
Abstract
Purpose
This study aims to determine the incidence, etiology, and management options for symptomatic gastric obstruction caused by axially twisted sleeve gastrectomy.
Methods
In this retrospective study, we reviewed medical charts of all morbidly obese patients who underwent laparoscopic sleeve gastrectomy. Patients who developed gastric obstruction symptoms and were diagnosed with twisted sleeve gastrectomy were identified and included in this study.
Results
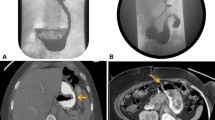
From October 2005 to December 2015, there are 3634 morbidly obese patients who underwent laparoscopic sleeve gastrectomy (LSG). Eighty-six (2.3%) patients developed symptoms of gastric obstruction. Forty-five (1.23%) patients were included in this study. The mean time of presentation was 59.8 days after surgery. Upper GI contrast study was done routinely, and it was positive for axial twist in 37 (82%) patients. Abdominal CT with oral and IV contrast was done in eight (18%) when swallow study was equivocal. Endoscopic treatment was successful in 43 patients (95.5%). Sixteen patients were successfully managed by endoscopic stenting, and 29 patients had balloon dilation. The average numbers of dilation sessions were 1.7. Out of these 29 patients, 18 responded well to a single session of dilatation and did not require any further dilatation sessions. Two patients who failed to respond to three subsequent sessions of balloon dilation underwent laparoscopic adhesiolysis and gastropexy.
Conclusions
Endoscopic stenting is an effective tool in management of axial rotation of sleeved stomach. Balloon dilation can also be effective in selected cases. Few cases might require laparoscopic adhesiolysis and gastropexy.




Similar content being viewed by others


References
Himpens J, Dobbeleir J, Peeters G. Long-term results of laparoscopic sleeve gastrectomy for obesity. Ann Surg. 2010;252:319–24.
Givon-Madhala O, Spector R, Wasserberg N, et al. Technical aspects of laparoscopic sleeve gastrectomy in 25 morbidly obese patients. ObesSurg. 2007;17:722–7.
Gluck B, Movitz B, Jansma S, et al. Laparoscopic sleeve gastrectomy is a safe and effective bariatric procedure for the lower BMI (35.0–43.0 kg/m2) population. Obes Surg. 2011;21(8):1168–71.
Gagner M, Deitel M, Kalberer TL, et al. The second international consensus summit for sleeve gastrectomy, March 19–21, 2009. Surg Obes Rel Dis. 2009;5:476–85.
Frezza E, Reddy S, Gee LL, et al. Complications after sleeve gastrectomy for morbid obesity. ObesSurg. 2009;19:684–7.
Brethauer S, Hammel J, Schauer P. Systematic review of sleeve gastrectomy as staging and primary bariatric procedure. Surg Obes Rel Dis. 2009;5:469–75.
Demaria EJ, Pate V, Warthen M, et al. Baseline data from American society for metabolic and bariatric surgery—designated bariatric surgery centers of excellence using the bariatric outcomes longitudinal database. Surg Obes Rel Dis. 2010;6:347–55.
Bohdjalian A, Langer FB, Shakeri-Leidenmühler S, et al. Sleeve gastrectomy as sole and definitive bariatric procedure: 5-year results for weight loss and ghrelin. ObesSurg. 2010;20:535–40.
Menenakos E, Stamou MK, Albanopoulos K, et al. Laparoscopic sleeve gastrectomy performed with intent to treat morbid obesity: a prospective single-center study of 261 patients with a median follow-up of 1 year. ObesSurg. 2009;20(3):276–82.
Nocca D, Krawczykowsky D, Bomans B, et al. A prospective multicenter study of 163 sleeve gastrectomies: results at 1 and 2 years. ObesSurg. 2008;18:560–5.
Parikh A, Alley JB, Peterson RM, et al. Management options for symptomatic stenosis after laparoscopic vertical sleeve gastrectomy in the morbidly obese. Surg Endosc. 2012;26(3):738–46.
Subhas G, Gupta A, Sabir M, et al. Gastric remnant twist in the immediate post-operative period following laparoscopic sleeve gastrectomy. World J Gastrointest Surg. 2015;7(11):345–8.
Lacy A, Ibarzabal A, Obarzabal A, et al. Revisional surgery after sleeve gastrectomy. Surg Laparosc EndoscPercutan Tech. 2010;20:351–6.
Uglioni B, Wölnerhanssen B, Peters T, et al. Midterm results of primary vs secondary laparoscopic sleeve gastrectomy (LSG) as an isolated operation. ObesSurg. 2009;19:401–6.
de Godoy EP, Coelho D. Gastric sleeve fixation strategy in laparoscopic vertical sleeve gastrectomy. Arq bras Cir dig. 2013;26(Suppl 1):79–82
Del Castillo DD, Sabench Pereferrer F, Hernàndez Gonzàlez M, et al. Gastric volvulus after sleeve gastrectomy for morbid obesity. Surgery. 2013;153(3):431–3.
Murcia CH, Quintero PG, Rabaza J, Gonzalez A. Laparoscopic management of gastric torsion after sleeve gastrectomy. CRSLS.00143. 2014.
Gonzalez AM, Mucia CH, Quintero PG, et al. Treatment of gastric torsion after sleeve gastrectomy. Salt Lake City: SAGES; 2014.
Abd Ellatif ME, Abdallah E, Askar W, et al. Long term predictors of success after laparoscopic sleeve gastrectomy. Int J Surg. 2014;12(5):504–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures in the study were performed in accordance with the Institutional Research Board (IRB) Committee.
Informed Consent
Informed consent was obtained from all individuals who participated in the study.
Rights and permissions
About this article

Cite this article
Abd Ellatif, M.E., Abbas, A., El Nakeeb, A. et al. Management Options for Twisted Gastric Tube after Laparoscopic Sleeve Gastrectomy. OBES SURG 27, 2404–2409 (2017). https://doi.org/10.1007/s11695-017-2649-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-2649-y