
Abstract
Objectives
We explored the relationship between bone mineral density (BMD) and lifestyle in juveniles to identify factors leading to higher peak bone mass and prevention of osteoporosis in later life.
Methods
Juveniles (1,364 students: 770 boys and 594 girls, aged 6–18 years) attending school in Hokkaido prefecture, Japan, were asked to complete a brief self-administered diet history questionnaire for 10-year-olds (BDHQ10y) providing information about personal history, lifestyle, and intake of nutritional elements. In addition, BMD and grip strength were measured. We analyzed the relationship between BMD and lifestyle factors.
Results
The difference in BMD for boys was larger among the junior and senior high school groups. The difference in BMD for girls was larger among older elementary and later school children. Anthropometric variables and grip strength were strongly correlated with BMD. Having a nap-time routine was significantly correlated with BMD, but sleep time and sports club activities were not. BMD among juveniles who attained secondary sexual characteristics was significantly higher than that of juveniles of the same age who had not attained these characteristics. Calcium intake was significantly lower in senior high school students compared with other grades. Consumption of milk by senior high school boys and junior high school girls was weakly correlated with BMD.
Conclusions
Our findings encourage educational interventions to counsel students to avoid weight loss and calcium deficiency. This effective intervention should begin before the higher elementary school, when juveniles have the greatest likelihood for preventing lower peak bone mass and osteoporosis.
Similar content being viewed by others

Introduction
Osteoporosis is a common clinical condition affecting an estimated 7.8–11 million people in Japan [1]. As bone fractures not only reduce quality of life but also lead to immobility in elderly people, preventing osteoporosis is an important concern in health care. Three primary strategies for preventing osteoporotic fracture have been identified: (1) minimizing bone loss in postmenopausal women, (2) preventing falls in elderly adults, and (3) increasing peak bone mass in adolescents. Recently, calcium intake and moderate exercise have attracted attention as strategies for preventing the development of osteoporosis by increasing peak bone mass in adolescence [2–6]. It has been reported that a 10% increase in peak bone mass is predicted to delay the development of osteoporosis by 13 years [7].
There are several methods for measuring bone mass and bone mineral density (BMD), such as quantitative ultrasound and dual X-ray absorptiometry (DXA) [8]. BMD measurement using DXA is one of the important elements in diagnosing osteoporosis and screening people at a high risk of fracture. DXA is a convenient method for measuring osteoporosis in many people because it is both quick and inexpensive. The age of peak bone mass differs at various skeletal sites (lumbar spine, femoral neck, trochanter, intertrochanter, Ward’s triangle, total hip, distal one third of the radius, and ultradistal forearm) [9]. The distal one third of the radius has been used when measurement of the lumbar spine could not be obtained. Peak bone mass in the distal one third radial BMD by DXA has been reported to be achieved by the third decade of life [8, 9]. Recently, several reports investigating BMD in juveniles have added to the previously accumulated data obtained for elderly adults in Japan [10]. However, few reports have surveyed the correlation between BMD and lifestyle in elementary and junior high school students [11]. In particular, insufficient data on BMD have been obtained from young boys, as the participants in most of the previous studies were girls. Furthermore, the examination methods used to assess the relationship between daily diet and BMD have been simple. In most of the previous studies conducted in Japanese populations, a 3-day dietary record or simple questionnaire has been used for dietary assessment, and it was difficult to examine the correlation between BMD and detailed nutrient factors [12, 13]. Therefore, in this study, we used the brief self-administered diet history questionnaire for 10-year olds (BDHQ10y), a semiquantitative food frequency questionnaire that asked the dietary habits of the previous month [14, 15].
The aim of the study was to explore the relationship between BMD and lifestyle, including nutrient intake, sports club activity, and sleep time, in juveniles to identify educational intervention methods to prevent osteoporosis in later life by achieving high peak bone mass in juveniles.
Methods
Subjects
Participants were 1,392 students aged 6–18 years attending school in seven municipalities throughout Hokkaido prefecture, Japan. Informed consent to participate in the study, including BMD measurement and completion of the questionnaire, was obtained from students and their guardians. Participants for whom BMD data could not be obtained were excluded from the analysis, leaving a study group of 1,364 (770 boys and 594 girls). This survey was carried out from September 2002 to September 2005.
BMD measurement
BMD was measured by DXA at the distal forearm of the nondominant side (DTX-200; Osteometer MediTech Inc., CA, USA), as previously described [9]. When the participants had a history of bone fracture or any bone diseases in the nondominant side, the other side was scanned.
Anthropometric measurement
Data for weight (kg) and standing height (cm) of each participant were obtained from the most recent anthropometric measurement records at their school. Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared.
Grip strength measurement
The grip strength of the nondominant side was measured twice using a digital grip dynamometer (Grip-D; Takei Scientific Instruments Co., Ltd., Niigata, Japan), and the stronger values were used for analysis.
Questionnaire
Lifestyle, participation in sports club activities, secondary sexual characteristics (data on change in voice and menstrual status), history of bone fracture at any site, personal medical history, current therapy, and milk consumption were assessed with a self-administered questionnaire. If the participants could not fill in the questionnaire by themselves, their guardian was asked to complete it with them. Nutrient intake was assessed with the BDHQ10y. Total calories and five nutrients, i.e., calcium, phosphorus, and vitamins A, C, and D, which previous studies [16–19] have suggested influence BMD, were calculated for each participant and included in the analysis.
Statistical analysis
The difference in BMD by calendar age was analyzed by one-way analysis of variance (ANOVA) or, if necessary, by the Bonferroni method to identify differences. Spearman rank correlation coefficient with BMD was computed for milk consumption, grip strength, and anthropometric variables such as body height, body weight, and BMI. Differences in BMD between two groups divided by lifestyle were analyzed by Student’s t test. To investigate the relationship between secondary sexual characteristics and BMD, participants were divided into two groups, as follows: boys were divided into “before” or “after” groups based on change in voice; girls were divided into “before” or “after” groups based on menarche. We used data from boys aged 12–14 years and girls aged 11–13 years to analyze the correlation between secondary sexual characteristics and BMD. The participants were divided into four groups according to their grade of school, i.e., lower elementary, higher elementary, junior high, and senior high student, to analyze milk consumption and total calorie and nutrient intake. The means among them were compared using Kruskal–Wallis rank test or, if necessary, by Mann–Whitney U test corrected by the Bonferroni method to identify differences. Multivariate analysis of BMD, anthropometric, lifestyle, and nutrient data was performed by multiple linear regression analysis. P values <5% were considered statistically significant in all analyses. All statistical analyses were performed using SPSS for Windows version 14.0 (SPSS, Chicago, IL, USA).
Ethical issues
The Ethics Committee of Asahikawa Medical College, Asahikawa, Japan, approved the study protocol.
Results
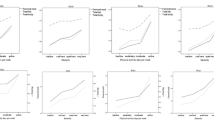
Mean values and standard deviations (SDs) of BMD according to gender and calendar age are presented in Fig. 1. The difference in BMD was compared between the two adjacent calendar ages in each gender. The difference in BMD for boys was larger among the junior and senior high school groups. The SD of male BMD after age 12–13 years was larger than before. On the other hand, although the difference in BMD for girls was larger among older elementary school children and later groups, the difference was moderate among junior high school and almost plateaued in senior high school participants aged 16–18 years. The SD of female BMD after 12–13 years was larger than before.

Bone mineral density (BMD) of study participants by calendar age in each gender. *p < 0.05, **p < 0.01, ***p < 0.001 according to Bonferroni method for multiple comparison (for boys only); † p < 0.05 according to Bonferroni method for multiple comparison (for girls only)
Each anthropometric variable was strongly correlated with BMD [body height (boys and girls): r = 0.701 and r = 0.689; body weight r = 0.823, r = 0.826; BMI r = 0.716, r = 0.763; all correlations were p < 0.001]. Grip strength was strongly correlated with BMD (boys r = 0.811, girls r = 0.758; p < 0.001, respectively). Multiple linear regression analysis was performed with BMD as the dependent variable, with sex, calendar age, BMI, and grip strength as independent variables. The regression coefficient of any independent variable was significant (p < 0.001) (Table 1).
Multiple linear regression analysis was then performed with BMD as the dependent variable, with sex, calendar age, BMI, and sports club activities as independent variables. The regression coefficient of sports club activities was not significant (p = 0.360) (Table 2). Similarly, sleep time, having a nap-time routine, and history of bone fracture were analyzed by multiple linear regression analysis. The regression coefficient of having a nap-time routine was significant (p < 0.01), but the regression coefficient of sleep time was not significant (p = 0.059). The regression coefficient of history of bone fracture was not significant (p = 0.330).
The relationship between secondary sexual characteristics and BMD is shown in Fig. 2. Among boys aged 12–14 years, BMD in the “after change in voice” group was higher than that in the “before change in voice” group, and significance was detected at the age of 12 and 13 years. Among girls aged 11–13 years, BMD in the “after menarche” group was significantly higher than that in the “before menarche” group.

The relationship between secondary sexual characteristics and bone mineral density (BMD). a Comparison of BMD between the “before change in voice” and “after change in voice” groups in boys. b Comparison of BMD between the “before menarche” and “after menarche” groups in girls. *p < 0.05, **p < 0.01
Milk is a common food that provides a ready source of calcium. Milk consumption was significantly lower in senior high school students compared with other grades for both genders (Fig. 3). The correlation between milk consumption and BMD was analyzed and correlated weakly with BMD in senior high school boys and junior high school girls (Table 3).

Mean values for daily milk consumption. LE lower elementary student, HE higher elementary student, JH junior high school student, SH senior high school student. ***p < 0.001 according to Bonferroni method for multiple comparison
Figure 4 shows means ± SDs of daily total calorie and calcium intakes based on the BDHQ10y. Total calorie intake of boys in junior high school students was significantly higher than that in lower elementary school children (p < 0.05). Total calorie intake of girls in senior high school students was significantly lower than that in lower elementary school children (p < 0.05) and higher elementary school children (p < 0.01). Calcium intake was significantly lower in senior high school students compared with other grades for both genders. Other nutrient elements showed a similar tendency as total calories. Intake of total calories; calcium; phosphorus; and vitamins A, C, and D were independent of BMD by multiple linear regression analysis (Table 4).

Mean values for daily total calorie and calcium intakes based on the brief self-administered diet history questionnaire for 10-year-olds (BDHQ10y). a Total calorie and b calcium. LE lower elementary student, HE higher elementary student, JH junior high school student, SH senior high school student. *p < 0.05, **p < 0.01 according to Bonferroni method for multiple comparison
Discussion
Few reference data on forearm BMD obtained using the DXA method are available for Japanese juveniles [20]. Most previous studies of BMD in juveniles included only girls and did not include elementary school children [13]. This study reports general population-based data on forearm BMD in Japanese juveniles. We used the BDHQ10y, which asked participants to report their dietary habits for the previous month. The BDHQ10y was easy to research and standardize and made it possible to investigate comparatively long-term dietary habits. The BDHQ10y had the advantage of not causing a day-to-day variation. The BDHQ10y was useful to clarify the correlation between BMD and detailed nutrient factors. Responses to the BDHQ10y provided detailed information on nutritional elements and total calories, enabling us to analyze the correlation between BMD and specific nutritional elements. Therefore, the data from this study are important for preventing osteoporosis.
The difference in BMD for boys peaked among junior to senior high school groups, and the SD after age 12–13 years was larger than before. The difference in BMD for girls peaked among higher elementary school children and declined at age 17–18 years, and the SD of BMD after 11–12 years was larger than before. The widening SD for BMD indicates a time lag in the growth spurt of BMD among individuals and that that time is a critical period for increasing BMD. In other words, the period before 12–13 years of age in boys and before 11–12 years of age in girls is an important time for intervention to increase peak bone mass. Matsukura et al. [20] reported that BMD increased steadily with age in boys and increased with age and then plateaued in girls among Japanese children and adolescents. Our results indicate a similar tendency, although the mean value for BMD was different. This difference could be caused by differences in measurement site; specifically, other studies measured at one third of the forearm length proximal to the ulnar end plate and the ultradistal forearm, and we measured at the distal forearm.
It is agreed that BMD and anthropometric variables are strongly correlated. A significant relationship between BMD and anthropometric variables such as body weight has been reported [21, 22], and low body weight was reported to be the major risk factor for low peak bone mass [6, 23, 24]. Our results support this correlation. The strongest factor that correlated with BMD was body weight. Grip strength was strongly correlated with BMD after adjusting for sex, calendar age, and BMI. There is ample evidence that mechanical stimuli can increase bone strength. Accordingly, physical exercise seems to prevent bone loss and possibly induce increases in bone mass, even at older ages [25]. However, our results show that the regression coefficient of sports club activities and BMD are not significant. There are two possible explanations: (1) physical activities other than sports club activities largely affected BMD increase, or (2) the difference among sporting events affected BMD increase. Maimoun et al. [26] reported that BMD in triathletes was higher than in controls and swimmers, and no differences in BMD were found among cyclists, swimmers, and controls. There have been many reports on the effects of exercise on BMD [6, 27, 28]. These correlations in juveniles require further exploration.
The supine position in bed places a light load on bones, and during nighttime sleep, hormonal secretion varies from the waking state [29–31]. Therefore, it is thought that sleep periods may provide a chance to change bone remodeling. Specker [32] reported that sleep deprivation is associated with lower BMD outcomes in some, but not all, individuals. Our results show that frequent or habitual napping was associated with BMD increase but that nighttime sleeping was not associated with such increase. Students who had a habit of napping might spend longer periods sleeping than other students. Sports club activities might also be a confounding factor because students who participate in sports club activities are estimated to sleep longer and nap more often than other students, as they get more tired. Detailed data are required to determine the effects of sleep.
BMD in juveniles in the period after the development of secondary sexual characteristics, identified as change in voice in boys and menarche in girls, was higher than that in juveniles of the same age in the period before development of these characteristics. This indicates that juveniles who developed secondary sexual characteristics at an early age had higher BMD. In other words, BMD was markedly increased at the secondary sexual characteristic period. However, this study could not clarify the relationship between secondary sexual characteristics and peak bone mass because the study was cross-sectional, and BMD increase continued after 17–18 years of age. Iki et al. [3] suggested that marked BMD increase occurred in boys after pubic hair appeared and before menarche in girls. Therefore, it is recommended that educational intervention to prevent osteoporosis begin before puberty.
Although this study shows no significant correlation between BMD and any nutritional elements, we identified some problems related to dietary habits in adolescence. The mean total calorie level in senior high school students was equivalent to that in junior high school students. This might suggest that senior high school students ate food that was not included in the BDHQ10y to obtain the necessary calories. Calcium intake was lower than the dietary reference value for all ages and noticeably lower among senior high school students. In addition, they might try to lose weight, which results in lack of calcium. The relationship between weight change and BMD change was significant [33]. This report supports that weight loss would cause adverse effect for BMD increase. Moreover, calcium intake tends to be less in ordinary daily meals in Japan because consumption of dairy products is lower than in Europe or the USA [34]. Consequently, osteoporosis risk in later life for Japanese people could be increased, as they did not have enough calcium in adolescence, when additional calcium is needed to obtain greater BMD.
Milk is a readily available source of calcium. Milk and dairy products are excellent foods due not only to their high calcium content but also to their high absorption rates [35]. As drinking milk has been recommended as a means for preventing calcium deficiency, we investigated the effectiveness of drinking milk on BMD increase in adolescents. We found a relationship between milk consumption and BMD in the same age group. Cadogan [36] reported that increased milk consumption significantly enhances bone mineral acquisition in adolescent girls. However, intake of calcium has been shown to decrease significantly in senior high school students compared with other age groups. At the same time, milk consumption has been shown to decrease significantly in senior high school students compared with other age groups. In Japan, junior high schools and elementary schools have provided lunch services that include milk. However, senior high schools do not have a school-provided lunch service, resulting in decreased milk consumption. This decrease has been suggested as a reason for a decrease in calcium intake. Xueqin [37] reported that a school-milk intervention trial enhanced bone mineral accretion in Chinese girls. That report suggests milk service in school is an effective way to increase BMD. Although our results do not indicate that BMD was dependent on intake of calcium, it was a problem that calcium intake, particularly among senior high school students, was less than the dietary reference value. Calcium intake that supplements this decrease might be necessary because BMD increase continued after junior high school.
This study has several limitations. First, it is a cross-sectional study, and BMD data may have been affected by past lifestyle habits. The questionnaire asked mainly about present habits, and the results could probably be influenced by a changed lifestyle habit of the past. Second, although the BDHQ10y was adapted for juveniles, it could not support all age groups. In particular, dietary consumption among senior high school students tended to be underrated. Although these limitations made the analysis more difficult, it is still possible to compare nutritional elements among the same grade groups.
In conclusion, this study elucidates several factors related to an increase of BMD in Japanese juveniles: Maintaining adequate body weight for obtaining higher peak bone mass. Calcium intake, particularly among senior high school students, was low, and considering the dietary reference values for children 15–17 years (boy 800 mg/day and girl 700 mg/day), this intake level was a problem. It has been suggested that avoiding weight loss and calcium deficiency may prevent lower peak bone mass and osteoporosis. Moreover, effective educational intervention to obtain higher peak bone mass must begin before the higher elementary school.
References
Yamamoto I. Estimation of osteoporosis population. Osteoporos Jpn. 1999;7:10–1. (article in Japanese).
Wosje KS, Specker BL. Role of calcium in bone health during childhood. Nutr Rev. 2000;58:253–68.
Iki M, Naka H, Sato H. A cross-sectional study on bone mineral density at the spine and hip and its determinants in Japanese children and adolescents. Osteoporos Jpn. 2003;11:266–9. (article in Japanese).
Hirota T, Hirota K. Exercise and other lifestyle factors for prevention of osteoporosis during growth and young adulthood. Clin Calcium. 2002;12:489–94. (article in Japanese).
Fujita Y, Katsumata K, Unno A, Tawa T, Tokita A. Factors affecting peak bone density in Japanese women. Calcif Tissue Int. 1999;64:107–11.
Ho AY, Kung AW. Determinants of peak bone mineral density and bone area in young women. J Bone Miner Metab. 2005;23:470–5.
Hernandez CJ, Beaupre GS, Carter DR. A theoretical analysis of the relative influences of peak BMD, age-related bone loss and menopause on the development of osteoporosis. Osteoporos Int. 2003;14:843–7.
Ishikawa K, Ohta T. Radial and metacarpal bone mineral density and calcaneal quantitative ultrasound bone mass in normal Japanese women. Calcif Tissue Int. 1999;65:112–6.
Iki M, Kagamimori S, Kagawa Y, Matsuzaki T, Yoneshima H, Marumo F. Bone mineral density of the spine, hip and distal forearm in representative samples of the Japanese female population: Japanese population-based osteoporosis (JPOS) study. Osteoporos Int. 2001;12:529–37.
Ikeda Y, Iki M, Morita A, Kajita E, Kagamimori S, Kagawa Y, et al. Intake of fermented soybeans, natto, is associated with reduced bone loss in postmenopausal women: Japanese population-based osteoporosis (JPOS) study. J Nutr. 2006;136:1323–8.
Tamaki J, Ikeda Y, Morita A, Sato Y, Naka H, Iki M. Which element of physical activity is more important for determining bone growth in Japanese children and adolescents: the degree of impact, the period, the frequency, or the daily duration of physical activity? J Bone Miner Metab. 2008;26:366–72.
Uenishi K, Ishida H, Nakamura K. Development of a simple food frequency questionnaire to estimate intakes of calcium and other nutrients for the prevention and management of osteoporosis. J Nutr Sci Vitaminol. 2008;54:25–9.
Tsukahara N, Sato K, Ezawa I. Effects of physical characteristics and dietary habits on bone mineral density in adolescent girls. J Nutr Sci Vitaminol. 1997;43:643–55.
Sasaki S, Yanagibori R, Amano K. Self-administered diet history questionnaire developed for health education: a relative validation of the test-version by comparison with 3-day diet record in women. J Epidemiol. 1998;8:203–15.
Sasaki S. Association between current nutrient intakes and bone mineral density at calcaneus in pre- and postmenopausal Japanese women. J Nutr Sci Vitaminol. 2001;47:289–94.
Welton DC, Kemper HC, Post GB, van Staveren WA. A meta-analysis of the effect of calcium intake on bone mass in young and middle aged females and males. J Nutr. 1995;125:2802–13.
Feskanich D, Singh V, Willett WC, Colditz GA. Vitamin A intake and hip fractures among postmenopausal women. JAMA. 2002;287:47–54.
Simon JA, Hudes ES. Relation of ascorbic acid to bone mineral density and self-reported fractures among US adults. Am J Epidemiol. 2001;154:427–33.
Nakamura K, Iki M. Efficacy of optimization of vitamin D in preventing osteoporosis and osteoporotic fractures: a systematic review. Environ Health Prev Med. 2006;11:155–70.
Matsukura T. Reference data of forearm bone mineral density in healthy Japanese male and female subjects in the second decade based on calendar age and puberty onset: Japanese population-based osteoporosis (JPOS) study. Osteoporos Int. 2000;11:858–65.
Saito T. Weight gain in childhood and bone mass in female college students. J Bone Miner Metab. 2005;23:69–75.
Nara H, Iki M, Morita A, Ikeda Y. Effects of pubertal development, height, weight, and grip strength on the bone mineral density of the lumbar spine and hip in peripubertal Japanese children: Kyoto kids increase density in the skeleton study (Kyoto KIDS study). J Bone Miner Metab. 2005;23:463–9.
Matsueda M, Takahashi K, Seino Y. The effects of growth, maturation and life-style on acquiring bone strength during adolescence: a comparison between males and females. Jpn J School Health. 2001;43:199–210.
Takahata Y. Peak bone mass of the calcaneus and the factors influencing it during adolescence. Osteoporos Jpn. 2007;15:573–82.
Rittweger J. Can exercise prevent osteoporosis? J Musculoskelet Neuronal Interact. 2006;6:162–6.
Maimoun L, Mariano-Goulart D, Couret I, Manetta J, Peruchon E, Micallef JP, et al. Effects of physical activities that induce moderate external loading on bone metabolism in male athletes. J Sports Sci. 2004;22:875–83.
Valdimarsson O, Linden C, Johnell O, Gardsell P, Karlsson MK. Daily physical education in the school curriculum in prepubertal girls during 1 year is followed by an increase in bone mineral accrual and bone width—data from the prospective controlled Malmö pediatric osteoporosis prevention study. Calcif Tissue Int. 2006;78:15–71.
Wallace BA, Cumming RG. Systematic review of randomized trials of the effect of exercise on bone mass in pre- and postmenopausal women. Calcif Tissue Int. 2000;67:10–8.
Spiegel K, Leproult R, Van Cauter E. Impact of sleep debt on metabolic and endocrine function. Lancet. 1999;354:1435–9.
Blumsohn A, Herrington K, Hannon RA, Shao P, Eyre DR, Eastell R. The effect of calcium supplementation on the circadian rhythm of bone resorption. J Clin Endocrinol Metab. 1994;79:730–5.
Chapotot F, Gronfier C, Spiegel K, Luthringer R, Brandenberger G. Relationships between intact parathyroid hormone 24-hour profiles, sleep-wake cycle, and sleep electroencephalographic activity in man. J Clin Endocrinol Metab. 1996;81:3759–65.
Specker BL, Binkley T, Vukovich M, Beare T. Volumetric bone mineral density and bone size in sleep-deprived individuals. Osteoporos Int. 2007;18:93–9.
Rourke KM, Brehm BJ, Cassell C, Sethuraman G. Effect of weight change on bone mass in female adolescents. J Am Diet Assoc. 2003;103:369–72.
Kanis JA. Textbook of osteoporosis. Oxford: Blackwell Science; 1996. p. 106.
Uenishi K. Calcium absorption rate according to foods and food groups. Clin Calcium. 1996;6:1235–8.
Cadogan J, Eastell R, Jones N, Barker ME. Milk intake and bone mineral acquisition in adolescent girls: randomised, controlled intervention trial. BMJ. 1997;315:1255–60.
Xueqin D, Kun Z, Angelika T, Qian Z, Guansheng M, Xiaoqi H, et al. School-milk intervention trial enhances growth and bone mineral accretion in Chinese girls aged 10–12 years in Beijing. Br J Nutr. 2004;92:159–68.
Acknowledgments
This study was supported by a 2003–2004 Grant-in-Aid for Scientific Research (Grant-in-Aid for Exploratory Research 15659138) from the Japanese Ministry of Education, Culture, Sports, Science, and Technology, the Japanese Society for the Promotion of Science, and a 2005 Seeds Development Research Grant from the Japan Science and Technology Agency.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nakagi, Y., Ito, T., Hirooka, K. et al. Association between lifestyle habits and bone mineral density in Japanese juveniles. Environ Health Prev Med 15, 222–228 (2010). https://doi.org/10.1007/s12199-009-0131-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12199-009-0131-8