.001] (Table 2).
Association Between AD Subgroups and Systemic Infections
Participants with a 1-year history of AD were stratified into three categories of atopic disease severity: (1) no other atopic disease, (2) at least one other atopic disease, defined as current diagnosis of asthma or allergic rhinitis, and (3) both asthma and allergic rhinitis. In both datasets, there was parallel increase in odds of infectious disease with increasing atopic disease (Tables 3, 4). All adjusted odds ratios in those with additional atopic disease were significantly higher than AD alone, except for GI illness in NHIS 2010 [one atopic disease: 1.33 (0.97, 1.84), P = 0.08; two atopic diseases: 1.30 (0.72, 2.35), P = 0.39] (Table 3) and strep throat/tonsillitis in NHIS 2012 [one atopic disease: 1.09 (0.84, 1.41), P = 0.51] (Table 4).
Association Between Atopic Disease and Multiple Infections
The NHIS 2010 and 2012 datasets were combined, and the cumulative number of infectious outcomes was calculated for participants in the following subgroups of atopic disease: (1) no atopic disease, (2) AD alone, (3) AD plus one other atopic disease (asthma or allergic rhinitis), (4) all three atopic diseases. Using a multivariate generalized linear model controlling for the same confounders as in the previous analysis, the means and 95% CI for each group were generated: (1) 0.62 (0.62, 0.63), (2) 0.85 (0.82, 0.87), (3) 1.25 (1.21, 1.30), (4) 1.68 (1.59, 1.77). An increase in atopic disease mirrored an increase in number of infectious outcomes and was statistically significant in the combined dataset (Fig. 1; P < 0.001).

Association between atopic disease and number of infections in NHIS 2010 and 2012. The number of infectious outcomes was calculated for 1 no atopic disease, 2 AD alone, 3 AD plus one other atopic disease, and 4 all three atopic diseases. The increased number of infections was significant in a multivariable linear regression model (P < 0.001)
Discussion
In this population-based study, atopic dermatitis was associated with increased odds of systemic infections including pneumonia/influenza, strep throat/tonsillitis, sinusitis, overall infectious disease, head or chest cold, and GI illness. This risk remained significant after adjusting for other atopic diseases, asthma and allergic rhinitis, and controlling for comorbidities commonly associated with risk of infection. Stratification of AD into participants with one or two atopic diseases revealed an increased risk of all infections with increased atopic comorbidity. As the number of comorbid atopic diseases increased, participants reported a parallel increase in cumulative number of infections.
It is well-established that patients with AD are susceptible to skin infections by several microorganisms, but significance beyond the skin is not as well understood. Increased risk of systemic infections has been demonstrated in pediatric patients with atopic dermatitis [17–21]. In adults, one small-scale study did find an increased risk of serious invasive pneumococcal disease in adults with AD [22]. Other small studies examining outcomes of strep pharyngitis and pneumonia failed to ascertain a significant difference, perhaps due to limited sample size [23]. Our results are consistent with a recent publication examining the risk of infections in adult AD [24]. However, we have expanded on this study by including one more year of data and controlling for several important comorbidities that also increase infection risk, decreasing the possibility of confounding. Additionally, we have examined the relationship between comorbid atopic disease and infection.
The association between AD and systemic infections suggests that the immunological defects contributing to skin disease may also be contributing on a deeper level. Extensive study of the immunologic basis of AD consistently identifies an expansion of Th2, Th17, and Th22 cells and concomitant decreased Th1 cell frequency in AD versus control skin [25–27]. The expression of Th2/Th22 cytokines such as Interleukin (IL)-4, IL-13, IL-25, and IL-33 can directly impair expression of barrier proteins [28] and also increase serine protease activity [29, 30], both of which contribute to a defective skin barrier. These cytokines inhibit antimicrobial peptide production and impair innate immune cell activation at the epidermis [4]. In addition, the relative deficiency of interferon gamma producing T cells can inhibit viral immunity [31]. These consequences of Th2 lymphocyte skewing help explain the increased susceptibility to skin infections. However, how these immune mechanisms function at other epithelial sites is largely unknown. Increased circulating levels or induction of these cytokines at other epithelial surfaces in the body can theoretically induce similar suppression of barrier proteins and antimicrobial defense.
Additionally, behavioral changes related to atopic disease may contribute to this phenomenon. Epidemiology studies have shown that severe atopic disease, including AD, is associated with reduced physical activity and sports participation in children [32]. Some may also avoid outdoor activities due to irritation from airborne allergens and sun exposure, resulting in low vitamin D levels. Given that exercise and adequate vitamin D levels are powerful stimuli of immune function, these behavioral changes may partially explain the risk of infections in atopic patients [33–36].
Our findings demonstrate that multiple comorbid atopic diseases directly correlate with increased infections. While this is purely an observational study, this suggests that increased atopic sensitization may lead to greater immune dysregulation. Further epidemiologic in vitro and in vivo studies investigating the differences between subgroups of atopic patients may help to understand the pathophysiology. If indeed there is a significant difference, those with multiple atopic conditions may benefit from stricter monitoring for infectious disease.
This study has several strengths, including the use of two large, randomly sampled US population surveys. The survey respondents represent diverse geographic and demographic variables, making them generalizable to the entire population. In addition, there was a sufficiently large population to control for a large number of potential confounders in logistic regression analyses. The use of a survey dataset also has limitations. Ascertainment of exposure and outcome variables was based on self-report of disease status and was not verified by clinical or laboratory measures. However, the self-report questions used to determine AD in this survey have been validated as adequately sensitive and specific for epidemiologic research [37]. Selection bias is also possible given that those with AD may be more likely to remember and report illness.
Conclusions
In conclusion, adult atopic dermatitis is associated with increased risk of pneumonia/influenza, sinusitis, strep pharyngitis, head or chest cold, gastrointestinal illness, and infectious disease overall. Atopic dermatitis plus increasing atopic comorbidity confers significantly increased risk for these systemic infections compared to atopic dermatitis alone. Little is known about the morbidity and mortality of this increased susceptibility in this population. Further studies are warranted to characterize the burden of infectious disease in atopic dermatitis.
References
Miyagaki T, Sugaya M. Recent advances in atopic dermatitis and psoriasis: Genetic background, barrier function, and therapeutic targets. J Dermatol. 2015;78(2):89–94.
Silverberg N. A practical overview of pediatric atopic dermatitis, part 1: epidemiology and pathogenesis. Cutis. 2016;97(4):267–71.
Silverberg JI, Hanifin JM, York N. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. J Allergy Clin Immunol. 2013;132(5):1132–8.
Weidinger S, Novak N. Atopic dermatitis. Lancet. 2015;387(10023):1109–22.
Silverberg JI, Greenland P. Eczema and cardiovascular risk factors in 2 US adult population studies. J Allergy Clin Immunol. 2015;135(3):721–8.
Yu SH, Silverberg JI. Association between atopic dermatitis and depression in US adults. J Invest Dermatol. 2015;135(12):3183–6.
Silverberg JI, Garg NK, Paller AS, Fishbein AB, Zee PC. Sleep disturbances in adults with eczema are associated with impaired overall health: a US population-based study. J Invest Dermatol. 2015;135(1):56–66.
Galli E, Gianni S, Auricchio G, Brunetti E, Mancino GRP. Atopic dermatitis and asthma. Allergy Asthma Proc. 2007;28(5):540–3.
Ong PY, Ohtake T, Brandt C, et al. Endogenous antimicrobial peptides and skin infections in atopic dermatitis. N Eng J Med. 2002;347(15):1151–60.
Kong HH, Oh J, Deming C, et al. Temporal shifts in the skin microbiome associated with disease flares and treatment in children with atopic dermatitis. Genome Res. 2012;22(5):850–9.
Wollenberg A, Wetzel S, Burgdorf WC, Haas J. Current perspectives: viral infections in atopic dermatitis: pathogenic aspects and clinical management. J Allergy Clin Immunol. 2003;112(4):667–74.
Brandt E, Sivaprasad U. Th2 cytokines and atopic dermatitis. J Clin Cell Immunol. 2011;2(3):110.
Arkwright PD, Patel L, Moran A, Haeney MR, Ewing CL, David TJ. Atopic eczema is associated with delayed maturation of the antibody response to Pneumococcal vaccine. Clin Exp Immunol. 2000;122(1):16–9.
Juhn YJ. Risks for infection in patients with asthma (or other atopic conditions): is asthma more than a chronic airway disease? J Allergy Clin Immunol. 2014;134(2):247–57.
Kapoor R, Chandrakala M, Hoffstad O, Bilker W, Leclerc P, Margolis DJ. The prevalence of atopic triad in children with physician-confirmed atopic dermatitis. J Am Acad Dermatol. 2008;58(1):68–73.
The Center for Disease Control and Prevention. Updated recommendations for prevention of invasive pneumococcal disease among adults using the 23-valent pneumococcal polysaccharide vaccine (PPSV23). Morb Mortal Wkly Rep. 2010;59:1102–6.
Silverberg JI, Silverberg NB. Childhood atopic dermatitis and warts are associated with increased risk of infection: a US population-based study. J Allergy Clin Immunol. 2014;133(4):1041–7.
Bjur K, Lynch R, Fenta Y, et al. Assessment of the association between atopic conditions and tympanostomy tube placement in children. Allergy Asthma Proc. 2012;33(3):289–96.
Santos JCH, Zhang L, Menegatti PK, et al. Pneumonia in the first 2 years of life and asthma in preschool-age children. Pediatr Int. 2011;53:576–80.
Boikos C, Quach C. Risk of invasive pneumococcal disease in children and adults with asthma: a systematic review. Vaccine. 2013;31(42):4820–6.
Lynch MD, Sears A, Cookson H, et al. Disseminated coxsackievirus A6 affecting children with atopic dermatitis. Clin Exp Dermatol. 2015;40(5):525–8.
Jung J, Kita H, Yawn BP, et al. Increased risk of serious pneumococcal disease in patients with atopic conditions other than asthma. J Allergy Clin Immunol. 2010;125(1):217–21.
Juhn YJ, Frey D, Li X, Jacobson R. Streptococcus pyogenes upper respiratory infection and atopic conditions other than asthma: a retrospective cohort study. Prim Care Respir J. 2012;21(2):153–8.
Strom M, Silverberg JI. Association between atopic dermatitis and extracutaneous infections in US adults. Br J Dermatol. 2016. doi:10.1111/bjd.14708
Kuo I, Yoshida T, De Benedetto A, Beck LA. The cutaneous innate immune response in patients with atopic dermatitis. J Allergy Clin Immunol. 2013;131(2):266–78.
Gittler J, Shermer A, Suárez-Fariñas M, et al. Progressive activation of Th2/Th22 cytokines and selective epidermal proteins characterizes acute and chronic atopic dermatitis. J Allergy Clin Immunol. 2012;130(6):1344–54.
De Benedetto A, Agnihothri R, Mcgirt LY, Bankova LG, Beck LA. Atopic dermatitis: a disease caused by innate immune defects? J Invest Derm. 2009;129(1):14–30.
Seltman J, Roesner LM, von Hesler FW, Wittmann M, Werfel T. IL-33 impacts on the skin barrier by downregulating the expression of filaggrin. J Allergy Clin Immunol. 2015;135(6):1659–61.
Morizane S, Yamasaki K, Kajita A, et al. Th2 cytokines increase kallikrein 7 expression and function in atopic dermatitis. J Allergy Clin Immunol. 2012;130(1):259–61.
Di ZH, Ma L, Qi RQ, et al. T helper 1 and T helper 2 cytokines differentially modulate expression of filaggrin and its processing proteases in human keratinocytes. Chin Med J (Engl). 2016;129(3):295–303.
Brar K, Leung DYM. Recent considerations in the use of recombinant interferon gamma for biological therapy of atopic dermatitis. Expert Opin Biol Ther. 2016;16(4):507–14.
Strom MA, Silverberg JI. Associations of physical activity and sedentary behavior with atopic disease in United States children. J Pediatr. 2016;174:247.e3–253.e3.
Yameogo CW, Cichon B, Fabiansen C, et al. Correlates of physical activity among young children with moderate acute malnutrition. J Pediatr. 2016;(16):S0022–S3476.
Gleeson M, Bishop NC, Stensel DJ, Lindley MR, Mastana SS, Nimmo MA. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat Rev Immunol. 2011;11:607–15.
Kroner JC, Sommer A, Fabri M. Vitamin D every day to keep the infection away? Nutrients. 2015;7(6):4170–88.
Hart PH, Gorman S, Finlay-Jones JJ. Modulation of the immune system by UV radiation: more than just the effects of vitamin D? Nat Rev Immunol. 2011;11(9):584–96.
Silverberg JI, Patel N, Immaneni S, et al. Assessment of atopic dermatitis using self-report and caregiver report: a multicentre validation study. Br J Dermatol. 2015;173(6):1400–4.
Acknowledgements
No funding or sponsorship was received for this study or publication of this article. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published. This work was presented at the American Academy of Dermatology Summer Meeting in July 2016.
Disclosures
Saisindhu Narala and Tissa R. Hata declare no conflicts of interest.
Compliance with Ethics Guidelines
This study was approved by the Institutional Review Board at the University of California, San Diego. This article does not contain any new studies with human or animal subjects performed by any of the authors.
Data Availability
The datasets generated during and/or analyzed during the current study are available in the National Health Interview Survey repository, https://www.cdc.gov/nchs/nhis/data-questionnaires-documentation.htm.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/C387F0603683BDAA.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Narala, S., Hata, T.R. Adult Atopic Dermatitis with Comorbid Atopic Disease is Associated with Increased Risk of Infections: A Population-Based Cross-Sectional Study. Dermatol Ther (Heidelb) 7, 111–121 (2017). https://doi.org/10.1007/s13555-017-0172-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-017-0172-7