
Abstract
Objective
To identify the major causes of death in Down Syndrome (DS), the ages at which mortality rates are the highest and recognize factors associated with it.
Methods
The prospective cohort-based study was carried out in a tertiary health care center. Children with DS (n = 543) counseled at the Center of Medical Genetics, Sir Ganga Ram Hospital from 2005 through 2009 were followed up in year 2010. Survival curves and Cox’s proportional hazards regression analysis were used to determine the effect of different variables on survival.
Results
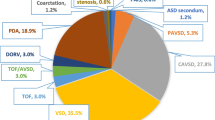
Total mortality was 13 %, of which 80.3 % was in children less than 2 y of age. Presence of congenital heart disease (CHD) increased the risk of mortality by 5.7 folds (p = 0.001). A definitive survival benefit after cardiac intervention was noted, although it differed with the type of CHD. Sex, maternal age at time of birth and karyotypes did not show a significant correlation with survival.
Conclusions
The higher DS infant mortality observed in the present study could be attributed to financial constraints of the families and misconceptions amongst health professionals. It is recommended that a nation-wide DS registry be created to study the morbidity and mortality in Down syndrome from birth. The findings of this study will help clinicians in making management decisions and enable better counseling.

Similar content being viewed by others


References
Patel ZM, Adhia RA. Birth defects surveillance study. Indian J Pediatr. 2005;72:489–91.
Verma IC. Genetic causes of mental retardation in India. In: Hicks EK, Berg JM, eds. The genetics of mental retardation. Dordrecht, Boston: Kluwer Academic Publishers; 1988. pp. 99–106.
Sureshbabu R, Kumari R, Ranugha S, Sathyamoorthy R, Udayashankar C, Oudeacoumar P. Phenotypic and dermatological manifestations in Down Syndrome. Dermatol Online J. 2011;17:3.
Arya R, Kabra M, Gulati S. Epilepsy in children with Down syndrome. Epileptic Disord. 2011;13:1–7.
Bhattacharyya R, Sanyal D, Roy K, Bhattacharyya S. Correlation between physical anomaly and behavioral abnormalities in Down syndrome. J Pediatr Neurosci. 2010;5:105–10.
Asokan S, Muthu MS, Sivakumar N. Oral findings of Down syndrome children in Chennai city, India. Indian J Dent Res. 2008;19:230–5.
Awasthi A, Das R, Varma N, et al. Hematological disorders in Down syndrome: ten-year experience at a Tertiary Care Center in North India. Pediatr Hematol Oncol. 2005;22:507–12.
Kava MP, Tullu MS, Muranjan MN, Girisha KM. Down syndrome: clinical profile from India. Arch Med Res. 2004;35:31–5.
Irving C, Basu A, Richmond S, Burn J, Wren C. Twenty-year trends in prevalence and survival of Down Syndrome. Eur J Hum Genet. 2008;16:1336–40.
Glasson EJ, Sullivan SG, Hussain R, Petterson BA, Montgomery PD, Bittles AH. Comparative survival advantage of males with Down’s syndrome. Am J Hum Biol. 2003;15:192–5.
Stos B, Dembour G, Ovaert C, et al. Risks and benefits of cardiac surgery in Down’s syndrome with congenital heart disease. Arch Pediatr. 2004;11:1197–201.
Frid C, Drott P, Lundell B, Rasmussen F, Annerén G. Mortality in Down’s syndrome in relation to congenital malformations. J Intellect Disabil Res. 2001;43:234–41.
Tubman TR, Shields MD, Craig BG, Mulholland HC, Nevin NC. Congenital heart disease in Down’s syndrome: two years prospective early screening study. BMJ. 1991;302:1425–7.
Mikkelsen M, Poulsen H, Nielsen KG. Incidence, survival, and mortality in Down syndrome in Denmark. Am J Med Genet Suppl: Trisomy 21 (Down Syndrome). 1990;37:S75–8.
Bell JA, Pearn JH, Firman D. Childhood deaths in Down’s syndrome. Survival curves and causes of death from a total population study in Queensland, Australia, 1976 to 1985. J Med Genet. 1989;26:764–8.
McGrother CW, Marshall B. Recent trends in incidence, morbidity and survival in Down’s syndrome. J Ment Defic Res. 1990;34:49–57.
Fudge Jr JC, Li S, Jaggers J, et al. Congenital heart surgery outcomes in Down syndrome: analysis of a National Clinical Database. Pediatrics. 2010;126:315–22.
Parvathy U, Balakrishnan KR, Ranjith MS, Saldanha R, Sai S, Vakamudi M. Surgical experience with congenital heart disease in Down’s syndrome. Indian Heart J. 2000;52:438–41.
Kumar AKS, Chen LC, Choudhury M, et al. India: Towards universal health coverage 6- financing health care for all: challenges and opportunities. Lancet. 2011;377:668–77.
Saxena A. Congenital Heart Disease in India: a status report. Indian J Pediatr. 2005;72:595–8.
Census Data (2001) National summary page. http://www.censusindia.gov.in/Census_Data_2001/National_Summary/National_Summary_DataPage.aspx. Last accessed 06/08/2011.
Elwood JH, Darragh PM. Prevalence of mongolism in Northern Ireland. J Ment Defic Res. 1981;25:157–60.
Viola G, Rosano A. Time trend of survival among infants with Down’s syndrome. Ital J Pediatr. 2005;31:254–60.
Acknowledgements
The authors would like to thank Ashish Upadhyay for his assistance with statistical analysis.
Conflict of Interest
None.
Role of Funding Source
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nahar, R., Kotecha, U., Puri, R.D. et al. Survival Analysis of Down Syndrome Cohort in a Tertiary Health Care Center in India. Indian J Pediatr 80, 118–123 (2013). https://doi.org/10.1007/s12098-012-0836-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-012-0836-3