
Abstract
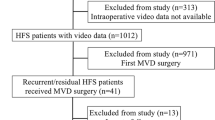
The postoperative course of microvascular decompression (MVD) for hemifacial spasm (HFS) is variable, and the optimal time for assessing the results is unclear. From April 1997 to October 2007, MVD for HFS was performed in 801 patients. Patients were divided into two groups (cured or failed) according to subjective patient assessments over a 3-year period. We analyzed patient characteristics and surgical findings to determine prognostic factors. Medical records were analyzed retrospectively over the 3-year follow-up period. Of the 801 patients who underwent surgery, 743 (92.8 %) appeared to be cured, 70 (8.7 %) had residual or recurrent spasms more than 1 year after surgery, 11 (1.3 %) had gradual improvement over 3 years, and 1 (0.1 %) had delayed improvement more than 3 years after surgery. Fifty-eight patients (7.2 %) had residual or recurrent spasms more than 3 years after surgery, of which 19 (2.4 %) had recurrence after initial relief. The mean time to spasm recurrence was 18.9 months. Intraoperative resolution of the lateral spread response (LSR) after decompression (p = 0.048) and severe indentation (p = 0.038) were significant predictors of good long-term outcome after MVD for HFS. In our series, 70 patients (8.7 %) had residual or recurrent spasms more than 1 year after surgery, of which 12 (17.1 %) improved gradually after 1 year. If the surgeon can confirm intraoperative resolution of the LSR and severe indentation, reoperation can be delayed until 3 years after MVD.

Similar content being viewed by others


References
Park K, Hong SH, Hong SD, Cho YS, Chung WH, Ryu NG (2009) Patterns of hearing loss after microvascular decompression for hemifacial spasm. J Neurol Neurosurg Psychiatry 80:1165–1167
Chung SS, Chang JW, Kim SH, Chang JH, Park YG, Kim DI (2000) Microvascular decompression of the facial nerve for the treatment of hemifacial spasm: preoperative magnetic resonance imaging related to clinical outcomes. Acta Neurochir (Wien) 142:901–906, discussion 907
Gardner JW, Sava GA (1962) Hemifacial spasm: a reversible pathophysiologic state. J Neurosurg 19:240–247
Hyun SJ, Kong DS, Park K (2010) Microvascular decompression for treating hemifacial spasm: lessons learned from a prospective study of 1,174 operations. Neurosurg Rev 33:325–334, discussion 334
Jannetta PJ (1977) Observations on the etiology of trigeminal neuralgia, hemifacial spasm, acoustic nerve dysfunction and glossopharyngeal neuralgia. Definitive microsurgical treatment and results in 117 patients. Neurochirurgia (Stuttg) 20:145–154
Jannetta PJ, Resnick D (1996) Cranial rhizopathies. In: Youmans JR (ed) Neurological surgery: a comprehensive reference guide to the diagnosis and management of neurosurgical problems, 4th edn. Saunders, Philadelphia, pp 3563–3574
Moller AR (1997) Pathophysiology of hemifacial spasm. In: Sindou M, Keravel Y, Moller AR (eds) Hemifacial spasm: a multidisciplinary approach. Springer, New York, pp 51–62
Samii M, Gunther T, Iaconetta G, Muehling M, Vorkapic P, Samii A (2002) Microvascular decompression to treat hemifacial spasm: long-term results for a consecutive series of 143 patients. Neurosurgery 50:712–718, discussion 718-719
Kim HR, Rhee DJ, Kong DS, Park K (2009) Prognostic factors of hemifacial spasm after microvascular decompression. J Korean Neurosurg Soc 45:336–340
Kong DS, Park K, Shin BG, Lee JA, Eum DO (2007) Prognostic value of the lateral spread response for intraoperative electromyography monitoring of the facial musculature during microvascular decompression for hemifacial spasm. J Neurosurg 106:384–387
Park JS, Kong DS, Lee JA, Park K (2008) Hemifacial spasm: neurovascular compressive patterns and surgical significance. Acta Neurochir (Wien) 150:235–241, discussion 241
Hitotsumatsu T, Matsushima T, Inoue T (2003) Microvascular decompression for treatment of trigeminal neuralgia, hemifacial spasm, and glossopharyngeal neuralgia: three surgical approach variations: technical note. Neurosurgery 53:1436–1441, discussion 1442-1433
Park JS, Kong DS, Lee JA, Park K (2007) Intraoperative management to prevent cerebrospinal fluid leakage after microvascular decompression: dural closure with a "plugging muscle" method. Neurosurg Rev 30:139–142, discussion 142
Moller AR, Jannetta PJ (1985) Microvascular decompression in hemifacial spasm: intraoperative electrophysiological observations. Neurosurgery 16:612–618
Li CS (2005) Varied patterns of postoperative course of disappearance of hemifacial spasm after microvascular decompression. Acta Neurochir (Wien) 147:617–620, discussion 620
Sindou M, Keravel Y (2009) Neurosurgical treatment of primary hemifacial spasm with microvascular decompression. Neurochirurgie 55:236–247
Sanders DB (1989) Ephaptic transmission in hemifacial spasm: a single-fiber EMG study. Muscle Nerve 12:690–694
Saito S, Moller AR, Jannetta PJ, Jho HD (1993) Abnormal response from the sternocleidomastoid muscle in patients with spasmodic torticollis: observations during microvascular decompression operations. Acta Neurochir (Wien) 124:92–98
Park JS, Kong DS, Lee JA, Park K (2008) Chronologic analysis of symptomatic change following microvascular decompression for hemifacial spasm: value for predicting midterm outcome. Neurosurg Rev 31:413–418, discussion 418-419
Yamaki T, Hashi K, Niwa J et al (1992) Results of reoperation for failed microvascular decompression. Acta Neurochir (Wien) 115(1–2):1–7
Wilson CB, Yorke C, Prioleau G (1980) Microsurgical vascular decompression for trigeminal neuralgia and hemifacial spasm. West J Med 132:481–487
Park YS, Chang JH, Cho J, Park YG, Chung SS, Chang JW (2006) Reoperation for persistent or recurrent hemifacial spasm after microvascular decompression. Neurosurgery 58:1162–1167, discussion 1162-1167
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Tetsuya Goto, Matsumoto, Japan
The long-term outcome after microvascular decompression (MVD) to treat hemifacial spasm (HFS) was presented from a leading institute. They concluded that the remnant HFS after MVD should be waited for at least 3 years because their results indicated that there was 10 % of residual or recurrent spasms more than 1 year after surgery, of which 20 % of patients improved HFS gradually until 3 years later.
This conclusion should be applied only for well-experienced neurosurgeons of MVD who can be sure of the success of their own procedure. When the residual or recurrent spasms after MVD happens, we must exclude the possibility of inadequate MVD and re-compression by several factors such as shift of the prosthesis or compression by prosthesis itself. Wait-and-follow should be chosen after exclusion of these reasons of residue or recurrence. The postoperative long-standing follow-up improving rate after MVD must be superior to that of the true natural history of HFS, which has not been clarified yet.
Giorgio Iaconetta, Naples, Italy
This report by Jo et al. documents their experience on 801 patients with hemifacial spasm who were treated in 10 years by microvascular decompression.
The paper corroborates the fact that microvascular decompression is the treatment of choice for hemifacial spasm, with 92.8 % of patients free of spasm after surgery. Their results are excellent and analogous to the results reported by my Maestro Prof. Samii (92.3 %). Hearing loss is often the most common complication which occurs frequently after surgical reexploration and if the offending vessel is located in between the VII–VIII cranial nerve complex. Intraoperative monitoring of brain stem evoked potentials is imperative in diminishing the risk of hearing loss. As reported in the paper by an experienced group, this surgical procedure, if perfectly performed, is a low-risk treatment, well-tolerated even by elderly patients, associated to a low recurrence rate, and represents the definitive treatment for more than 90 % of patients. Botulinum toxin and medical therapy should be reserved for patients who are not suitable for surgery.
Makoto Nakamura, Hannover, Germany
Jo et al. present an impressive series of 801 patients, who underwent microvascular decompression (MVD) for hemifacial spasm (HFS) during a time period of 10 years. Surgical results were analyzed retrospectively over a mean follow-up of 64 months.
It is a well-known phenomenon that HFS may persist after successful MVD for several months. In our experience, the majority (>90 %) of patients are spasm-free after 6–12 months.
The authors report an excellent surgical outcome with 743 out of 801 patients (92.8 %) achieving definitive cure after a 3-year follow-up period. However, 11 patients among them showed a gradual improvement of spasm even 1–3 years after surgery. The chance of delayed cure, even up to 3 years after MVD, deserves special consideration.
Most interestingly, the authors found that intraoperative resolution of the lateral spread response (LSR) after decompression and severe indentation were significant predictors of good long-term outcome after MVD for HFS. Based on their retrospective data, they therefore recommend delay of reoperation until 3 years after MVD, when the surgeon was able to confirm intraoperative resolution of the LSR and severe indentation of the root entry zone.
Although the retrospective nature of the study limits the data available for evaluation of long-term outcome, the reported intraoperative observations are important and may help in the decision pro or contra reoperation in residual HFS.
Rights and permissions
About this article
Cite this article
Jo, K.W., Kong, DS. & Park, K. Microvascular decompression for hemifacial spasm: long-term outcome and prognostic factors, with emphasis on delayed cure. Neurosurg Rev 36, 297–302 (2013). https://doi.org/10.1007/s10143-012-0420-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-012-0420-3