
Abstract
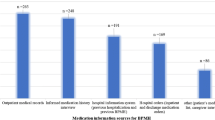
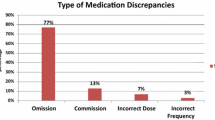
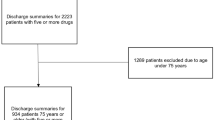
Background Care transitions are risk points for medication discrepancies, especially in the elderly. Objective This study was undertaken to assess prevalence and describe medication reconciliation errors during admission in elderly patients and to analyze associated risk factors. We also evaluate the effect of these errors on the length of hospital stay. Setting General surgery, orthopedics, internal medicines and infectious diseases departments of a 1070-bed Spanish teaching hospital. Method This is a prospective observational study. Patients >65 years and taking ≥5 medications were randomly selected from those admitted to hospital. The pharmacist obtained the best possible medication history based on medical records, medical notes from patients’ previous admissions to hospital, “brown bag” review, community care prescriptions, and comprehensive patient interviews. It was compared to current inpatient prescription to detect unintentional discrepancies (discrepancy with no apparent clinical explanation), which were reported to the physician. When the physician accepted the discrepancy by changing the medication order, it was recorded as a medication reconciliation error and classified by type of error. Several variables were analyzed as possible risk/protective factors. Main outcome measure Is prevalence of medication reconciliation errors at admission. Results Reconciliation was performed on 206 patients. Medication reconciliation errors occurred in 49.5 % (102/206) of patients. 1996 medications were recorded, and 359 had unintentional discrepancies (56.0 % (201/359) medication reconciliation errors). The most common was omission (65.1 %). Identified risk factors were as follows: physician experience, number of pre-admission prescribed medications, and previous surgeries. Computerized order entry system was a protective factor. Conclusion Medication reconciliation errors occur in almost half of the elderly patients at admission, especially omissions. Risk factors were a larger number of previous medications, less physician years of experience, and more previous surgeries. Having a computerized order entry system in the hospital protected against some errors.

Similar content being viewed by others
References
Rozich J, Resar R. Medication safety: one organization’s approach to the challenge. Qual Manag Health Care. 2001;8:27–34.
Using Medication Reconciliation to prevent error. Joint Commission Sentinel Alert, Issue 35 (25 Jan 2006). http://www.jointcommission.org/sentinel_event_alert_issue_35_using_medication_reconciliation_to_prevent_errors/. Accessed 13 Nov 2015.
World Health organization: High 5s: Action on patient safety. standard operating protocol fact sheet: medication reconciliation. 2006. http://www.who.int/patientsafety/implementation/solutions/high5s/ps_medication_reconcili ation_fs_2010_en.pdf. Accessed 15 April 2015.
Mueller SK, Sponsler KC, Kripalani S, Schnipper JL. Hospital-based medication reconciliation practices: a systematic review. Arch Intern Med. 2012;172:1057–69.
Redmond P, Grimes T, McDonnell R, Boland F, Hughes C, Fahey T. Tackling transitions in patient care: the process of medication reconciliation. Fam Pract. 2013;30(5):483–4.
Kennelty KA, Chewning B, Wise M, Kind A, Roberts T. Kreling D Barriers and facilitators of medication reconciliation processes for recently discharged patients from community pharmacists’ perspectives. Res Social Adm Pharm. 2015;11(4):517–30.
Cumbler E, Wald H, Kutner J. Lack of patient knowledge regarding hospital medications. J Hosp Med. 2010;5(2):83–6.
Kaboli PJ, Fernandes O. Medication reconciliation: moving forward. Arch Intern Med. 2012;172(14):1069–70.
Kwan JL, Lo L, Sampson M, Shojania KG. Medication reconciliation during transitions of care as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158:397–403.
Rodríguez Vargas Silveira B, Delgado E, Bermejo Vicedo T. Estudio prospectivo de conciliación de la medicación al ingreso hospitalario. Aten Farm. 2011;13(5):272–8.
Roure Nuez C, Aznar Saliente T, Delgado Sánchez O, Fuster L, Villar I. Consensus document on terminology and classification of programs medication reconciliation. Mayo ed. Barcelona: Spanish Society of Hospital Pharmacy; 2009.
Institute for Safe Medication Practices: ISMP’s List of High-Alert Medications in acute care sites. http://www.ismp.org/tools/highalertmedications.pdf. Accessed 20 May 2015.
World Health Organization: ATC/DDD index. http://www.whocc.no/atc_ddd_index/. Accessed 25 April 2013.
National Coordinating Council for Medication Error Reporting and Prevention: Medication Error Index, 1996. [update 20 Feb 2001]. http://www.nccmerp.org/types-medication-errors. Accessed 20 May 2013.
Delgado O, Nicolás J, Martínez I, Serrano Fabiá A, Anoz Jiménez L, Fernández Cortés F. Reconciliation errors at admission and departure in old and polymedicated patients. Prospective, multicenter randomized study. Med Clin. 2009;133:741–4.
Vasileff HM, Whitten LE, Pink JA, Goldsworthy SJ, Angley MT. The effect on medication errors of pharmacists charting medication in an emergency department. Pharm World Sci. 2009;31:373–9.
van den Bemt PM, van der Schrieck-de Loos EM, van der Linden C, Theeuwes AM, Pol AG. Dutch CBO WHO High 5 s Study Group. Effect of medication reconciliation on unintentional medication discrepancies in acute hospital admissions of elderly adults: a multicenter study. J Am Geriatr Soc. 2013;61(8):1262–8.
Rentero L, Iniesta C, Urbieta E, Madrigal M, Pérez MD. Causas y factores asociados a los errores de conciliación en servicios médicos y quirúrgicos. Farm Hosp. 2014;38(5):398–404.
García Ramos SE. Santolaya Perrin R Medication reconciliation at hospital admission. Aten Farm. 2012;14:7–17.
Unroe KT, Pfeiffenberger T, Riegelhaupt S, et al. Inpatient medication reconciliation at admission and discharge: a retrospective cohort study of age and other risk factors for medication discrepancies. Am J Geriatr Pharmacother. 2010;8:115–26.
Manias E, Gerdtz MF, Weiland TJ, Collins M. Medication use across transition points from the emergency department: identifying factors associated with medication discrepancies. Ann Pharmacother. 2009;43:1755–64.
Buckley MS, Harinstein LM, Clark KB, Smithburger PL, Eckhardt DJ, Alexander E, et al. Impact of a clinical pharmacy admission medication reconciliation program on medication errors in “high-risk” patients. Ann Pharmacother. 2013;47:1599–610.
Reeder TA, Mutnick A. Pharmacist- versus physician-obtained medication histories. Am J Health Syst Pharm. 2008;65:857–60.
Zoni AC, Durán-García ME, Jiménez-Muñoz AB, Salomón Pérez R, Martin P, Herranz Alonso A. The impact of medication reconciliation program at admission in an internal medicine department. Eur J Intern Med. 2012;23:696–700.
Kemp LO, Narula P, McPherson ML, Zuckerman I. Medication reconciliation in hospice: a pilot study. Am J Hosp Palliat Care. 2009;26:193–9.
Kern LM, Wilcox A, Shapiro J, Dhopeshwarkar RV, Kaushal R. Which components of health information technology will drive financial value? Am J Manag Care. 2012;18:438–45.
Chan AH, Garratt E, Lawrence B, Turnbull N, Pratapsingh P. Black PN Effect of education on the recording of medicines on admission to hospital. J Gen Intern Med. 2010;25:537–42.
Andreoli L, Alexandra JF, Tesmoingt C, Eerdekens C, Macrez A, Papo T, et al. Medication reconciliation: a prospective study in an internal medicine unit. Drugs Aging. 2014;31(5):387–93.
Garrido-Garrido EM, García-Garrido I, García-López-Durán JC, García-Jiménez F, Ortega-López I, Bueno-Cavanillas A. Study of polymedicated patients over 65 years-old in an urban primary care centre. Rev Calid Asist. 2011;26:90–6.
Gleason KM, McDaniel MR, Feinglass J, Baker DW, Lindquist L, Liss D, et al. Results of the medications at transitions and clinical handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25:441–7.
Buurman BM, Hoogerduijn JG, de Haan RJ, Abu-Hanna A, Lagaay AM, Verhaar HJ, et al. Geriatric conditions in acutely hospitalized older patients: prevalence and one-year survival and functional decline. PLoS One. 2011;6(11):e26951.
Pippins JR, Gandhi TK, Hamann C, Ndumele CD, Labonville SA, Diedrichsen EK, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23:1414–22.
Shulman R, Singer M, Goldstone J, Bellingan G. Medication errors: a prospective cohort study of hand-written and computerised physician order entry in the intensive care unit. Crit Care. 2005;9:516–21.
Koppel R, Metlay JP, Cohen A, Abaluck B, Localio AR, Kimmel SE, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293(10):1197–203.
Lee JY, Leblanc K, Fernandes OA, Huh JH, Wong GG, Hamandi B, et al. Medication reconciliation during internal hospital transfer and impact of computerized prescriber order entry. Ann Pharmacother. 2010;44:1887–95.
Lesselroth BJ, Felder RS, Adams SM, Cauthers PD, Dorr DA, Wong GJ, et al. Design and implementation of a medication reconciliation kiosk: the Automated Patient History Intake Device (APHID). J Am Med Inform Assoc. 2009;16(3):300–4.
Osorio SN, Abramson E, Pfoh ER, Edwards A, Schottel H, Kaushal R. Risk factors for unexplained medication discrepancies during transitions in care. Fam Med. 2014;46(8):587–96.
Mekonnen AB, McLachlan AJ, Brien JA. Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: a systematic review and meta-analysis. BMJ Open. 2016;6(2):e010003.
Acknowledgments
We would like to thank Justino Rodríguez Vargas, patients, caregivers, physicians, nurses, and pharmacists of the Ramon y Cajal University Health Centre for their collaboration to this study.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Rodríguez Vargas, B., Delgado Silveira, E., Iglesias Peinado, I. et al. Prevalence and risk factors for medication reconciliation errors during hospital admission in elderly patients. Int J Clin Pharm 38, 1164–1171 (2016). https://doi.org/10.1007/s11096-016-0348-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-016-0348-8