
Abstract
In recent years, robotic assistance for surgical procedures has grown on a worldwide scale, particularly for use in more complex operations. Such operations usually require meticulous handling of tissue, involve a narrow working space and limit the surgeon’s sense of orientation in the human body. Improvement in both tissue handling and working within a narrow working space might be achieved through the use of robotic assistance. Soft tissue navigation might improve orientation by visualizing important target and risk structures intraoperatively, thereby possibly improving patient outcome. Prerequisites for navigation are its integration into the surgical workflow and accurate localization of both the instruments and patient. Magnetic tracking allows for good integration but is susceptible to distortion through metal or electro-magnetic interference, which may be caused by the operation table or a robotic system. We have investigated whether magnetic tracking can be used in combination with the da Vinci® (DV) telemanipulator in terms of stability and precision. We used a common magnetic tracking system (Aurora®, NDI Inc.) with the DV in a typical operation setup. Magnetic field distortion was evaluated using a measuring facility, with the following reference system: without any metal (R), operation table alone (T), DV in standby (D) and DV in motion (Dm). The maximum error of the entire tracking volume for R, T, D and Dm was 9.9, 32.8, 37.9 and 37.2 mm, respectively. Limiting the tracking volume to 190 mm (from cranial to caudal) resulted in a maximum error of 4.0, 8.3, 8.5 and 8.9 mm, respectively. When used in the operation room, magnetic tracking shows high errors, mainly due to the operation table. The target area should be limited to increase accuracy, which is possible for most surgical applications. The use of the da Vinci® telemanipulator only slightly aggravates the distortion and can thus be used in combination with magnetic tracking systems.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The major benefits of laparoscopy for the patient are a reduced need for analgesics, reduced surgical trauma, improved cosmesis and faster recovery [1]. This accounts for the worldwide acceptance of laparoscopy in the clinical setting, with its applications having expanded from simple ablative procedures to more complex operations, such as prostatectomy, gastric bypass and liver and rectal surgery [2–5]. Under these circumstances, the shortcomings of conventional laparoscopy, especially the limited degrees of freedom, two-dimensional view, restricted ergonomics for the surgeon and the lack of the wrist gear, have become more evident [6, 7]. Minimally invasive robotic systems, such as the da Vinci® surgical system (DV) (Intuitive Surgical, Sunnyvale, CA), theoretically provide an ideal approach to address this challenge [6, 7]. However, orientation in a narrow space, the identification and attribution of structures and the estimation of the instrument’s position in relation to the position of risk and target structures remain difficult [8].
A navigation system, similar to those used in neuro- and maxillofacial surgery, might be a possible solution to these problems [11–13]. However, navigation in soft tissue surgery is relatively more complex due to organ deformation and changing organ positions caused by tissue elasticity as well as cardiac and respiratory movements [9]. There is a need for updated information on the position of patient risk and target structures to build a navigation system that shows enough precision and accuracy for soft tissue surgery.
A tracking system is required to assess the spatial position of these structures. The most widely used tracking systems are magnetic and optic systems. While optic tracking systems provide high accuracy and precision, they require a direct line of sight from the sensor to the camera [10]. Their usability, high accuracy and precision in minimally invasive robotic surgery have already been proven [11]. Electromagnetic tracking systems are also highly accurate and precise, and they do not require a direct line of sight. However, they are susceptible to interference from ferromagnetic materials and electromagnetic fields [12]. Since DV effectors and instruments consist of metal, wire ropes and servo motors, its influence on magnetic tracking and its usability in the operating room are not known. The aim of the study reported here was to evaluate whether the DV can be used in combination with an electromagnetic navigation system to provide sufficient accuracy to visualize risk and target structures intraoperatively.
Materials and methods
To evaluate the effect of the DV and the operation table on the NDI Aurora® V1 (NDI Inc, Waterloo, Ontario, Canada) electromagnetic tracking system, here referred to as EMT, a metal-free measuring facility had to be built to minimize other possible sources of interference. In addition, the data acquisition setup was chosen to be as close to the real operation setup as possible to evaluate the usability of the EMT in a realistic environment.
Development of the measuring facility
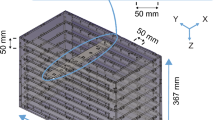
A completely metal-free measuring facility was built to minimize interference with the EMT. This consisted of 12 polyvinyl chloride (PVC) rigid tubes that were arranged in such a way that the DV instruments and camera could be used in between them. The measuring facility walls were built out of medium-density fiberboard (diameter 22 mm). The PVC rigid tubes were 500 mm long and had a wall thickness and inner diameter of 3 and 5 mm, respectively. The pipes were arranged to cover the complete tracking volume of the EMT. The cubic tracking volume featuring a volume of 500 × 500 × 500 mm, according to the manufacturer of the EMT, was chosen due to known increased distortion in the periphery of the alternative dome volume. The pipes (500 mm) were arranged along the x-axis of the EMT volume (Fig. 1). A computed tomography (CT) (512 × 512 pixel, layer thickness 0.6 mm) was performed to generate a digital representation of the measuring facility.

Wooden metal-free measuring facility with 12 polyvinyl chloride (PVC) tubes, thus enabling laparoscopic instruments to be used between the tubes
Tracking system
The EMT was used with one field generator and one sensor. The field generator was a rectangle box that created an electromagnetic field, with a cube size tracking volume of 500 × 500 × 500 mm, according to the manufacturer. The sender was arranged on the right side of the operating table (Fig. 2). The EMT was used in combination with a 5DOF sensor (type Mednetix-5DK) embedded in a flexible cord. The outer diameter of the cord was adjusted to fit the inner diameter of the pipes using Leukosilk® tape.

Realistic setup in the operating room with anesthesia console, laparoscopic turret and the da Vinci surgical system, as used in laparoscopic nissen fundoplication
Setup in the operating room
The DV was arranged in the operating room in the same way a typical operation setup is used for nissen fundoplication, with the DV over the head of the patient. All medical instruments and devices were positioned as if for a regular abdominal operation (Fig. 2) [13]. The operating table used was an Alphamaquet® 1150 (Maquet, Rastatt, Germany) system and consisted of several parts with ferromagnetic characteristics (Fig. 3).

Operating table Alphamaquet 1150, with outlined ferromagnetic material (yellow). EMT Electromagnetic tracking system
Data acquisition and processing
Stable conditions were not expected during navigated surgery. Thus, the sensor was constantly pulled orthogonally to the field generator along the path forced by the PVC tube, simulating the instruments in use. The measurement of distorted positions was achieved by pulling the sensor from one end of the pipe to the other. In this way, the shift in the y- and z-axes of the tracking coordinate space was addressed. The shift in the x-axis was not captured in this setup. A shift was detected if the tracked position left the centerline of the corresponding pipe. The distance between the centerline and the tracked coordinate was used to describe distortion at each point along the x-axis. Two measurements for each tube and setup were acquired by slowly and continuously pulling the sensor through each pipe. We performed seven measurements: a reference measurement without the table, the DV and other metallic objects in close proximity (R), respectively, one with the measuring facility directly on the table (Tl), one with the measuring facility lifted 50 mm (T), one with the DV in active mode but not in motion (D), and one with the DV in motion (Dm) (Fig. 4). The DV measurements were only performed with a 50 mm-lifted measuring facility due to obvious high distortion when the measuring facility was not lifted.

Left Static da Vinci—magnetic sensors were pulled through a PVC tube. Right da Vinci® was constantly in motion using the da Vinci console
For data processing the centerline of each pipe was interactively defined. This was accomplished by processing the CT scan DICOM file of the measuring facility and precisely defining sample points inside each pipe at five equivalent positions, using MITK (Medical Imaging Interaction Toolkit; DKFZ, German Cancer Research Center, Heidelberg, Germany), thereby creating four line segments. Registration between the CT coordinate and tracking coordinate space was done by rigid point-to-point registration. The middle of the tubes were taken for registration. The attribution of each measured track sample to the corresponding line segment was first determined for each x coordinate, and then the offset vector between the matched track sample and the matched line segment in orthogonal direction was calculated. If two measurements were found for the same x coordinate, the larger offset vector was used. To ensure precision, each evaluation setup was also assessed by measuring three fixed positions of each track: head, middle and feet. Orientations were not assessed.
Results
Reference measurements (R) showed low errors (Fig. 5). Accuracy particularly decreased at the periphery of the tracking volume, far from the field generator. In contrast, the tracking system showed low distortion at the center of the tracking volume (Fig. 6).

Reference evaluation shows the virtual three-dimensional (3D) scene by MITK: interactively defined reference centerlines are red, and measured positions with the EMT system at corresponding centerline positions are yellow. The yellow and green lines should always stay close to the red line for high accuracy

Results of the exemplary reference measurements for each separate tube showing the respective maximum distance from the centerline. The y-axis represents the extent of shift (of the tracked position); the x-axis represents the x-coordinate of the tracking volume
The results of the two operation table assessments (Tl, T) showed that the closer the field generator was to the table, the higher the amount of errors. These errors increased dramatically towards the periphery of the tracking volume (Figs. 7, 8).

Measurement without the da Vinci system for all tubes, with the measuring facility lifted 50 mm on the operation table

Overview of the maximal error for all tubes (according to the setup in the x-axis), measured orthogonally to the reference lines
The use of the DV (D, Dm) did not reveal any additional measurable errors, neither in static position nor during motion (Fig. 8).
For all measurements, variance declined from the periphery to the middle of the tracking volume for both the y- and z-axes, although to a lesser extent along the z-axis. Limiting the tracking volume to 190 mm in the craniocaudal direction led to a maximum error of 10 mm. The maximum errors of the entire tracking volume are shown in Table 1.
Discussion
In summary, this study has shown that an EMT can be reliably used with the DV within a real medical environment if the tracking volume is limited. Our results also demonstrate that the DV seems to have had hardly any effect on the accuracy of the magnetic tracking system. In contrast, metallic parts of the operating table distorted the positions delivered by the EMT to a large extent. The result from lifting the measurement setup by 50 mm shows that the EMT was more accurate in areas that were further away from ferromagnetic objects. The largest errors were seen towards the borders of the tracking volume, which can be explained by the decreasing strength of the electromagnetic field the further away it was from the electromagnetic field generator.
In general, detected errors have to be either eliminated or accurately detected in order to ensure precise navigation throughout the tracking volume. Since the amount of errors detected is still fairly high, our results indicate the need for an EMT calibration prior to intervention. This can be done by using the wooden measuring facility presented here as a reference; for example, by logging the coordinates over time and registering them with the virtual description of the wooden measuring facility (centerlines). By means of an iterative closest point algorithm, the best fit can be calculated in order to construct a lookup table for distorted positions and their corresponding correction. The distortion can also be decreased by repositioning the field generator (and the patient) to a position which is less affected by distortion due to ferromagnetic objects. However, this repositioning depends on the intervention performed.
The resulting amount of electromagnetic distortion caused by the operating table can also be decreased by choosing a table with a different material. An operation table constructed with carbon might have less effect on the electromagnetic field of the EMT. Furthermore, it should be noted that the results presented here can be only applied to the EMT tested. We did not evaluate a different Aurora tracking system or a different EMT, but according to theory, similar types of results are expected. NDI Inc. has developed a new type of electromagnetic field generator which resembles a board that can be installed right under the patient directly on top of the operation table. According to the manufacturer, this system shows less distortion due to ferromagnetic material of the operation table, but it has yet to be evaluated with the above-mentioned setup.
Previous work has already shown that navigation is feasible, such as for transhiatal minimally invasive esophagectomy [11]. The biggest challenge of these systems is that they do not provide an intraoperative update of the target position and risk structures. Particularly in esophagectomy, but also in rectal surgery, the iatrogenic manipulation causes a substantial shift of structures. Determining the correct height for the anastomosis in transhiatal esophagectomy or rectal resection requires much surgical experience. To achieve this, EMT sensors could be applied endoscopically in the esophagus and the rectum. Thus, combining the developed system, which is based on optical tracking, with an EMT will enable, for example, the intraoperative update of the position of a tumor in the esophagus or rectum, resulting in higher overall precision. This navigation system could help to find the correct position for anastomosis or affected lymph nodes in esophagectomy, or it could help to distinguish between scar and tumor for tumor recurrence of preoperated rectal cancer.
There are also limitations to this study. To compute the overall volume, we deemed accuracy to be less useful for the EMT because of the strong spatial dependence of its errors. Therefore, we computed the maximum errors which we believe to be clinically more important. Values such as the root mean square deviation have been calculated but are of less use since they involve the entire pipe, whereas here only the positional deviation at certain points of the x-axis was important.
To summarize, a magnetic tracking system can be used reliably in combination with the DV in a limited tracking volume and shows sufficient accuracy for navigation purposes.
References
Li X, Zhang J, Sang L, Zhang W, Chu Z, Liu Y (2010) Laparoscopic versus conventional appendectomy—a meta-analysis of randomized controlled trials. BMC Gastroenterol 10:129. doi:10.1186/1471-230X-10-129
Sauerland S, Angrisani L, Belachew M, Chevallier JM, Favretti F, Finer N, Fingerhut A, Garcia Caballero M, Guisado Macias JA, Mittermair R, Morino M, Msika S, Rubino F, Tacchino R, Weiner R, Neugebauer EA (2005) Obesity surgery: evidence-based guidelines of the European association for endoscopic surgery (EAES). Surg Endosc 19(2):200–221. doi:10.1007/s00464-004-9194-1
Gumbs AA, Tsai TJ, Hoffman JP (2012) Initial experience with laparoscopic hepatic resection at a comprehensive cancer center. Surg Endosc 26:480–487. doi:10.1007/s00464-011-1904-x
Row D, Weiser MR (2010) An update on laparoscopic resection for rectal cancer. Cancer Control 17(1):16–24
Coelho RF, Rocco B, Patel MB, Orvieto MA, Chauhan S, Ficarra V, Melegari S, Palmer KJ, Patel VR (2010) Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a critical review of outcomes reported by high-volume centers. J Endourol 24(12):2003–2015. doi:10.1089/end.2010.0295
Kenngott HG, Muller-Stich BP, Reiter MA, Rassweiler J, Gutt CN (2008) Robotic suturing: technique and benefit in advanced laparoscopic surgery. Minim Invasive Ther Allied Technol 17(3):160–167. doi:10.1080/13645700802103381
Maeso S, Reza M, Mayol JA, Blasco JA, Guerra M, Andradas E, Plana MN (2010) Efficacy of the Da Vinci surgical system in abdominal surgery compared with that of laparoscopy: a systematic review and meta-analysis. Ann Surg 252(2):254–262. doi:10.1097/SLA.0b013e3181e6239e
Antoniou SA, Antoniou GA, Koch OO, Pointner R, Granderath FA (2011) Robot-assisted laparoscopic surgery of the colon and rectum. Surg Endosc. doi:10.1007/s00464-011-1867-y
Baumhauer M, Feuerstein M, Meinzer HP, Rassweiler J (2008) Navigation in endoscopic soft tissue surgery: perspectives and limitations. J Endourol 22(4):751–766. doi:10.1089/end.2007.9827
West JB, Maurer CR Jr (2004) Designing optically tracked instruments for image-guided surgery. IEEE Trans Med Imag 23(5):533–545
Kenngott HG, Neuhaus J, Muller-Stich BP, Wolf I, Vetter M, Meinzer HP, Koninger J, Buchler MW, Gutt CN (2008) Development of a navigation system for minimally invasive esophagectomy. Surg Endosc 22(8):1858–1865. doi:10.1007/s00464-007-9723-9
Frantz DD, Wiles AD, Leis SE, Kirsch SR (2003) Accuracy assessment protocols for electromagnetic tracking systems. Phys Med Biol 48:2241–2251
Muller-Stich BP, Reiter MA, Wente MN, Bintintan VV, Koninger J, Buchler MW, Gutt CN (2007) Robot-assisted versus conventional laparoscopic fundoplication: short-term outcome of a pilot randomized controlled trial. Surg Endosc 21(10):1800–1805. doi:10.1007/s00464-007-9268-y
Acknowledgments
This research project was carried out with the support of the Research Training Group 1126 “Soft-tissue Surgery: New Computer-based Methods for the Future Workplace”, funded by the German Research Foundation.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Kenngott, H.G., Wegner, I., Neuhaus, J. et al. Magnetic tracking in the operation room using the da Vinci® telemanipulator is feasible. J Robotic Surg 7, 59–64 (2013). https://doi.org/10.1007/s11701-012-0347-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-012-0347-2