
Abstract
Background
A novel avian influenza A(H7N9) virus, first identified in Mainland China in February and March 2013, caused an outbreak in humans in April and May, 2013. Closure of live poultry markets in some affected cities dramatically reduced numbers of cases during summer of 2013, but the epidemic resurged during the winter 2013–14, increasing reported cases to 393 in Mainland China as of 30 March 2014.
Purpose
The study aimed to explore population behavior patterns responding to an epidemic of influenza A(H7N9) virus.
Method
Three cross-sectional surveys were conducted among 1000, 680, and 1011 respondents in December 2013, January 2014, and February 2014, with response rates of 68.0, 64.4, and 66.6 %, respectively, in Hong Kong. Adults were recruited and interviewed using random digit-dialing telephone survey. Latent class analysis was employed to explore heterogeneity in protective behavior patterns across the three surveys. Multinomial regression models were developed to determine factors associated with latent class membership.
Results
Three comparable latent classes were identified across the three surveys: Moderate hygiene compliance (Class 1), High hygiene compliance (Class 2), and Vigilance (Class 3). The prevalence of Class 1 was 48–52 % across the three surveys while Class 3 prevalence increased significantly from 13 % in the Dec-2013 survey to 20 % in the Feb-2014 survey. Compared with Class 1, Class 3 were more likely to be female, older, better educated, married, perceive higher susceptibility to H7N9, attribute greater severity to H7N9, report higher current worry, and anticipated worry about H7N9 infection.
Conclusion
The three classes reflect different levels of adoption of protection and thereby may have different levels of vulnerability toward contracting H7N9 infection. It appears that as the epidemic intensifies, Class 2 (Good hygiene compliance) members are likely to transfer to Class 3 (Vigilance) while Class 1 (Moderate hygiene compliance) could be unchanged. The young, mostly single males and those with lower educational achievement represent a group for whom public health messages need to be targeted.
Similar content being viewed by others

Introduction
A novel avian influenza A(H7N9) virus, first identified in Mainland China in February and March 2013 [1], caused an outbreak in humans in April and May, 2013 [2, 3]. Closure of live poultry markets in some affected cities dramatically reduced numbers of cases during summer of 2013 [4], but the epidemic resurged during the winter 2013–14, increasing reported cases to 393 in Mainland China as of 30 March 2014 [5]. The winter 2013–14 outbreak was mainly focused in Zhejiang Province in eastern China near Shanghai and Guangdong province in southern China adjacent to Hong Kong [6]. Guangdong’s proximity sees considerable daily cross-border movement of people and poultry into Hong Kong. Ten confirmed human cases of H7N9 infection have been reported in Hong Kong since the winter 2013–2014 outbreak, each of which had a recent history of exposure to live poultry in Guangdong [7].
Although a local epidemic has yet to occur in Hong Kong, the behavioral responses among the public in the early stages of an infectious disease epidemic are important for determining the patterns of population contacts. Population behavior can significantly modify the basic reproductive number, R 0, and thereby the daily number of newly emerging cases, influencing the epidemic’s trajectory and final size [8–10]. A few studies have tried to measure the patterns of social contacts to provide some empirical parameters for mathematical models to assess the dynamics of transmission during epidemics [9, 10]. These studies mainly focused on patterns of daily individual contacts, and they treated behavior in the population as homogenous, without considering the potential heterogeneity in population behavior in response to infectious disease outbreaks [9, 10]. Latent class analysis (LCA), a statistical approach that captures population heterogeneity and classifies the observed population into a certain number of groups who answer a set of categorical variables in similar ways [11], has been widely used to analyze patterns of behaviors in relation to non-communicable diseases such as alcohol drinking [12, 13]. However, we are not aware of previous studies that attempted to classify population behavioral patterns in response to a new infectious disease. To address this knowledge gap, the first objective of this study was to explore population behavior patterns in response to newly emerging infection diseases, using H7N9 infection as an example. We also examined whether patterns of behavioral responses would change as the H7N9 epidemic grew in Mainland China and more imported H7N9 human cases were reported in Hong Kong.
Accounting for variation in adoption of personal protective behaviors is an important task that has so far not been well addressed. Population behaviors toward a threat are inherently heterogeneous because of individual variation in perceived personal risk to any given threat which serves to motivate responses to the threat [14]. Prevailing cognitive behavioral models [15, 16] propose that higher perceived personal susceptibility to disease and higher perceived threat severity motivates greater adoption of protective behaviors. A recent literature review [14] showed that most empirical studies have consistently reported a positive association between perceived personal risk (including perceived personal susceptibility to and perceived severity of the disease, and worry about the infection) and adoption of both hygiene practices and avoidance behaviors during the 2003 outbreak of severe acute respiratory syndrome and the 2009 influenza A/H1N1 pandemic.
People with different demographics are likely to vary in their perceived personal risk to a common threat. Older people are more likely to view themselves as more susceptible to a disease [17], and thereby they were more likely to adopt hygiene practices [18–20] and avoid public places during epidemics [21, 22]. Reports suggest that females perceive themselves to be more vulnerable to a threat and to worry more about diseases [23]. Women report better hygiene and more avoidance behaviors during epidemics [18, 19, 24]. The association between educational attainment and adoption of protective behaviors is less conclusive in the literature [14]. Better educated individuals may be more aware of the risk related to the threat but may also have more confidence to control the threat [25], and so might be expected to be more variable in their responses to a new infectious disease. Therefore, the second objective of this study involved examining how patterns of behavioral responses among the public differed by their demographics and risk perception relating to H7N9 infection.
Methods
Timing of the Population Surveys
Three independent cross-sectional surveys were conducted among the Hong Kong general public in 4–8 December 2013 (Dec-2013 survey), 23–28 January 2014 (Jan-2014 survey), and 12–17 February 2014 (Feb-2014 survey), respectively. The Dec-2013 survey was conducted after two imported cases were reported in Hong Kong and before the winter 2013–2014 outbreak had started, while the Jan-2014 and Feb-2014 surveys were conducted during the peak of the winter 2013–2014 outbreak. The Feb-2014 survey was also conducted after H7N9 virus was first identified from samples of live chickens imported from Mainland China and the government closed all live poultry markets in Hong Kong accordingly [26]. Three more imported cases were confirmed in Hong Kong between the Jan-2014 and the Feb-2014 surveys.
Participants
Penetration of landlines among Hong Kong households was around 100 % [27]. Over 90 % of the Hong Kong population were Chinese ethnicity and able to communicate using Cantonese or Mandarin. All three surveys recruited subjects who were of Chinese ethnicity, aged 18 years or above, and able to speak Cantonese or Mandarin. To recruit subjects, households were first selected using random-digit dialed telephone numbers. Then within each household, one eligible subject was randomly selected using Kish grid methods and invited to complete a telephone interview based on a standardized questionnaire. This has been demonstrated to be a valid method to recruit a sample representative of the population in Hong Kong in previous studies [19, 28]. All calls were made by an experienced polling institution that had demonstrated good performance in similar population surveys [28]. All interviews were conducted during non-working hours to avoid over-sampling of unemployed subjects. Up to four additional calls were made for unanswered numbers or if the selected subjects were not available. All respondents gave verbal consent before participating in the study. The study obtained ethics approval from the Institutional Review Board of The University of Hong Kong/Hospital Authority Hong Kong West Cluster.
A total of 1000, 680, and 1011 respondents completed the Dec-2013, Jan-2014, and Feb-2014 surveys, with response rates of 68.0, 64.4, and 66.6 %, respectively.
Study Measures
The questionnaires used for the three surveys were similar to those used in our previous surveys related to severe acute respiratory syndrome (SARS) [19], A/H5N1 in 2004 and 2005 [29, 30], and the 2009 influenza A/H1N1 pandemic [28]. Each questionnaire required on average 15 min to complete by telephone interview. This paper focuses on respondents’ adoption of protective measures and their associations with perception of H7N9 risk and demographics. All the following measures were assessed using identical items for the three surveys.
Adoption of Protective Measures
A total of 14 items were used to measure respondents’ adoption of protective measures including hygiene practices, avoidance behaviors, and wearing face masks. Specifically, respondents were asked how frequent they had adopted the following seven practices 3 days prior to the survey: washing hands after sneezing or coughing, washing hands after returning home, using liquid soap when washing hands, using serving utensils when dining with others, avoiding touching common objects such as door knobs and lift buttons, washing hands after touching common objects, and wearing face masks. Responses for all these items were dichotomized as “1 = always/usually” and “0 = sometimes/never” except for of the item “wearing face masks” which was dichotomized as “1 = always/usually/sometimes” and “0 = never” because it is unlikely that most respondents will routinely wear face masks in their daily life. Respondents were also asked whether they had adopted any of the following practices in the 7 days prior to the survey: avoiding eating out, avoiding using public transport, avoiding going to crowded places, rescheduling travel plans, cleaning or disinfecting household more often, avoiding visiting live poultry market, and avoiding eating poultry. All these items were dichotomized as “1 = yes” and “0 = no” for subsequent data analysis.
Perceived Susceptibility to H7N9 Infection
Respondents were asked about their perceived personal likelihood of being infected with H7N9 over the next 1 month. Responses for this item were seven-point Likert scale ranged from “never” to “certain.”
Perceived Severity of H7N9
One item each addressed respondents’ perception of H7N9 severity relative to SARS and A/H5N1, respectively. Responses for these two items were on five-point categorical scales that ranged from “Much lower” to “much higher.”
Worry About H7N9 Infection
One item addressed respondents’ anticipated level of worry about developing flu-like symptoms the next day. Responses for this item were on a seven-point categorical scale ranging from “not at all worried” to “extremely worried.” Another item asking respondents to rate their current level of worry about H7N9 infection on a scale from “1” to “10”, with 1 indicating “very mild” and 10 indicating “very severe.”
Demographics
Age, gender, education obtainment, place of birth, and marital status were collected at the end of the questionnaire.
Data Analysis
Proportions of adopting different protective behaviors across surveys were first calculated and weighted by age, gender, and educational achievement within the Hong Kong general population. Then, LCA was employed to explore latent classes regarding adoption of protective behavior among the respondents across the three surveys. To perform the LCA, all items on protective measures which had been dichotomized as described above were entered into Mplus 6.0 for data analysis. Mplus employs full information maximum likelihood (FIML) methods to handle missing data. Hence, all cases can be used for data analysis except for cases with data missing in all analyzed items [31]. To determine how many latent classes can best fit to our data, LCA was performed in an exploratory way starting with a single-class model. The model with “n + 1” classes was compared against model with “n” classes in terms of major model fit statistics including Akaike information criterion (AIC), Bayesian information criterion (BIC), sample size adjusted BIC (aBIC), and entropy value. Models with smaller values of AIC, BIC, and aBIC and greater entropy values were preferred. The simulation study suggested that BIC index was more accurate in determining the true number of classes in LCA based on large sample size (N = 1000) compared with AIC and aBIC [32]. Entropy has a value range from 0 to 1 with higher values indicating better quality of classification of the model [31]. Except for the model fit statistics, the principle of parsimony and model interpretability are another two critical criteria for determining the optimal number of latent classes [33]. Parsimony means that when other conditions are equal, model selection should favor the model with fewer freely estimated parameters. That is, the model with fewer latent classes should be selected. For multigroup models, model selection should also privilege models in which all groups have the same number of latent classes if the data can be easily interpreted based on the same model [33]. Using the above criteria, the optimal number of latent class was determined for each sample. LCA estimates both the item-response probabilities for each latent class and the class probabilities (latent class prevalence) within each sample.
If the number of latent classes is the same for the three samples based on the above procedure, multigroup LCA will be conducted to determine the equivalence in behavior patterns across samples, that is, the equivalence test of item-response probabilities for each latent class across the three samples while number of latent classes is set equal across samples. To do this, we compare the unconstrained model (M1) in which all item-response probabilities and class probabilities across the three samples were set free and a nested model (M2) in which item-response probabilities were set equal across samples but class probabilities were allowed to vary across samples. Then M1 and M2 will be compared for their likelihood ratio chi-square (G 2) and values of AIC and BIC. An insignificant p value (p > 0.05) associated with the difference G 2 statistics and smaller values of AIC and BIC suggest that the more restrictive model fits as well as the less restrictive model, then for the principle of parsimony, the more restrictive model will be selected [33]. If item-response probabilities could be constrained equal across samples, equivalence in class probabilities will then be tested by comparing M2 with a further nested model (M3) in which item-response probabilities and class probabilities across samples were set equal.
If item-response probabilities could be constrained equal across samples, the three samples will be combined into one to rerun the LCA to determine individual class memberships. The prevalence of latent classes across the three samples will then be compared using multinomial logistic regression model adjusted by sample age, gender, and educational attainment. Multinomial logistic regression models were also performed to determine factors associated with patterns of protective behavioral responses (latent class membership). The odds ratios (OR) of respondents with certain characteristic belonging to a particular class relative to belonging to the reference class and their corresponding 95 % confidence interval (CI) were estimated. p values of less than 0.05 were considered as statistically significant for all analysis.
Results
The characteristics of the respondents were generally comparable across the three surveys except that the second surveys comprised more respondents aged 34–55 years (Appendix Table). Adoption of the 14 preventive measures among the respondents across the three surveys is shown in Table 1. Generally, compliance to hand hygiene was high among respondents with more than 60 % across the three surveys. The prevalence of avoidance behaviors was generally low, but around one third of the respondents reported avoiding crowded places and avoiding markets where live poultry were sold.
Behavioral Patterns Regarding Adoption of Preventive Measures Across the Three Surveys
Table 2 shows that BIC values were lowest for the three-class model across all three surveys. Additionally, the entropy value was also highest for the three-class model in both the Dec-2013 and Jan-2014 surveys (Table 2). Although the values of AIC or aBIC continued to decline as the four-class model and the five-class model were tried, based on the principle of parsimony and model interpretation, the model with fewer latent classes that is easier to interpret and, for multiple groups, the model in which all groups can hold the same number of latent classes are preferred [33]. Therefore, according to the value of BIC, parsimony, and model interpretation, the three-class model was determined to be optimal in all three surveys.
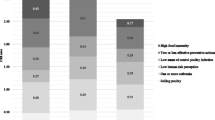
The profiles of the three latent classes across the three surveys were indicated by the estimated response probabilities on each preventive measure (item-response probabilities) for members within each latent class. A higher positive item-response probability indicated a higher chance a respondent would adopt a particular preventive measure. Figure 1 shows the positive response probabilities for each preventive measure in each latent class across the three surveys. It shows that the conditional item-response probabilities in each latent class only vary slightly across the three surveys, indicating that the profiles of three latent classes are comparable across the three surveys (Fig. 1). In all three surveys, Class 1 was characterized by a moderate probability of adopting basic hygiene practices including washing hands after sneezing or coughing, washing hands after returning home, and using liquid soap when washing hands. The probability of adopting other preventive measures in Class 1 was low. Therefore, we named this class “Moderate hygiene compliance” group. Class 2 had high compliance with most routine hygiene practices but low probabilities of adopting avoidance behaviors. Class 2 was labeled “Good hygiene compliance.” Class 3 was characterized by both high probabilities of adopting hygiene practices and relatively higher probabilities of avoidance behaviors relative to Classes 1 and 2. It indicates that this group of people may have heightened sensitivity toward threat signals in the environment, one manifestation of which is enhanced vigilance [34, 35]. Class 3 was labeled “Vigilance.”

Positive item-response probabilities of the preventive measures for members within each latent class across the three cross-sectional surveys. See footnote to Table 1 for interpretation of positive responses
Although item-response probabilities in each latent class across surveys were generally comparable, there was an obvious declining trend of adopting washing hands after sneezing and coughing for members of Class 1 across the three surveys while members of Class 3 apparently increased adoption of wearing face mask in the Jan-2014 survey but reduced that in the Feb-2014 survey (Fig. 1). Members of Class 3 also reduced their adoption of cleaning and disinfecting household, avoiding eating out, avoiding visiting live poultry markets, and avoiding eating poultry in the Feb-2014 survey (Fig. 1).
Multigroup LCA was further conducted to test equivalence in behavior patterns across samples. Table 3 shows the fit statistics for sets of nested models. The difference of G 2 between M2 (the more constrained model) and M1 (the unconstrained model) was statistically significant, indicating that M2 did not fit as well as M1. However, the large number of degree of freedom difference between these two models (∆d f = 86) raised a question about whether G 2 differences (∆G 2) could distribute approximately well by chi-square [33]. Furthermore, the lower values of AIC and BIC for M2 indicated that the more parsimonious M2 should be selected. Taking into account the comparable item-response probabilities within each latent class across samples (Fig. 1), we determined that item-response probabilities across samples could be equally constrained. Comparing M3 (the complete constrained model) with M2, the ∆G 2 indicated that M3 did not fit as well as M2. The higher value of AIC for M3 than for M2 also indicated that class probabilities were not equivalent across the three samples.
The prevalence of latent classes across the three surveys, after adjustment for sample age, gender, and educational attainment using a multinomial logistic regression model, indicated that only prevalence of Class 2 and Class 3 varied across surveys with prevalence of Class 2 being significantly lower while prevalence of Class 3 significantly increased in the Feb-2014 survey (Fig. 2).

Prevalence of latent class memberships across the three surveys. The error bars represent the 95 % confidence for each class probability estimated using multinomial logistic regression models
Factors Associated with Response Patterns
Since item-response probabilities can be set equal across the three surveys, indicating structure invariance of behavior patterns across samples, the three samples were subsequently treated as one sample for the purposes of examining factors associated with latent class membership. Table 4 shows comparisons of the characteristics and perceptions of H7N9 risk by the three latent classes. The three classes differed significantly in most characteristics including gender, age, educational achievement, place of birth, and marital status. Compared with the other two classes, respondents in Class 1 (moderate hygiene compliance) were more likely to be male, single, young respondents with higher educational attainment and born in Hong Kong. The three classes also differed in perceived personal susceptibility; perceived severity of H7N9 compared with A/H5N1; anticipated worry about developing flu-like symptoms; current worry about H7N9, with respondents in Class 3 (Vigilance) reporting the highest levels of perceived susceptibility; perceived severity; and anticipated worry and current worry toward H7N9 (Table 4).
Multinomial logistic regression model was conducted to examine factors associated with patterns of behavioral responses adjusted by study waves. The results (Table 5) indicated that compared with Class 1 (moderate hygiene compliance), Class 2 (High hygiene compliance), and Class 3 (Vigilance) were more likely to be female, older, better educated, perceived higher susceptibility, and had higher level of current worry toward H7N9. Furthermore, compared with Class 1 (moderate hygiene compliance), Class 3 members (Vigilance) were also more likely to be married or formerly married, perceive greater severity for H7N9 relative to A/H5N1, and report higher anticipated worry (Table 5).
Discussion
We believe this to be the first study that quantifies and characterizes population patterns of preventive behavior in the pre-epidemic stage. Across the three samples, we identified three comparable major patterns (classes) in preventive behavior: the moderate hygiene compliance, Good hygiene compliance, and Vigilance. This suggests that, currently within the context of repeated epidemic influenza irruptions from South China, the Hong Kong population may retain relative stable patterns of behavioral responses to a new infectious disease in the early stages, even as more confirmed cases of human infection were reported and the epidemic progressed [6]. The generally consistent item-response probabilities of a particular latent class across the three surveys further suggest structural invariance in behavior patterns [33] though it is possible that members of particular classes also change certain behaviors. For example, the Moderate hygiene compliance group reduced hand-washing after coughing or sneezing as the epidemic progressed but might have demonstrated an increase if the epidemic had significantly intensified. Moderate hygiene compliance defined the most prevalent group and its prevalence was comparable across the three surveys. Members in the Moderate hygiene compliance class may be quite resistant to changing their existing pattern of practices even if a potential epidemic is indicated but might change if significant increases in threat level are indicated. However, there were significant changes in prevalence of Class 2 (Good hygiene compliance) and Class 3 (Vigilance) in the third survey (Feb-2014 survey), suggesting that as the H7N9 epidemic became more severe in Mainland China and more imported H7N9 human cases were reported in Hong Kong; members of Class 2 may become more vigilant to the threat and thereby increase adoption of avoidance behaviors subsequently. However, this speculation awaits confirmation in future cohort surveys.
The Moderate hygiene compliance class accounted for around half of the respondents, who adopted only the most basic hand hygiene practices at a moderate level. Since it is unlikely that people will reduce their prevention practices in response to a growing epidemic threat, this pattern of practices is very likely to be habitual or even increased over the usual level seen in the absence of any epidemic activity. This class may contribute to transmitting infections such as seasonal influenza in their daily life or they might be late-stage responders who intensify protective behaviors only when risk is perceived to be imminent. Compared with the characteristics of the other two classes, respondents in this class were more likely to be male, younger, and less educated. This is consistent with previous studies conducted during SARS and the 2009 influenza A/H1N1 pandemic in Hong Kong [18, 19, 28], suggesting that these subpopulations should be considered for targeted public health interventions to control future outbreaks of infectious diseases.
The Good hygiene compliance class, which captured around one third of respondents, was characterized by greater hygiene practices relative to Class 1 but few avoidance behaviors. However, members of this group perceived generally comparable levels of threat from H7N9 to members of Moderate hygiene compliance except that members in Good hygiene compliance reported slightly higher perceived susceptibility and level of current worry about H7N9. The comparable risk perception patterns to those seen in Moderate hygiene compliance members suggest that habitual preventive practices dominate in this class also. The occasional avoidance behavior characterizing the behavior pattern of members in Good hygiene compliance suggests that they may have greater propensity toward modifying behavior should threat increase, through adopting greater avoidance and intensification of prevention.
Previous mathematical models concluded that early behavioral change in response to an epidemic is small and should have little impact on the development of the epidemic [36]. However, the present study suggests that even in the early pre-epidemic stage, when there is little evidence for human-to-human transmission of H7N9 and no locally acquired cases, around 13–20 % of the respondents had reported high compliance to most hygiene practices and avoidance behaviors, indicating high vigilance to the threat. Except for high compliance to hygiene practices, this group also adopted more avoidance behaviors that were recommended by the government of Hong Kong, suggesting that this group had high compliance to government recommendation in the prevention of H7N9. The odds of an individual being assigned to this group were positively associated with greater perceived threat from H7N9 relative to members in the other two classes. Female, older, married, and better educated individuals were more likely to belong to Class 3 compared to the other two classes. This was also consistent with previous studies conducted during SARS [14, 19].
Previous studies have indicated that humans are inherently heterogeneous in their attention to threat, which is closely linked to personality characteristics such as neuroticism and trait anxiety [34, 35, 37]. For example, people who are generally more anxious would be expected to show high vigilance for potential threat information [34, 35]. Variation in these personality characteristics generates variable attentional bias in information processing and, coupled with cognitive style manifests as enhanced, or blunted vigilance toward threat-related information [38, 39]. This might help to explain the spectrum of active and passive behaviors seen when different individuals face a common threat signal. However, we did not measure neuroticism or trait anxiety among the respondents and thereby cannot conclude whether the heterogeneity in behavioral responses to this new infectious diseases was due to variation in these personality characteristics or not. However, the significant difference in perceived threat of H7N9 among the three classes suggests that variation in perceived vulnerability at least partially explained the behavioral heterogeneity across classes. Such variability has long been described with younger males particularly poor at risk estimates and overconfident in their abilities to control risk impacts [23, 40], so this may reflect a developmental state.
This study had some limitations. First, although the three independent cross-sectional surveys enable observing the change in profiles and prevalence of each behavior pattern, the actual growth and decay of preventive behaviors in these three classes within the evolution of an epidemic remain unknown. Longitudinal studies should be conducted throughout future epidemics to more precisely investigate these research questions. Second, sampling errors may be a reason for the variation in prevalence of behavior patterns across surveys. However, the three cross-sectional surveys were conducted using the same sampling methods, and the demographics of the three samples were generally comparable. We had further adjusted the difference in the prevalence of behavioral patterns by sampling age, gender, and education to minimize the influence of sampling errors on behavioral variation across samples. Third, our measure of perceived personal susceptibility to H7N9 was not conditional on “not taking any prevention.” This may lead to underestimation of the true association between perceived personal susceptibility and adoption of prevention if some respondents estimated their personal susceptibility to be low because they had taken the preventive behaviors [41]. Furthermore, although LCA provides significant insights in guiding public health practices, how to determine the optimal number of classes using LCA can be as much an art as a science [31]. Here, we determined the final number of latent classes based on BIC, entropy value, the principle of parsimony, and the model interpretation, factors which have been suggested to be more important over other model fit indices in simulation studies [31–33]. Finally, since all behaviors were measured relying on self-reported data, the results may be subject to social desirability bias. As a result, the actual size of the second and the third classes may be overestimated.
In conclusion, Hong Kong’s population may evidence three major protective behavior response classes in the face of preliminary threat from H7N9, tentatively named: Moderate hygiene compliance, Good hygiene compliance, and Vigilance. These three classes reflect different levels of adoption of protection which may translate to different levels of vulnerability toward contracting and spreading H7N9 infection or instead may be a reflection of generalized compliance behavior. It appears that as epidemic threat increases, more people in Good hygiene compliance may transfer to the Vigilance group while that of Moderate hygiene compliance may remain unchanged. However, it remains unknown how the trajectories of change in these behavioral practices will unfold as the threat level evolves throughout an epidemic. Given the present limited data, young, mostly single males and those with lower educational achievement represent a group for whom public health messages need to be targeted.
References
Gao R, Cao B, Hu Y, Feng Z, Wang D, Hu W, et al. Human infection with a novel avian-origin influenza A (H7N9) virus. N Engl J Med. 2013;368:1888–97.
Cowling BJ, Jin L, Lau EH, Liao Q, Wu P, Jiang H, et al. Comparative epidemiology of human infections with avian influenza A H7N9 and H5N1 viruses in China: a population-based study of laboratory-confirmed cases. Lancet. 2013;382:129–37.
Li Q, Zhou L, Zhou M, Chen Z, Li F, Wu H, et al. Preliminary report: epidemiology of the avian influenza A (H7N9) outbreak in China. N Engl J Med. 2013;370:520–32.
Yu H, Wu JT, Cowling BJ, Liao Q, Fang VJ, Zhou S, et al. Effect of closure of live poultry markets on poultry-to-person transmission of avian influenza A H7N9 virus: an ecological study. Lancet. 2013;383:541–8.
Center for Health Protection Hong Kong. CHP closely monitors two additional human cases of avian influenza A(H7N9) in Mainland. Government of Hong Kong Hong Kong. 30 March 2014. http://www.chp.gov.hk/en/content/116/34056.html. Accessed 1 April 2014.
World Health Organization. Confirmed human cases of avian influenza A(H7N9) reported to WHO. 2014. http://www.who.int/influenza/human_animal_interface/influenza_h7n9/17_ReportWebH7N9Number_20140408.pdf?ua=1. Accessed 10 May 2014.
Center for health Protection Hong Kong. Epidemiological investigation and follow-up actions by CHP on confirmed human case of avian influenza A(H7N9) Government of Hong Kong, Hong Kong. 14 April 2014. http://www.chp.gov.hk/en/content/116/34363.html. Accessed 16 Apirl 2014.
Del Valle SY, Hyman JM, Chitnis N. Mathematical models of contact patterns between age groups for predicting the spread of infectious diseases. Math Biosci Eng. 2013;10:1475–97.
Eames KT, Tilston NL, Brooks-Pollock E, Edmunds WJ. Measured dynamic social contact patterns explain the spread of H1N1v influenza. PLoS Comput Biol. 2012;8:e1002425.
Mossong J, Hens N, Jit M, Beutels P, Auranen K, Mikolajczyk R, et al. Social contacts and mixing patterns relevant to the spread of infectious diseases. PLoS Med. 2008;5:e74.
McCutcheon AL. Latent class analysis, Sage University paper series on quantitative applications in the social science, vol. 07-064. CA: Sage; 1987.
Schuckit MA, Smith TL, Danko GP, Bucholz KK, Agrawal A, Dick DM, et al. Predictors of subgroups based on maximum drinks per occasion over six years for 833 adolescents and young adults in COGA. J Stud Alcohol Drugs. 2014;75:24–34.
Jackson N, Denny S, Sheridan J, Fleming T, Clark T, Teevale T, et al. Predictors of drinking patterns in adolescence: a latent class analysis. Drug Alcohol Depend. 2014;135:133–9.
Bish A, Michie S. Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. Br J Health Psychol. 2010;15:797–824.
Becker MH, Haefner DP, Maiman LA. The health belief model in the prediction of dietary compliance: a field experiment. J Health Soc Behav. 1977;18:348–66.
Rogers RW. Cognitive and physiological processes in fear appeals and attitude change: a revised theory of protection motivation. In: Cacioppo JT, Petty RE, editors. Social psychophysiology: a source book. New York: Guilford; 1983. p. 153–76.
Barr M, Raphael B, Taylor M, Stevens G, Jorm L, Giffin M, et al. Pandemic influenza in Australia: using telephone surveys to measure perceptions of threat and willingness to comply. BMC Infect Dis. 2008;8:117.
Leung GM, Lam TH, Ho LM, Ho SY, Chan BH, Wong IO, et al. The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. J Epidemiol Community Health. 2003;57:857–63.
Leung GM, Ho LM, Chan SK, Ho SY, Bacon-Shone J, Choy RY, et al. Longitudinal assessment of community psychobehavioral responses during and after the 2003 outbreak of severe acute respiratory syndrome in Hong Kong. Clin Infect Dis. 2005;40:1713–20.
Tang CS, Wong CY. An outbreak of the severe acute respiratory syndrome: predictors of health behaviors and effect of community prevention measures in Hong Kong, China. Am J Public Health. 2003;93:1887–8.
Lau JT, Yang X, Tsui H, Kim JH. Monitoring community responses to the SARS epidemic in Hong Kong: from day 10 to day 62. J Epidemiol Community Health. 2003;57:864–70.
Jones JH, Salathe M. Early assessment of anxiety and behavioral response to novel swine-origin influenza A(H1N1). PLoS ONE. 2009;4:e8032.
Gustafson PE. Gender differences in risk perception: theoretical and methodological perspectives. Risk Anal. 1998;18:805–11.
Rubin GJ, Amlot R, Page L, Wessely S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: cross sectional telephone survey. BMJ. 2009;339:b2651.
Tang CS, Wong CY. Psychosocial factors influencing the practice of preventive behaviors against the severe acute respiratory syndrome among older Chinese in Hong Kong. J Aging Health. 2005;17:490–506.
Government of Hong Kong. Live poultry imported from Mainland tested positive for H7 avian influenza virus. In: Press Releases. Hong Kong. 27 January 2014. http://www.info.gov.hk/gia/general/201401/27/P201401270847.htm. Accessed 28 February 2014.
Hong Kong Office of the Telecommunications Authority. Key telecommunications statistics. Hong Kong. 2013. http://www.ofca.gov.hk/mobile/en/media_focus/data_statistics/key_stat/index.html. Accessed 07 Jan 2017.
Cowling BJ, Ng DM, Ip DK, Liao Q, Lam WW, Wu JT, et al. Community psychological and behavioral responses through the first wave of the 2009 influenza A(H1N1) pandemic in Hong Kong. J Infect Dis. 2010;202:867–76.
Fielding R, Lam WW, Ho EY, Lam TH, Hedley AJ, Leung GM. Avian influenza risk perception, Hong Kong. Emerg Infect Dis. 2005;11:677–82.
Liao Q, Cowling BJ, Lam WW, Fielding R. The influence of social-cognitive factors on personal hygiene practices to protect against influenzas: using modelling to compare avian A/H5N1 and 2009 pandemic A/H1N1 influenzas in Hong Kong. Int J Behav Med. 2011;18:93–104.
Geiser C. Latent class analysis. In: Little TD, editor. Data analysis with Mplus. New York: The Guilford; 2013. p. 232–70.
Nylund K, Asparouhov T, Muthen BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Struct Equ Model. 2007;14:535–69.
Collins LM, Lanza ST. Latent class and latent transition analysis: with applications in the social, behavioral, and health sciences. Hoboken: Wiley; 2010.
Oathes DJ, Squillante CM, Ray WJ, Nitschke JB. The impact of worry on attention to threat. PLoS ONE. 2010;5:e13411.
Ioannou MC, Mogg K, Bradley BP. Vigilance for threat: effect of anxiety and defensiveness. Personal Individ Differ. 2004;36:1879–91.
Sahneh FD, Chowdhury FN, Scoglio CM. On the existence of a threshold for preventive behavioral responses to suppress epidemic spreading. Sci Rep. 2012;2:632.
Etkin A, Klemenhagen KC, Dudman JT, Rogan MT, Hen R, Kandel ER, et al. Individual differences in trait anxiety predict the response of the basolateral amygdala to unconsciously processed fearful faces. Neuron. 2004;44:1043–55.
Mathews A. Why worry? The cognitive function of anxiety. Behav Res Ther. 1990;28:455–68.
Derakshan N, Eysenck MW, Myers LB. Emotional information processing in repressors: the vigilance–avoidance theory. Cogn Emot. 2007;21:1585–614.
Savage I. Demographic influences on risk perceptions. Risk Anal. 1993;13:413–20.
Brewer NT, Chapman GB, Gibbons FX, Gerrard M, McCaul KD. Meta-analysis of the relationship between risk perception and health behavior: the example of vaccination. Health Psychol. 2007;26:136–45.
Acknowledgments
This work was supported by the Health and Medical Research Fund of the Health, Welfare and Food Bureau of the Hong Kong SAR Government (grant no. RRG-12), Area of Excellence Scheme of the Hong Kong University Grants Committee (grant no. AoE/M-12/06), and the Harvard Center for Communicable Disease Dynamics from the National Institute of General Medical Sciences (grant no. U54 GM088558). The authors thank Vicky Fang and Diane Ng for the technical support.
Conflict of Interest
BJC reports receipt of research funding from MedImmune Inc. and Sanofi Pasteur for studies of influenza vaccines and consulted for Crucell NV. The authors declare no other potential conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Liao, Q., Cowling, B.J., Wu, P. et al. Population Behavior Patterns in Response to the Risk of Influenza A(H7N9) in Hong Kong, December 2013–February 2014. Int.J. Behav. Med. 22, 672–682 (2015). https://doi.org/10.1007/s12529-015-9465-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-015-9465-3