
Abstract
Background
Transarterial chemoembolization (TACE) is an important treatment modality for hepatocellular carcinoma (HCC). Accurate identification of feeding arteries and catheterization are necessary for achieving treatment efficacy, especially with selective TACE. However, this often requires multiple imaging studies. We evaluated the utility of a newly developed apparatus that combines multidetector-row computed tomography (MDCT) and angiography (angio-MDCT) to facilitate TACE for treatment of HCC.
Methods
A total of 73 patients who underwent selective TACE with angio-MDCT were compared with 57 patients who had undergone selective TACE with single-row computed tomography assisted by angiography (angio-CT) in terms of the number of imaging studies needed to complete TACE.
Results
The mean number of digital subtraction arteriography (DSA) and CT studies required for characterization of feeding arteries before embolization was 3.53 (range 1–8) and 5.16 (range 2–11), respectively, with single-row angio-CT, and 1.67 (range 1–5) and 2.90 (range 1–5), respectively, with angio-MDCT. Fewer studies were needed in patients who underwent TACE with angio-MDCT (p < 0.0001 for both DSA and CT). Whereas single-row angio-CT failed to identify extrahepatic feeders in three patients (37.5 %), all extrahepatic feeders could be identified with angio-MDCT.
Conclusions
Angio-MDCT facilitates rapid and accurate identification of feeding arteries in patients undergoing TACE through the three-dimensional image analyses by the reconstruction with the workstation.



Similar content being viewed by others

References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90.
Llovet JM, Real MI, Montana X, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359:1734–9.
Inaba Y, Arai Y, Kanematsu M, et al. Revealing hepatic metastases from colorectal cancer: value of combined helical CT during arterial portography and CT hepatic arteriography with a unified CT and angiography system. AJR Am J Roentogenol. 2000;174:955–61.
Takayasu K, Muramatsu Y, Maeda T, et al. Targeted transarterial oily chemoembolization for small foci of hepatocellular carcinoma using a unified helical CT and angiography system: analysis of factors affecting local recurrence and survival rates. AJR Am J Roentogenol. 2001;176:681–8.
Hirota S, Nakano N, Yamamoto S, et al. Cone-beam CT with flat-panel-detector digital angiography system: early experience in abdominal interventional procedures. Cardiovasc Interv Radiol. 2006;29:39–48.
Kakeda S, Korogi Y, Ohnari N, et al. Usefulness of cone-beam volume CT with flat panel detectors in conjunction with catheter angiography for transcatheter arterial embolization. J Vasc Interv Radiol. 2007;18:1508–16.
Iwazawa J, Ohue S, Mitani T, et al. Identifying feeding arteries during TACE of hepatic tumors: comparison of C-arm CT and digital subtraction angiography. AJR Am J Roentgenol. 2009;192:1057–63.
Kothary N, Abdelmaksoud MH, Tognolini A, et al. Imaging guidance with C-arm CT: prospective evaluation of its impact on patient radiation exposure during transhepatic arterial chemoembolization. J Vasc Interv Radiol. 2011;22:1535–43.
Eide KR, Odegard A, Myhre HO, et al. DynaCT during EVAR—a comparison with multidetector CT. Eur J Vasc Endovasc Surg. 2009;37:23–30.
Toyoda H, Kumada T, Sone Y. Impact of a unified CT angiography system on outcome of patients with hepatocellular carcinoma. AJR Am J Roentogenol. 2009;192:766–74.
Fishman EK, Ney DR, Heath DG, et al. Volume rendering versus maximum intensity projection in CT angiography: what works best, when, and why. Radiographics. 2006;26:905–22.
Kokudo N, Makuuchi M. Evidence-based clinical practice guidelines for hepatocellular carcinoma in Japan: J-HCC guidelines. J Gastroenterol. 2009;44:S119–21.
Matsui O, Kadoya M, Suzuki M, et al. Work in progress: dynamic sequential computed tomography during arterial portography in the detection of hepatic neoplasms. Radiology. 1983;146:721–7.
Freeny PC, Marks WM. Computed tomographic arteriography of the liver. Radiology. 1983;148:193–7.
Minamiguchi H, Kawai N, Sato M, et al. Hepatoma feeding arteriogram created by CT during aortography using IVR 64-multidetector-row CT for catheterization in transcatheter arterial chemoembolization for hepatocellular carcinoma. Jpn J Radiol. 2013;31:428–36.
Lee KH, Sung KB, Lee DY, Park SJ, Kim KW, Yu JS. Transcatheter arterial chemoembolization for hepatocellular carcinoma: anatomic and hemodynamic considerations in the hepatic artery and portal vein. Radiographics. 2002;22:1077–91.
Kim HC, Chung JW, Lee W, Jae HJ, Park JH. Recognizing extrahepatic collateral vessels that supply hepatocellular carcinoma to avoid complications of transcatheter arterial chemoembolization. Radiographics. 2005;25:S25–9.
Miyayama S, Matsui O, Taki K, et al. Extrahepatic blood supply to hepatocellular carcinoma: angiographic demonstration and transcatheter arterial chemoembolization. Cardiovasc Interv Radiol. 2006;29:39–48.
Gwon DI, Ko GY, Yoon HK, et al. Inferior phrenic artery: anatomy, variations, pathologic conditions, and interventional management. Radiographics. 2007;27:687–705.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
535_2015_1065_MOESM1_ESM.tiff
Fig. S1 Construction of three-dimensional abdominal vascular and bone images based on computed tomography (CT) aortography using a combined 64-multidetector-row CT and angiography system. Images of bone and organs were first removed from the original image (a, b), and the vascular image was extracted (c). Bone images were then added (d) to facilitate identification of the level of the origin of the feeding artery on the X-ray monitor
535_2015_1065_MOESM2_ESM.tiff
Fig. S2 Changes in the orientation of three-dimensional (3D) vascular images. The orientation of the 3D vascular image can easily be changed to avoid overlap of the target artery with other arteries. CAU caudal view, CRA cranial view, LAO left anterior oblique view, RAO right anterior oblique view
535_2015_1065_MOESM3_ESM.tiff
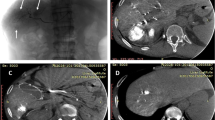
Fig. S3 Identification of the hepatocellular carcinoma (HCC) feeding artery based on three-dimensional (3D) vascular images from a combined 64-multidetector-row computed tomography (CT) and angiography (angio-MDCT) system. The HCC was located in the right lobe of the liver (a, b). It was difficult to identify the feeding artery on two-dimensional digital subtraction angiography (DSA) images (c) because of the lack of clear tumor staining. Analysis of 3D vascular images revealed that the feeding artery branched from left hepatic artery, which was far from the HCC (d). a CT during arterial portography, b CT during hepatic arteriography, c two-dimensional DSA, d 3D vascular image constructed from aortography using angio-MDCT
535_2015_1065_MOESM4_ESM.tiff
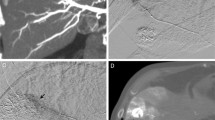
Fig. S4 Identification of the hepatocellular carcinoma (HCC) feeding artery using three-dimensional (3D) vascular images from a combined 64-multidetector-row computed tomography (CT) and angiography system. It was difficult to identify the feeding artery at its origin on two-dimensional digital subtraction angiography (DSA) images (a) or in the frontal view of the 3D vascular image (b) owing to overlap of arteries. Changing the orientation of the 3D vascular image (c) and changing the X-ray monitor view to the 3D vascular image (d) allows the identification and catheterization of the feeding artery. a DSA of the common hepatic artery, b 3D vascular image constructed from CT aortography (frontal view), c 3D vascular image constructed from CT aortography (right oblique view), d DSA of the proximal branch of the feeding artery (views with orientation adjusted on the basis of the 3D vascular image). Red arrow very weak tumor staining on DSA, green arrow enhancement of the HCC on CT
Rights and permissions
About this article

Cite this article
Takada, K., Toyoda, H., Tada, T. et al. Accurate and rapid identification of feeding arteries with multidetector-row angiography-assisted computed tomography for transarterial chemoembolization for hepatocellular carcinoma. J Gastroenterol 50, 1190–1196 (2015). https://doi.org/10.1007/s00535-015-1065-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-015-1065-0