
Abstract
Background
CKD patients referred to a renal management clinic are looked after by a multidisciplinary team whose care may improve outcome and delay the progression of kidney disease. This paper describes our experience and the results obtained in 940 patients with CKD stage 4 and 5 patients from two renal management clinics (RMC).
Subjects and methods
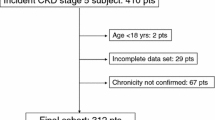
We collected and analyzed the data from 940 patients with CKD stage 4 and 5 at the RMCs of the Toronto General Hospital (TGH), University Health Network and The Scarborough General Hospital (TSH) from January 2000 to November 2007. Inclusion criteria for the study required at least three measurements of serum creatinine over a minimum follow-up of 6 months. We calculated the change of slope of the estimated GFR by linear regression analysis. The slopes were further subdivided into five groups: improved eGFR (eGFR slope ≥+5 ml/min/year); mild improvement (slope >+1 to <+5 ml/min/year); stable (slope <+1 to >−1 ml/min/year); slow progression (i.e., deterioration; slope <−1 to >−5 ml/min/year) and rapid progression (slope >−5 ml/min/year).
Results
During a median follow-up of 1.57 year (range 0.5–8.7 year) of stage 4 patients, eGFR improved in 10.6%, showed mild improvement in 24.2%, was stable in 27.5%, showed slow progression in 28.8% and rapid progression in 8.9% of patients. During a median follow-up of 1.4 year (range 0.5–8 year) of CKD stage 5 patients, eGFR improved in only 1.3%, showed mild improvement in 4.3%, remained stable in 35.6%; showed slow progression in 19.7% and rapid progression in 39.1%. Between the two hospitals (TGH and TSH) there was a statistically significant difference in the number of visits per year for CKD stage 4 patients during the first, second and third year. However, the number of visits per year had no effect on the rate of decline. On univariate analysis, factors predicting non-progression in eGFR slope were eGFR at referral, the use of ACE inhibitors-ARBs and absence of cardiovascular disease. However, in logistic multivariate regression analysis, after adjusting for confounding factors only the eGFR at referral and ACE inhibitors-ARBs were independent factors for non-progression in eGFR.
Summary and conclusions
A significant percentage of CKD stage 4 patients attending a renal management clinic (RMC) showed non-progression or improvement in their kidney function. Although only few stage 5 CKD patients had improvement in their eGFR, 32% of them maintained their eGFR on conservative treatment for over 2 years delaying the initiation of dialysis.

Similar content being viewed by others


References
Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS (2003) Prevalence of chronic kidney disease and decreased kidney function in the adult us population: third national health and nutrition examination survey. Am J Kid Dis 41:1–12
De Vecchi AF, Dratwa M, Wiedermann ME (1999) Healthcare systems and ESRD therapies–an international review. Costs and reimbursement/funding of ESRD therapies. Nephrol Dial Transplant 14(Suppl 6):31–41
Zhou XJ, Saxena R, Liu ZH, Vaziri ND, Silva FG (2008) Renal senescence in 2008: progress and challenges. Int Uro Nephrol 40:823–839
United States Renal Data System (USRDS) (2003) USRDS annual report: incidence and prevalence of ESRD. Am J Kid Dis 42(Suppl 5):1–230
K/DOQI clinical practice guidelines for chronic kidney disease (2002) Evaluation classification and stratification kidney disease outcomes quality initiative. Am J Kid Dis 39(Suppl 2):S7–S246
Jones C, Roderick P, Harris S, Rogerson M (2006) Decline in kidney function before and after nephrology referral and the effect on survival in moderate to advanced chronic kidney disease. Nephrol Dial Transplant 21:2133–2143
Van Biesen W, Vanholder R, Veys N, Verbeke F, Delanghe J, De Bacquer D et al (2006) The importance of standardization of creatinine in the implementation of guidelines and recommendations for CKD: implications for CKD management programmes. Nephrol Dial Transplant 21(1):77–83 Epub 2005 Oct 12
Taskapan H, Tam P, Au V, Chow S, Fung J, Nagai G et al (2008) Improvement in eGFR in patients with chronic kidney disease attending a nephrology clinic. Int Urol Nephrol Epub 40:841–848. doi:10.1007/s11255-008-9360-9
Mendelssohn DC, Toffelmire EB, Levin A (2006) Attitudes of Canadian nephrologists towards multidisciplinary team-based CKD clinic care. Am J Kidney Dis 47:277–284
Levin A, Djurdjev O, Beaulieu M, Er L (2008) Variability and risk factors for kidney disease progression and death following attainment of stage 4 CKD in a referred cohort. Am J Kidney Dis 52(4):661–671
Lindeman RD (2007) Hypertension and kidney protection in the elderly: what is the evidence in 2007? Int Urol Nephrol 39:669–678
Johnson ES, Thorp ML, Platt RW, Smith DH (2008) Predicting the risk of dialysis and transplant among patients with CKD: a retrospective cohort study. Am J Kidney Dis 52:653–660 Epub 2008 Jun 30
Pohl MA, Blumenthal S, Cordonnier DJ, De Alvaro F, Deferrari G, Eisner G et al (2005) Independent and additive impact of blood pressure control and angiotensin II receptor blockade on renal outcomes in the Irbesartan diabetic nephropathy trial: clinical implications and limitations. J Am Soc Nephrol 16:3027–3037
Covic A, Gusbeth-Tatomir P, Goldsmith DJ (2007) Current dilemmas in inhibiting the renin-angiotensin system: do not forget real life. Int Urol Nephrol 39:571–576
Hou FF, Zhang X, Zhang GH, Xie D, Chen PY, Zhang WR et al (2006) Efficacy and safety of benazepril for advanced chronic renal insufficiency. N Engl J Med 354(2):131–140
Tseng CL, Elizabeth FOK, Miller DR, Tiwari A, Maney M, Rajan M, Pogach L (2008) Survival benefit of nephrologic care in patients with diabetes mellitus and chronic kidney disease. Arch Intern Med 168(1):55–62
Tattersall J, Martin-Malo A, Pedrini L, Basci A, Canaud B, Fouque D et al (2007) EBPG guideline on dialysis strategies. Nephrol Dial Trans 22(2):5–21
Fouque D, Guebre-Egziabher F (2007) An update on nutrition in chronic kidney disease. Int Uro Nephrol 39:239–246
Ersoy FF (2007) Osteoporosis in the elderly with chronic kidney disease. Int Uro Nephrol 39:321–331
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhang, AH., Tam, P., LeBlanc, D. et al. Natural history of CKD stage 4 and 5 patients following referral to renal management clinic. Int Urol Nephrol 41, 977–982 (2009). https://doi.org/10.1007/s11255-009-9604-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-009-9604-3