
Abstract
Background and Objective
Unauthorized immigrants seldom have access to public health insurance programs such as Medicare Part A, which pays hospitals and other health facilities and is funded through the Medicare Trust Fund.
Design and Main Measures
We tabulated annual and total Trust Fund contributions and withdrawals by unauthorized immigrants (i.e., outlays on their behalf) from 2000 to 2011 using the Current Population Survey and Medical Expenditure Panel Surveys. We estimated when the Trust Fund would be depleted if unauthorized immigrants had neither contributed to it nor withdrawn from it. We estimated Trust Fund surpluses by unauthorized immigrants if 10 % were to become authorized annually over the subsequent 7 years.
Key Results
From 2000 to 2011, unauthorized immigrants contributed $2.2 to $3.8 billion more than they withdrew annually (a total surplus of $35.1 billion). Had unauthorized immigrants neither contributed to nor withdrawn from the Trust Fund during those 11 years, it would become insolvent in 2029—1 year earlier than currently predicted. If 10 % of unauthorized immigrants became authorized annually for the subsequent 7 years, Trust Fund surpluses contributed by unauthorized immigrants would total $45.7 billion.
Conclusions
Unauthorized immigrants have prolonged the life of the Medicare Trust Fund. Policies that curtail the influx of unauthorized immigrants may accelerate the Trust Fund’s depletion.
Similar content being viewed by others


INTRODUCTION
Due to rising health care costs, and increased enrollment driven by baby-boomers, politicians and others have expressed concerns that Medicare may not be sustainable.1,2 Medicare’s revenues are mostly derived from earmarked taxes and general government revenues, with smaller funding streams from beneficiary premiums, state payments, taxes on Social Security benefits, and a few other sources.3 Medicare has two trust funds: the Hospital Insurance Trust Fund (HITF), financed mostly through payroll taxes (and interest on past surpluses), primarily pays for inpatient care. The Supplemental Medical Insurance Trust Fund (SMITF)—which primarily pays for outpatient care—is not actually a trust fund but rather an account that is fully funded annually through enrollee premiums and Congressional appropriations from general revenues.3 Thus, while the SMITF receives yearly appropriations matching anticipated outlays, the HITF depends primarily on payroll tax contributions to cover its outlays; when HITF outlays exceed its revenue, assets accumulated from prior years’ surpluses are used.
Recently, publicity has highlighted large numbers of unaccompanied unauthorized minors crossing the US border with Mexico.4 Public discussion has focused on the economic costs but not benefits of this influx of young immigrants. Some advocate that a path to citizenship should be opened for the 11 million unauthorized immigrants, many of whom lack access to publicly funded services, such as health care.5,6 Even the Affordable Care Act blocks unauthorized immigrants from participating in Medicaid expansions and private health insurance marketplaces.7 Many argue that public funds should not support immigrants whose tax payments may be insufficient to justify access to publicly funded programs.8–10
While public debate and policy are driven by these concerns, data suggest that unauthorized immigrants utilize less health care than US natives, even those enrolled in some public programs.11,12 Only 7.9 % of unauthorized immigrants incur publicly financed health expenditures (averaging $140 per person annually), compared to 30.1 % of US natives (who received $1,385 per person annually).11 While we previously assessed Medicare contributions of foreign-born persons,13 no previous studies have specifically assessed contributions of unauthorized foreign-born persons. Hence, concerns remain that unauthorized immigrants are financially draining the health care system.
We determined HITF contributions and expenditures attributable to authorized persons (citizens and legal immigrants) and unauthorized immigrants between 2000 and 2011. We also estimated the year the HITF would have become insolvent had unauthorized immigrants not contributed to or expended funds during these 11 years.
METHODS
Data Sources
Tax Contributions to Medicare Trust Fund
To determine HITF contributions, we analyzed data for persons of all ages from the 2001–2012 Current Population Survey (CPS) March supplements, which included 201,398 respondents in 2012. The CPS (conducted jointly by the Census Bureau and the Bureau of Labor Statistics) provides detailed income information for civilian non-institutionalized US residents.14 This nationally representative survey includes self-reported income from the previous calendar year, birthplace, and citizenship status.
Medicare Expenditures
Medicare expenditures were determined from the 2000–2011 Medical Expenditure Panel Surveys (MEPS). Like the CPS, the MEPS is a nationally representative survey of US civilian non-institutionalized persons. Conducted by the Agency for Healthcare Research and Quality (AHRQ), it provides detailed health care expenditure information by payment source. We linked data from MEPS to the National Health Interview Survey (NHIS, from which the MEPS sample is drawn) to confirm birthplace and citizenship status. MEPS sample sizes for each year ranged from 21,700 to 37,867 persons for whom nativity and citizenship could be identified. The MEPS and NHIS did not inquire about citizenship prior to 2000.
Calculating Contributions, Expenditures, Surpluses, and Deficits
Contributions to the HITF come primarily from payroll taxes with a small contribution from income taxes levied on the Social Security benefits of higher-income beneficiaries. To calculate payroll contributions to the HITF, we multiplied wage and salary earnings by 2.9 % (the rate of payroll taxes funding Medicare). We used the Social Security Administration’s estimate that 50 % of unauthorized persons earn income on which they do not pay FICA taxes.15 We then added revenue from income taxes on Social Security income. To calculate these income taxes, we used tax rates derived from the Congressional Budget Office’s analysis of the 2005 CPS and Statistics of Income data.16 Our estimates of HITF contributions averaged 92 % (range 88–96 %) of the Trustees' reported contributions.
To calculate HITF expenditures for beneficiaries in Medicare’s fee-for-service program, we summed beneficiaries’ hospitalization expenditures. We added the proportion of home health care expenditures that were financed by the HITF.17 The MEPS does not include skilled nursing facility and hospice expenses; thus, we were unable to estimate these directly from MEPS. Instead, we assumed that the share of these expenditures attributable to unauthorized immigrants was proportional to their share of expenditures for inpatient care, home health care, and Medicare Advantage. We estimated expenditures for those covered under Medicare’s managed care plans (Medicare Advantage) by summing Medicare Advantage plans’ total payments to providers and inflating them by the inverse of the average Medicare Advantage medical loss ratio (obtained from a 2009 survey of 41 major Medicare Advantage plans18), a standard method used to adjust payments for health insurance companies’ overhead. We then determined the proportion of these Medicare Advantage expenditures that were financed by the HITF.17
HITF contribution and expenditure dollar estimates were generated by multiplying each group’s (authorized persons vs. unauthorized immigrants) shares of total contributions/expenditures by the Medicare Trustees’ estimates of total HITF revenues and outlays.19–30 Multiplying each groups’ share of total expenditures by the Medicare Trustees’ estimates of HITF outlays corrected for the known underestimation of Medicare expenditures in MEPS.31 Total net surpluses or deficits for each group were calculated by subtracting that group’s withdrawals from their contributions. CPS data were used for total and authorized persons’ population estimates. We used population estimates of unauthorized immigrants published by Passel and Cohn.32 Passel and Cohn apply a residual methodology to CPS data that subtracts the number of legal immigrants and uses a probabilistic model to assign the remaining foreign-born respondents as unauthorized.
Unauthorized Immigrant Estimates
Federal surveys such as CPS and MEPS/NHIS do not query about unauthorized status, although CPS and NHIS ask about place of birth and citizenship status. Although the Survey of Income and Program Participation (SIPP) contains questions used by others to identify unauthorized persons,33 we used the CPS because of the higher numbers of foreign-born respondents [27,889 (author’s analysis, compared to the SIPP’s 10,53033 in 2008)]. To estimate unauthorized immigrants’ CPS contributions and MEPS expenditures, an imputation procedure modeled after Stimpson et al. (2013) was employed; details are described elsewhere.11 In brief, we developed a multivariate regression model to predict all noncitizen immigrants’ expenditures (or contributions). We then used the model to impute unauthorized immigrants’ expenditures (or contributions) based on differences in demographic, economic, and other characteristics. We used an authoritative source on the size and characteristics of unauthorized immigrants as the basis for the imputation.5
Short-Term Impact of the Path to Citizenship Analysis
To estimate the impact of a path to citizenship over the subsequent 7 years (2012–2019), we projected the proportion of total contributions by, expenditures on behalf of, and number of unauthorized immigrants by fitting regression lines to 2000–2011 data. We used the Medicare Trustees’ projections of total contributions and expenditures34 to tabulate future contributions and expenditures per unauthorized immigrant. We assumed that 10 % of unauthorized immigrants became authorized annually and that newly authorized immigrants paid 10 % more in payroll taxes.35 We assumed that expenditures of the newly authorized would mirror those of the unauthorized because few unauthorized immigrants would reach age 65 and have worked legally for 40 quarters, the two requirements for Medicare eligibility. Finally, we calculated cumulative surpluses by unauthorized immigrants (and those who are legalized) under this scenario and in the absence of a path to citizenship.
Estimating the Date of Insolvency
To determine when the HITF would have become insolvent if unauthorized immigrants had neither contributed to nor utilized it from 2000 to 2011, we estimated HITF’s assets at the end of 2013 (the most recent year for which the total surplus or deficit is known) under this counterfactual scenario.34,36 We then estimated each year’s projected surplus or deficit by projecting total expenditures and income (including both taxable payroll revenue and other income sources) for each year from 2014 to 2030. For 2014–2023, total expenditures and income were based on the Medicare Trustees’ estimates.34 The Trustees have not published expenditure and income projections for later years; however, they have published annual changes in expenditures and taxable payroll in 2025 and 2030.34 For the years 2024–2030, we estimated expenditures by multiplying the prior year’s expenditures by the projected annual expenditure change in 2025 (for 2024–2025) and in 2030 (for 2026–2030). We estimated taxable payroll revenue for these later years by multiplying the prior year’s taxable payroll by the projected annual taxable payroll change in 2025 (for 2024–2025) and 2030 (for 2026–2030). For other sources of income, we determined average yearly changes from 2014 to 2023 by subtracting taxable payroll from total income. We assumed that average annual changes for other sources of income in 2024–2030 were equal to the average annual change in 2021–2023.
HITF assets at the end of each year if unauthorized immigrants had neither contributed to nor utilized the HITF from 2000 to 2011 were estimated by determining the difference between the prior years’ assets and the projected subsidy for that year. When the projected assets fell below zero, we concluded that the HITF would have become insolvent in that year. We used the Medicare Trustee’s intermediate, low, and high cost assumptions to create three estimates for the insolvency date.34
Statistical Analyses
We used chi-square tests for proportions and linear regressions for dollar estimates (including time trends) in order to determine statistical significance. To account for the highly skewed nature of expenditure data, sensitivity analyses using alternate regression modeling strategies as detailed elsewhere13 were performed for some years; these analyses yielded nearly identical results and thus are not reported on further.
The main analyses were conducted using SAS software (version 9.3) with some sensitivity analyses undertaken with STATA 12. This study was exempted from human subjects review by the Cambridge Health Alliance Institutional Review Board.
RESULTS
Contributions, Expenditures and Net Surplus or Deficit by Authorization Status
In 2011, unauthorized immigrants comprised 3.5 % of the US population and made 1.5 % of HITF contributions, or $3.5 billion. They were responsible for none of its expenditures. Thus, in 2011 unauthorized immigrants generated a trust fund surplus of $3.5 billion. In contrast, authorized persons made $225.4 in HITF contributions and were responsible for $256.7 billion expenditures, generating a $31.3 billion net deficit. Unauthorized immigrants generated an average surplus of $316 per capita, while authorized persons generated a deficit of $106 per capita (Fig. 1).

Per capita contributions, expenditures, and net surpluses to the Medicare Hospital Insurance Trust Fund, 2011, authorized persons and unauthorized immigrants. Source: Author’s analysis of data from the 2012 Current Population Survey (CPS) and 2011 Medical Expenditure Panel Survey (MEPS). Note: Confidence intervals not included for unauthorized immigrants because of unavailability of individual-level data. Adapted from Zallman et al. 13, Exhibit 3
Trends over Time
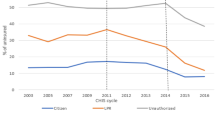
Between 2000 and 2011, unauthorized immigrants’ contributions to the HITF ranged from $2.2 to $3.8 billion (Fig. 2), a total of $35.2 billion. Their net contributions increased slightly over time (p = 0.006). The net contributions of authorized persons declined sharply from a surplus of $33.9 billion to a deficit of $31.3 billion annually (p = 0.006); this generated a total surplus of $67.4 billion between 2000 and 2011.

Net hospital insurance trust fund surplus or deficit attributable to unauthorized immigrants and authorized persons. Source: Author’s analysis of data from the 2001–2012 Current Population Surveys (CPS) and 2000–2011 Medical Expenditure Panel Surveys (MEPS). Adapted from Zallman et al. 13, Exhibit 4
Date of Insolvency
If unauthorized immigrants had not contributed to nor drawn HITF funds from 2000 to 2011, the HITF would become insolvent in 2029—1 year earlier than is currently predicted by Medicare’s Trustees based on their intermediate cost assumptions.3 Under the Trustees’ high cost assumptions, had unauthorized immigrants neither contributed nor withdrawn during 2000 to 2011, the HITF would have become insolvent in 2020, 1 year ahead of the date currently predicted.3 Under the Trustees’ low cost assumptions the trust fund would have accrued surpluses for subsequent years, remaining solvent indefinitely.
Impact of Path to Citizenship
If there were a path to citizenship, unauthorized immigrants and the newly authorized would contribute a cumulative surplus of $45.7 billion, as compared to $44.1billion in the absence of this policy, from 2012 to 2019.
DISCUSSION
Unauthorized immigrants provide a net subsidy to a major health care sector. We find that unauthorized immigrants contributed a net of $3.5 billion to the HITF in 2011 and that their net contributions increased over the prior decade. If unauthorized immigrants had not contributed to the HITF from 2000 to 2011, the HITF would have become insolvent 1 year earlier than predicted. While a prior study documented that immigrants as a whole subsidize Medicare,13 this is the first study to determine the subsidy provided by unauthorized immigrants.
This net subsidy is not surprising given that many unauthorized immigrants contribute to the HITF but none receive benefits. Employers are required to obtain, but not necessarily verify, social security numbers (SSNs) from employees. Unauthorized immigrants often provide (and pay payroll taxes through) SSNs tied to invented names or belonging to another person.37 Less often, unauthorized immigrants pay self-employment taxes (in lieu of payroll taxes) under Individual Tax Identification Numbers (ITINs) allowing them to claim credit for their contributions if they become legalized.38 Regardless of authorization status, many who contribute payroll taxes are unable to access Medicare benefits because they no longer reside in the US; one third of immigrants have returned to their country of origin by 15 years.39
This study has several limitations. Unauthorized immigrants’ HITF contributions may be larger than we estimate, given that unauthorized immigrants may be reluctant to participate in government surveys like the CPS or report their employment out of distrust or fear of deportation. It is difficult to quantify the extent of this possible undercount of their payroll tax contributions. On the expenditure side, this same reluctance might cause unauthorized immigrants to be underrepresented in the MEPS; however, because Medicare participation requires a valid SSN, Medicare expenditures for unauthorized persons are minimal.
Although interest accrues on HITF surpluses from prior years, we credited revenue generated from HITF interest to unauthorized immigrants in proportion to their current tax contributions. Had we credited interest revenue in proportion to past surpluses, our estimates of unauthorized immigrant contributions to the HITF would have increased; hence, our estimates are conservative. On the other hand, we do not have data on unauthorized immigrant contributions to other HITF revenue streams such as general tax revenue and premiums; we assumed that their contributions were proportional to revenue from payroll taxes, an assumption that might overstate their contribution. However, any such overestimation is likely to be small because only a small proportion of HITF revenues come from these other streams (1.4 % from premium contributions and 0.2 % from general tax revenues in 2011).3
In addition, the imputation procedure we used to estimate unauthorized immigrants’ Medicare contributions and expenditures may have limitations, which have been described in other papers that have used this method.11,12,40 However, given the limited availability of reliable data about the legal status of immigrants in large surveys, the imputation method we used appears reasonably reliable. A sensitivity analysis based on the estimated variation in size of the unauthorized population41 suggests that unauthorized immigrants provided a subsidy of between $33.6 and $36.5 billion between 2000 and 2011.
Our method for determining the date of insolvency assumes that unauthorized immigrants contributed to and utilized the HITF for only the 11 years (2000 to 2011) for which specific data on non-citizens were available from the CPS and MEPS. However, unauthorized immigrants almost certainly generated HITF surpluses in most years since Medicare’s implementation in 1966. If so, unauthorized immigrants’ salutary effect on the HITF’s long-term solvency is likely much greater than we estimated.
Our findings raise doubt about the widely held assumption that unauthorized immigrants burden publicly financed health care. While unauthorized immigrants might utilize more public resources than they contribute in some areas, our findings suggest that immigration restrictions based on this assumption may destabilize the public health care financing system, at least for Medicare. Ineligibility for Medicare may cause unauthorized immigrants to seek medical care through other publicly subsidized programs not analyzed in this study—such as uncompensated care and Medicaid. Most states fund emergency and obstetrical care of unauthorized immigrants; 18 states plus the District of Columbia offer prenatal, child, or other health care coverage.42–44 A few provide fully state-funded Medicaid benefits to unauthorized elderly immigrants. While our analysis is limited to the impact on the HITF trust fund, it is important to mention that unauthorized immigrants incur an estimated $5.5 billion in non-Medicare publicly funded health care expenses annually (author’s analysis based on available data5,11,45), mostly funded at the state and local level. However, immigrants also contribute substantially to state and local taxes; in addition to non-FICA state payroll taxes they pay property (they pay rent) and sales taxes; some estimates place the contributions of unauthorized immigrants to state and local taxes at over $10 billion.46
Some have raised ethical objections to denying health care access to individuals on the basis of their legal status. Even apart from these ethical considerations, our findings question these policies on economic and equity grounds.
Policies providing a path to citizenship for currently unauthorized immigrants would have multiple effects on Medicare’s finances. First, they would probably increase the number of immigrants eligible for Medicare and hence increase expenditures on their behalf in the long term. However, such policies would also likely increase payroll tax collections by reducing immigrants’ “off the books” employment and removing barriers that keep them out of jobs that generate higher wages (and payroll taxes). Our analysis of the short-term effects of a path to citizenship suggests that between 2012 and 2019, unauthorized immigrants (including the 10 % who recently became authorized) would provide a cumulative HITF subsidy of $45.7 billion. This would imply that policies that promote legalization, such as President Obama’s 2014 Executive Order on immigration, would not result in decreased net contributions, at least in the short term.
The younger age structure of the unauthorized immigrant population (compared to the age structure of the US-born) is likely to be the most important factor. This implies that a steady flow of healthy young immigrants would counterbalance the health care financing challenge presented by the aging US population and would help sustain Medicare funding for the millions of elderly and disabled Americans who rely on it.
References
Holahan J, McMorrow S. Medicare and Medicaid spending trends and the deficit debate. N Engl J Med. 2012;367:393–5.
Keehan S, et al. Health spending projections through 2017: the baby-boom generation is coming to Medicare. Health Aff. 2008;27(2):w145–55.
The Boards of Trustees Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds, 2013 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2013.
Krogstad J M, Gonzalez-Barrera A. Number of Latino children caught trying to enter U.S. nearly doubles in less than a year. 2014 [accessed 5/8/2015]; Available from: http://www.pewresearch.org/fact-tank/2014/06/10/number-of-latino-children-caught-trying-to-enter-u-s-nearly-doubles-in-less-than-a-year/.
Passel JS, Cohn D. Statistical Portrait of the Foreign-Born Population in the United States, 2011. Washington, DC: Pew Hispanic Research Center; 2013.
Passel JS, Cohn D, Gonzalez-Barrera A. New Estimate: 11.7 million in 2012 Population Decline of Unauthorized Immigrants Stalls, May Have Reversed. Washington, DC: Pew Hispanic Research Center; 2013.
Capps R, Fix M. Immigration reform: a long road to citizenship and insurance coverage. Health Aff (Millwood). 2013;32(4):639–42.
Camarota SA. Illegal immigrants and HR 3200: estimate of potential costs to taxpayers. Washington (DC): Center for Immigration Studies; 2009.
Edwards JR. The Medicaid costs of legalizing illegal aliens. Washington (DC): Center for Immigration Studies; 2010.
Martin J. Deterring illegal immigrant settlement: a guide to state and local action, 2nd edn. Washington, DC: Federation for American Immigration.
Stimpson JP, Wilson FA, Su D. Unauthorized immigrants spend less than other immigrants and US natives on health care. Health Aff (Millwood). 2013;32(7):1313–8.
Stimpson JP, Wilson FA, Zallman L. ED visits and spending by unauthorized immigrants compared with legal immigrants and US natives. Am J Emerg Med. 2014;32(6):679–80.
Zallman L, et al. Immigrants contributed an estimated $115.2 billion more to the Medicare Trust Fund than they took out in 2002–09. Health Aff (Millwood). 32(6): 1153–60.
United States Census Bureau. Current Population Survey (CPS): Methodology. [accessed 5/8/2015]. Available from: http://www.census.gov/cps/methodology/.
Goss S, et al. Effects of unauthorized immigration on the actuarial status of the social security trust funds. Actuarial Note Number 151. April 2013, Office of the Chief Actuary.
Scott C, Mulvey J. Social Security: Calculation and History of Taxing Benefits. January 15, 2010 [cited 5/8/2015]; Available from: http://congressionalresearch.com/RL32552/document.php.
Deputy Director Medicare and Medicaid Cost Estimates Group Office of the Actuary CMS, Medicare: Estimated Hospital Insurance Disbursements Calendar Years 1966–2012.
United States House of Representatives Committee on Energy and Commerce Majority Staff, Profits, Marketing and Corporate Expenses in the Medicare Advantage Market. 2009.
The Boards of Trustees Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds, 2001 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2001.
The Boards of Trustees Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds, 2002 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2002.
The Boards of Trustees Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds, 2003 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2003.
The Boards of Trustees Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds, 2004 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2004.
The Boards of Trustees Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds, 2005 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2005.
The Boards of Trustees Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds, 2006 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2006.
The Boards of Trustees Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds, 2007 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds. 2007.
The Boards of Trustees Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds, 2008 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds. 2008.
The Boards of Trustees Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds, 2009 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds. 2009.
The Boards of Trustees Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds, 2010 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds. 2010.
The Boards of Trustees Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds, 2011 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds. 2011.
The Boards of Trustees Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds, 2012 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplemetary Medical Insurance Trust Funds. 2012.
Zuvekas SH, Olin GL. Accuracy of Medicare expenditures in the medical expenditure panel survey. Inquiry. 2009;46(1):92–108.
Passel JS, Cohn D. Unauthorized Immigrants: 11.1 Million in 2011. [accessed 5/8/2015]; Available from: http://www.pewhispanic.org/2012/12/06/unauthorized-immigrants-11-1-million-in-2011/.
Capps R, et al. A Demographic, Socioeconomic, and Health Coverage Profile of Unauthorized Immigrants in the United States. Migration Policy Institute; 2013.
The Boards of Trustees Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds, 2014 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2014.
The Executive Office of the President. Fixing Our Broken Immigration System: The Economic Benefits of Providing a Path to Earned Citizenship. 2013 [accessed 5/8/2015]; Available from: http://www.whitehouse.gov/sites/default/files/our-broken-immigration-system-august-2013.pdf.
Zallman L. Staying Covered: How Immigrants Have Prolonged the Solvency of One of Medicare’s Key Trust Funds and Subsidized Care for U.S. Seniors. 2014 [accessed 5/8/2015]; Available from: http://www.renewoureconomy.org/research/staying-covered-immigrants-prolonged-solvency-one-medicares-key-trust-funds-subsidized-care-u-s-seniors/.
Goss SC. Letter to the Honorable Richard J. Durbin. Washington, DC: Social Security Administration Office of the Chief Actuary; 2007.
Immigration Policy Center. The Facts About the Individual Tax Identification Number (ITIN): An ITIN is NOT an Immigration Benefit. June 2009 [accessed 5/8/2015]; Available from: http://www.immigrationpolicy.org/sites/default/files/docs/ITIN%20fact%20sheet%20063009.pdf.
Van Hook J, Zhang W. Who stays? Who goes? Selective emigration among the foreign-born. Popul Res Policy Rev. 2011;30:1–24.
Zuckerman S, Waidmann, T A, Lawton E. Undocumented immigrants, left out of health reform, likely to continue to grow as share of the uninsured. Health Aff (Millwood). 30(10): 1997–2004.
Passel JS, Cohn D. Unauthorized Immigrant Population: National and State Trends, 2010. Washington, DC: Pew Research Center; 2011.
State Immigration Legislation: A Resource Page. [accessed 5/8/2015]; Available from: http://immigrationpolicy.org/just-facts/state-immigration-legislation-resource-page
National Council of State Legislatures Immigration Policy Project. 2013 Immigration Report. [accessed 5/8/2015]; Available from: http://www.ncsl.org/research/immigration/2013-immigration-report.aspx.
Fortuny A, Chaudry K. A Comprehensive Review of Immigrant Access to Health and Human Services. Urban Institute; 2011.
Hadley J, et al. Covering the uninsured in 2008: current costs, sources of payment, and incremental costs. Health Aff. 2008;27(5):399–415.
Insitute on Taxation and Economic Policy. Undocumented Immigrants’ State and Local Tax Contributions. 2013 [accessed 5/8/2015]; Available from: http://www.itep.org/pdf/undocumentedtaxes.pdf.
Conflict of interest
All authors declare that they do not have a conflict of interest.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Zallman, L., Wilson, F.A., Stimpson, J.P. et al. Unauthorized Immigrants Prolong the Life of Medicare’s Trust Fund. J GEN INTERN MED 31, 122–127 (2016). https://doi.org/10.1007/s11606-015-3418-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-015-3418-z