
Abstract
Background
IgA nephropathy (IgAN) is a chronic glomerular disease that causes end-stage renal disease in 20–40 % of patients within 20 years. The efficacy of tonsillectomy combined with steroid pulse (SP) administration (TSP) for clinical remission of IgAN has been reported. Particularly in Japan, TSP has been performed widely. However, the optimum method for steroid administration in TSP has not been established.
Methods
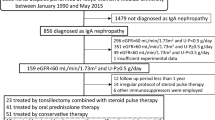
We retrospectively compared clinical remission in IgAN patients treated with tonsillectomy combined with two different steroid administration methods: (1) three courses of SP therapy and oral prednisolone administered on alternate days (group 3A; n = 25); and (2) one course of SP therapy and oral prednisolone administered on consecutive days (group 1C; n = 22).
Results
There was no significant difference in the clinical remission rates between the two groups at 12 (48.0 vs. 40.9 %, P = 0.77) and 24 months after starting treatment (68.0 vs. 72.7 %, P = 0.76) and at the final observation (76.0 vs. 81.8 %, P = 0.73). The mean period from starting treatment to remission of hematuria in group 3A was significantly shorter than that in group 1C (5.7 ± 4.4 vs. 9.9 ± 5.9 months, P = 0.03). Dyslipidemic patients treated for the first time with statin after the SP therapy were more present in group 3A at 24 months (P = 0.02).
Conclusions
In IgAN patients, treatment of group 3A may be effective for inducing rapid remission of hematuria. Further studies are needed to establish an appropriate protocol for TSP.


Similar content being viewed by others


References
Wyatt RJ, Julian BA. IgA nephropathy. N Engl J Med. 2013;368:2402–14.
Koyama A, Igarashi M, Kobayashi M. Natural history and risk factors for immunoglobulin A nephropathy in Japan. Research Group on Progressive Renal Diseases. Am J Kidney Dis. 1997;29:526–32.
Moriyama T, Tanaka K, Iwasaki C, et al. Prognosis in IgA nephropathy: 30-year analysis of 1012 patients at a single center in Japan. PLoS One. 2014;9:e91756.
Pozzi C, Bolasco PG, Fogazzi GB, et al. Corticosteroids in IgA nephropathy: a randomised controlled trial. Lancet. 1999;353:883–7.
Pozzi C, Andrulli S, Del Vecchio L, et al. Corticosteroid effectiveness in IgA nephropathy: long-term results of a randomized, controlled trial. J Am Soc Nephrol. 2004;15:157–63.
Xie Y, Nishi S, Ueno M, et al. The efficacy of tonsillectomy on long-term renal survival in patients with IgA nephropathy. Kidney Int. 2003;63:1861–7.
Hotta O, Miyazaki M, Furuta T, et al. Tonsillectomy and steroid pulse therapy significantly impact on clinical remission in patients with IgA nephropathy. Am J Kidney Dis. 2001;38:736–43.
Miura N, Imai H, Kikuchi S, et al. Tonsillectomy and steroid pulse (TSP) therapy for patients with IgA nephropathy: a nationwide survey of TSP therapy in Japan and an analysis of the predictive factors for resistance to TSP therapy. Clin Exp Nephrol. 2009;13:460–6.
Komatsu H, Fujimoto S, Hara S, Sato Y, Yamada K, Kitamura K. Effect of tonsillectomy plus steroid pulse therapy on clinical remission of IgA nephropathy: a controlled study. Clin J Am Soc Nephrol. 2008;3:1301–7.
Ochi A, Moriyama T, Takei T, Uchida K, Nitta K. Comparison between steroid pulse therapy alone and in combination with tonsillectomy for IgA nephropathy. Int Urol Nephrol. 2013;45:469–76.
Nakagawa N, Kabara M, Matsuki M, et al. Retrospective comparison of the efficacy of tonsillectomy with and without steroid-pulse therapy in IgA nephropathy patients. Intern Med. 2012;51:1323–8.
Kawamura T, Yoshimura M, Miyazaki Y, et al. A multicenter randomized controlled trial of tonsillectomy combined with steroid pulse therapy in patients with immunoglobulin A nephropathy. Nephrol Dial Transplant. 2014;29:1546–53.
Matsuzaki K, Suzuki Y, Nakata J, et al. Nationwide survey on current treatments for IgA nephropathy in Japan. Clin Exp Nephrol. 2013;17:827–33.
Kamei D, Moriyama T, Takei T, Wakai S, Nitta K. Comparison between consecutive and intermittent steroid pulse therapy combined with tonsillectomy for clinical remission of IgA nephropathy. Clin Exp Nephrol. 2014;18:320–8.
Cattran DC, Coppo R, Cook HT, et al. The Oxford classification of IgA nephropathy: rationale, clinicopathological correlations, and classification. Kidney Int. 2009;76:534–45.
Kawamura T, Joh K, Okonogi H, et al. A histologic classification of IgA nephropathy for predicting long-term prognosis: emphasis on end-stage renal disease. J Nephrol. 2013;26:350–7.
Clinical guides for immunoglobulin A (IgA) nephropathy in Japan, third version. Nihon Jinzo Gakkai Shi. 2011;53:123–35.
Matsuo S, Imai E, Horio M, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Suzuki Y, Matsuzaki K, Suzuki H, et al. Proposal of remission criteria for IgA nephropathy. Clin Exp Nephrol. 2013;18:481–6.
Hotta O. Use of corticosteroids, other immunosuppressive therapies, and tonsillectomy in the treatment of IgA nephropathy. Semin Nephrol. 2004;24:244–55.
Moreno JA, Yuste C, Gutiérrez E, et al. Haematuria as a risk factor for chronic kidney disease progression in glomerular diseases: a review. Pediatr Nephrol. 2016;31:523–33.
Gutiérrez E, González E, Hernández E, et al. Factors that determine an incomplete recovery of renal function in macrohematuria-induced acute renal failure of IgA nephropathy. Clin J Am Soc Nephrol. 2007;2:51–7.
Goto M, Wakai K, Kawamura T, Ando M, Endoh M, Tomino Y. A scoring system to predict renal outcome in IgA nephropathy: a nationwide 10-year prospective cohort study. Nephrol Dial Transplant. 2009;24:3068–74.
Yuste C, Rubio-Navarro A, Barraca D, et al. Haematuria increases progression of advanced proteinuric kidney disease. PLoS One. 2015;10:e0128575.
Suzuki Y, Matsuzaki K, Suzuki H, et al. Serum levels of galactose-deficient immunoglobulin (Ig) A1 and related immune complex are associated with disease activity of IgA nephropathy. Clin Exp Nephrol. 2014;18:770–7.
Suzuki H, Kiryluk K, Novak J, et al. The pathophysiology of IgA nephropathy. J Am Soc Nephrol. 2011;22:1795–803.
Tanaka K, Moriyama T, Iwasaki C, Takei T, Nitta K. Effect of hematuria on the outcome of IgA nephropathy with mild proteinuria. Clin Exp Nephrol. 2015;19:815–21.
Coppo R. Is a legacy effect possible in IgA nephropathy? Nephrol Dial Transplant. 2013;28:1657–62.
Szeto CC, Lai FM, To KF, et al. The natural history of immunoglobulin a nephropathy among patients with hematuria and minimal proteinuria. Am J Med. 2001;110:434–7.
Kawaguchi T, Ieiri N, Yamazaki S, et al. Clinical effectiveness of steroid pulse therapy combined with tonsillectomy in patients with immunoglobulin A nephropathy presenting glomerular haematuria and minimal proteinuria. Nephrology (Carlton). 2010;15:116–23.
Barratt J, Feehally J. Treatment of IgA nephropathy. Kidney Int. 2006;69:1934–8.
Tatematsu M, Yasuda Y, Morita Y, et al. Complete remission within 2 years predicts a good prognosis after methylprednisolone pulse therapy in patients with IgA nephropathy. Clin Exp Nephrol. 2012;16:883–91.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
About this article

Cite this article
Watanabe, H., Goto, S., Kondo, D. et al. Comparison of methods of steroid administration combined with tonsillectomy for IgA nephropathy patients. Clin Exp Nephrol 21, 257–265 (2017). https://doi.org/10.1007/s10157-016-1282-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-016-1282-8