
Abstract
Background
Transient postoperative hypocalcemia is one of the most common complications after thyroidectomy. Permanent hypocalcemia, however, is rare, but usually requires life-long treatment and follow-up. The risk of permanent hypocalcemia has been shown to be significantly higher in patients with Graves’ disease. In the present study we evaluated short-term and long-term changes in serum calcium, phosphate, magnesium, and parathyroid hormone (PTH) levels in order to characterize subjects at risk of postoperative hypoparathyroidism.
Methods
Forty patients who underwent total thyroidectomy for Graves’ disease were included in the study. Calcium, phosphate, magnesium, and PTH were measured before surgery and regularly during the year that followed.
Results
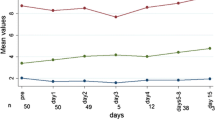
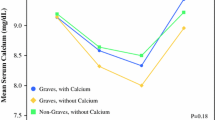
Postoperative hypocalcemia was seen in 21/40 (53 %) patients. Undetectable PTH (<0.6 pmol/L) was registered in 11/40 (27 %) patients. All patients with measurable PTH 6–48 h after operation regained normal calcium. Of those with undetectable PTH after 6–48 h, four developed permanent hypocalcemia. We found a significantly lower serum calcium level before operation in patients who developed permanent hypocalcemia compared to those who did not (p < 0.001). We also found a significant correlation between the decrease in serum magnesium from time 0 to 48 h after operation and permanent hypocalcemia (p = 0.015).
Conclusions
Serum calcium prior to operation, serum PTH, and degree of decrease in magnesium levels in serum 48 h after operation may predict development of permanent hypocalcemia. Magnesium plays an important role in calcium homeostasis via stimulation of PTH secretion and modulation of PTH receptor sensitivity. Both mechanisms may have played a role for the findings reported in this article.



Similar content being viewed by others

References
Pattou F, Combemale F, Fabre S et al (1998) Hypocalcemia following thyroid surgery: incidence and prediction of outcome. World J Surg 22:718–724
Thomusch O, Machens A, Sekulla C et al (2003) The impact of surgical technique on postoperative hypoparathyroidism in bilateral thyroid surgery: a multivariate analysis of 5846 consecutive patients. Surgery 133:180–185
Pfleiderer AG, Ahmad N, Draper MR et al (2009) The timing of calcium measurements in helping to predict temporary and permanent hypocalcaemia in patients having completion and total thyroidectomies. Ann R Coll Surg Engl 91:140–146
Davis RH (1961) Unsuspected partial hypoparathyroidism following thyroidectomy. Proc R Soc Med 54:970–971
Pesce CE, Shiue Z, Tsai HL et al (2010) Postoperative hypocalcemia after thyroidectomy for Graves’ disease. Thyroid 20:1279–1283
Wingert DJ, Friesen SR, Iliopoulos JI et al (1986) Post-thyroidectomy hypocalcemia. Incidence and risk factors. Am J Surg 152:606–610
See AC, Soo KC (1997) Hypocalcaemia following thyroidectomy for thyrotoxicosis. Br J Surg 84:95–97
Kovacevic B, Ignjatovic M, Cuk V et al (2011) Early prediction of symptomatic hypocalcemia after total thyroidectomy. Acta Chir Belg 111:303–307
Harden RM, Harrison MT, Alexander WD et al (1964) Phosphate excretion and parathyroid function in thyrotoxicosis. J Endocrinol 28:281–288
Reeve T, Thompson NW (2000) Complications of thyroid surgery: how to avoid them, how to manage them, and observations on their possible effect on the whole patient. World J Surg 24(8):971–975
Lal G, Ituarte P, Kebebew E et al (2005) Should total thyroidectomy become the preferred procedure for surgical management of Graves’ disease? Thyroid 15:569–574
Wade JS (1965) Three major complications of thyroidectomy. Br J Surg 52:727–731
Bergenfelz A, Jansson S, Kristoffersson A et al (2008) Complications to thyroid surgery: results as reported in a database from a multicenter audit comprising 3,660 patients. Langenbecks Arch Surg 393:667–673
Quinn EM, Neary PM, O’Connor OJ et al (2010) Routine calcium measurement is not necessary after most thyroid surgeries: a prospective clinical study. Clin Otolaryngol 35:468–473
Huang SM, Lee CH, Chou FF et al (2005) Characteristics of thyroidectomy in Taiwan. J Formos Med Assoc 104:6–11
Scurry WC Jr, Beus KS, Hollenbeak CS et al (2005) Perioperative parathyroid hormone assay for diagnosis and management of postthyroidectomy hypocalcemia. Laryngoscope 115:1362–1366
Erbil Y, Bozbora A, Ozbey N et al (2007) Predictive value of age and serum parathormone and vitamin D3 levels for postoperative hypocalcemia after total thyroidectomy for nontoxic multinodular goiter. Arch Surg 142:1182–1187
Amir A, Sands NB, Tamilia M et al (2010) Preoperative serum calcium levels as an indicator of postthyroidectomy hypocalcemia. J Otolaryngol Head Neck Surg 39:654–658
Harrison MT, Harden RM, Alexander WD (1964) Some effects of parathyroid hormone in thyrotoxicosis. J Clin Endocrinol Metab 24:214–217
Samiy AH, Brown JL, Globus DL et al (1960) Interrelation between renal transport systems of magnesium and calcium. Am J Physiol 198:599–602
Coburn JW, Massry SG, Kleeman CR (1970) The effect of calcium infusion on renal handling of magnesium with normal and reduced glomerular filtration rate. Nephron 7:131–143
Allgrove J, Adami S, Fraher L et al (1984) Hypomagnesaemia: studies of parathyroid hormone secretion and function. Clin Endocrinol (Oxf) 21:435–449
Rude RK, Oldham SB, Singer FR (1976) Functional hypoparathyroidism and parathyroid hormone end-organ resistance in human magnesium deficiency. Clin Endocrinol (Oxf) 5:209–224
Rude RK, Oldham SB, Sharp CF Jr et al (1978) Parathyroid hormone secretion in magnesium deficiency. J Clin Endocrinol Metab 47:800–806
Rude RK, Singer FR (1981) Magnesium deficiency and excess. Annu Rev Med 32:245–259
Klein GL, Langman CB, Herndon DN (2000) Persistent hypoparathyroidism following magnesium repletion in burn-injured children. Pediatr Nephrol 14:301–304
Klein GL, Nicolai M, Langman CB et al (1997) Dysregulation of calcium homeostasis after severe burn injury in children: possible role of magnesium depletion. J Pediatr 131:246–251
Sousa AA, Salles JM, Soares JM et al (2010) Evolution of blood magnesium and phosphorus ion levels following thyroidectomy and correlation with total calcium values. Sao Paulo Med J 128:268–271
Yamashita H, Murakami T, Noguchi S et al (1999) Postoperative tetany in Graves’ disease: important role of vitamin D metabolites. Ann Surg 229:237–245
Chia SH, Weisman RA, Tieu D et al (2006) Prospective study of perioperative factors predicting hypocalcemia after thyroid and parathyroid surgery. Arch Otolaryngol Head Neck Surg 132:41–45
Lips P, Bouillon R, van Schoor NM et al (2010) Reducing fracture risk with calcium and vitamin D. Clin Endocrinol (Oxf) 73:277–285
Acknowledgments
This study was supported by the Hormone Laboratory at Oslo University Hospital-Aker. The authors are grateful to the staff there and in the Department of Endocrinology at Oslo University Hospital-Aker, especially biomedical laboratory scientist Nina Gjerlaugsen, for their remarkable help in organizing the bio-bank and analyses. Also, special thanks to Professor Jens Peter Berg for his valuable support and help. The authors extend particular thanks to all participants in the study.
Conflicts of interests
There is no potential conflict of interest of any authors relevant to this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hammerstad, S.S., Norheim, I., Paulsen, T. et al. Excessive Decrease in Serum Magnesium After Total Thyroidectomy for Graves’ Disease Is Related to Development of Permanent Hypocalcemia. World J Surg 37, 369–375 (2013). https://doi.org/10.1007/s00268-012-1843-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-012-1843-2