
Abstract
Purpose
Epidermal growth factor receptor (EGFR) mutations and the anaplastic lymphoma kinase (ALK) rearrangement are the two most common druggable targets in non-small cell lung cancer (NSCLC). However, genetic testing is sometimes unavailable. Previous studies regarding the predictive role of 18F–FDG PET/CT for EGFR mutations in NSCLC patients are conflicting. We investigated whether or not 18F–FDG PET could be a valuable noninvasive method to predict EGFR mutations and ALK positivity in NSCLC using the largest patient cohort to date.
Methods
We retrospectively reviewed and included 849 NSCLC patients who were tested for EGFR mutations or ALK status and subjected to 18F–FDG PET/CT prior to treatment. The differences in several clinical characteristics and three parameters based on 18F–FDG PET/CT, including the maximal standard uptake value (SUVmax) of the primary tumor (pSUVmax), lymph node (nSUVmax) and distant metastasis (mSUVmax), between the different subgroups were analyzed. Multivariate logistic regression analysis was performed to identify predictors of EGFR mutations and ALK positivity.
Results
EGFR mutations were identified in 371 patients (45.9%). EGFR mutations were found more frequently in females, non-smokers, adenocarcinomas and stage I disease. Low pSUVmax, nSUVmax and mSUVmax were significantly associated with EGFR mutations. Multivariate analysis demonstrated that pSUVmax < 7.0, female sex, non-smoker status and adenocarcinoma were predictors of EGFR mutations. The receiver operating characteristic (ROC) curve yielded area under the curve (AUC) values of 0.557 and 0.697 for low pSUVmax alone and the combination of the four factors, respectively. ALK-positive patients tended to have a high nSUVmax. Younger age and distant metastasis were the only two independent predictors of ALK positivity.
Conclusion
We demonstrated that low pSUVmax is associated with mutant EGFR status and could be integrated with other clinical factors to enhance the discriminability on the EGFR mutation status in some NSCLC patients whose EGFR testing is unavailable.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Over the last decade, the introduction of tyrosine-kinase inhibitors (TKIs) has enabled a remarkable paradigm shift in the treatment of non-small cell lung cancer (NSCLC), especially in advanced adenocarcinoma (ADC). Epidermal growth factor receptor (EGFR) mutations and the echinoderm microtubule-associated protein-like 4 (EML4)-anaplastic lymphoma kinase (ALK) rearrangement are the two most-prevalent druggable targeting categories in NSCLC patients [1]. Randomized clinical trials have demonstrated that progression-free survival (PFS) is longer with TKIs than with chemotherapy when EGFR mutations [2, 3] or the ALK rearrangement [4, 5]are present in advanced NSCLC. Furthermore, the TKI efficacy is dependent on the presence of EGFR mutations or the ALK rearrangement. These discoveries have led to the recommendation of molecular profiling as the standard of care for advanced ADC patients [6, 7]. However, the acquisition of sufficient good-quality tumor tissues for gene alteration analyses remains challenging in many cases of advanced NSCLC.
18F–FDG PET is a widely used noninvasive diagnostic modality that is based on different rates of 18F–FDG uptake. EGFR signaling regulates the glucose metabolic pathway in EGFR-mutated lung cancer cells, and EGFR-TKIs decrease lactate production and glucose consumption [8]. Another study has also shown that EGFR-TKIs reverse the Warburg effect and decrease 18F–FDG uptake in mice bearing H1975- EGFR mutant or H1993-EGFR mutant tumors [9]. Thus, 18F–FDG avidity on PET may be useful as a noninvasive biomarker for predicting EGFR mutations and the ALK rearrangement.
Previous data concerning the association between 18F–FDG uptake and EGFR mutations are conflicting [10,11,12,13,14,15,16,17,18], and little is known about the correlation between 18F–FDG avidity and the ALK rearrangement [19, 20]. Thus, this study retrospectively reviewed patients in the last 5 years and included 849 NSCLC patients to investigate whether or not 18F–FDG PET could be a valuable method for predicting EGFR mutations and the ALK rearrangement in NSCLC.
Materials and methods
Patients and inclusion criteria
We retrospectively reviewed all NSCLC patients whose EGFR or ALK statuses were analyzed and who underwent PET/CT from January 2012 to September 2016. A total of 1042 patients was identified. We excluded 193 patients from this study for one of three reasons: (1) for 43 patients, the time interval between sampling and PET/CT exceeded 1 month; (2) 26 patients had a history of malignancy; and (3) 124 patients had been treated before sampling for the gene alteration analysis. Hence, a total of 849 patients were ultimately included in this study. Patient clinical characteristics including age, sex, smoking history, histopathology, tumor size, nodal involvement, distant metastasis and tumor stage were recorded. Non-smokers were defined as patients who never smoked or smoked less than 100 cigarettes in their lifetimes. The rest were categorized as ever-smokers. Tumor node metastasis (TNM) staging was based on the IASLC 8th TNM Lung Cancer Staging System.
18F–FDG PET/CT acquisition and analysis
PET/CT was performed on a Discovery LS PET/CT system (GE Medical Systems). Patients fasted for at least 6 h before examination. The blood glucose concentration was tested and confirmed to be less than 6.6 mmol/L before intravenous injection of 5.5 MBq/kg 18F–FDG. Imaging acquisition was conducted 1 h after 18F–FDG administration. Attenuation correction CT was performed using the following parameters: 120 kV, 80 mA, and 4.25 mm collimation. Then the PET scan was immediately acquired from the head to the upper leg in 2-dimensional mode at 3 min per bed position. Typically, 6–8 bed positions were examined depending on the height of patient. The PET data were reconstructed using the ordered set expectation maximization algorithm method. CT images were used for attenuation correction of the PET data and anatomic localization. The co-registered images were then displayed on the Xeleris Workstation (GE Medical System) for evaluation.
All PET/CT data were independently reviewed by two experienced nuclear medicine physicians. All reviewers were blinded to the EGFR and ALK status. A region of interest (ROI) was placed over the primary tumor, nodal metastasis and distant metastasis to measure each SUVmax. SUVmax was calculated with the most commonly applied formula: SUVmax = maximum pixel activity/ (injected dose/body weight).
ALK Ventana immunohistochemistry (IHC)
Ventana IHC is a fully automated IHC assay that is based on a monoclonal antibody, D5F3. Ventana IHC has been approved by the US FDA and China FDA for the identification of patients with NSCLC who are eligible for treatment with ALK TKIs. According to the manufacturer’s instructions and scoring algorithm, the assay was conducted with 4 μm-thick formalin-fixed, paraffin-embedded tissue sections. The result was dichotomous whereby the presence of any percentage of positive tumor cells with strong granular cytoplasmic staining was deemed ALK positive, while all other observations were deemed ALK negative.
EGFR mutation analysis
EGFR mutations were analyzed based on the principle of the amplification refractory mutation system (ARMS). Briefly, resected, aspirated or biopsied primary tumor, lymph node, or distant metastasis samples or pleural effusion samples were fixed in 10% neutral buffered formalin and embedded in paraffin wax. The DNA was extracted from the formalin-fixed, paraffin-embedded tissue sections using the QIAamp DNA FFPE tissue kit (Qiagen NV, Venlo,Netherlands) according to the manufacturer’s instructions. Polymerase chain reaction was carried out with the Mx3000PtM (Stratagene, La Jolla, USA) using the EGFR 29 Mutations Detection Kit (Amoy Diagnostics, Xiamen, People’s Republic of China), and the result was interpreted according to the manufacturer’s instructions.
IHC analysis
The IHC analysis was conducted by pathologists from the Department of Pathology of Wuhan Union Hospital. Briefly, the 4 μm-thick formalin-fixed, paraffin-embedded tissue sections were analyzed using the following primary antibodies: TTF-1 (clone 8G7G3/1, Maixin, Fuzhou, China), NapsinA (multiclone, Maixin), CK-7 (clone OV-TL 12/30, Maixin), and Ki67 (clone MX006, Maixin). Positive expression of TTF-1 was defined as >5% of tumor cells with distinct cytoplasmic or nuclear staining. The presence of >50% of tumor cells with diffuse and intense cytoplasmic staining was deemed positive for Napsin-A and CK-7. The percentage of tumor cells with distinct nuclear staining of Ki67 was denoted with a Ki67 score.
Statistical analysis
Clinical characteristics including the PET/CT parameters were compared according to the EGFR or ALK status using the chi-squared test and Student’s t-test. A two-sided p value < 0.05 was defined as statistically significant. Receiver operating characteristics (ROC) curves were constructed to obtain the cutoff value of the primary tumor SUVmax (pSUVmax) for predicting the EGFR mutations status. Logistic regression analysis was performed to identify independent predictors of the EGFR or ALK status. Clinical parameters and a pSUVmax with p < 0.05 in the univariate analysis, as well as previously reported factors associated with EGFR or ALK status, were further analyzed by multivariate regression analysis. Variates with p < 0.05 in the multivariate analysis were deemed independent predictors, and the odds ratios and 95% confidence intervals of the predictors were obtained. ROC curves were constructed for the combined independent factors for predicting mutant EGFR. All analyses were performed using the SPSS software package (version 16.0; SPSS, Chicago, IL, USA).
Results
Patient and tumor characteristics
Among the 849 NSCLC patients tested for EGFR and ALK status in our hospital between January 2012 to September 2016, 808 were tested for EGFR, 223 were tested for ALK, and 182 were tested for both. The clinical characteristics are summarized in Table 1 based on whether the patients were tested for EGFR or ALK.
Of the 808 patients tested for EGFR status, EGFR mutations were identified in 371 (45.9%); the patient group included 340 women (42.1%) and 468 men (57.9%) with a median age of 58.7 years (range, 25–85), and 498 (63.6%) were non-smokers. Seven hundred and thirty-one patients (90.5%), 58 patients (7.2%) and 19 patients (2.3%) were histologically confirmed to have ADCs, squamous cell carcinomas and other subtypes, respectively; the other subtypes included four large cell carcinomas and 15 undefined NSCLCs. One hundred and forty-two (17.5%), 49 (6.4%), 157 (19.4%) and 460 (56.8%) patients had stage I, stage II, stage III and stage IV disease, respectively. The median SUVmax of the primary tumor was 9.8 (range, 0.8–45.7).
Of the 223 patients tested for ALK, 17 (7.6%) were positive for ALK; the patient group included 101 women (45.3%) and 122 men (54.7%) with a median age of 58.2 years (range, 29–85), and 139(62.3%) were non-smokers. One hundred and ninety (85.2%), 25 (11.2%) and eight (3.5%) patients had histologically confirmed ADCs, squamous cell carcinomas and other subtypes, respectively; the other subtypes included one large cell carcinoma and seven undefined NSCLCs. Forty (17.9%), 11 (4.9%), 45 (20.2%) and 127 (57.0%) patients had stage I, stage II, stage III and stage IV disease, respectively. The median SUVmax of the primary tumor was 10.4 (range, 0.8–33.2).
Association between clinical characteristics and EGFR mutations
The clinical characteristics of the NSCLC patients are summarized in Table 1 based on the EGFR status. EGFR mutations were found more frequently in women (60.6% vs. 35.3%; p < 0.001), non-smokers (55.8% vs. 30.0%; p < 0.001), ADCs (50.2% vs. 9.1%; p < 0.001), and stage I patients (61.3% vs. 32.7%, 38.9%, and 45.0%; p < 0.001). Positive expression of IHC marker TTF-1 (47.7% vs. 14.1%; p < 0.001), NaspinA (45.8% vs. 16.5%; p < 0.001), and CK7 (37.9% vs. 8.7%; p = 0.005) were significantly associated with EGFR mutations. The Ki67 scores (22.4 ± 21.2 vs. 33.4 ± 22.1; p = 0.002) were lower in the EGFR-mutant NSCLC patients than in the EGFR wild-type patients. The PET parameters of the pSUVmax (8.7 ± 4.8 vs. 10.7 ± 6.2; p < 0.001) (Fig. 1 a), nodal metastases SUVmax (nSUVmax) (7.3 ± 4.2 vs. 9.3 ± 5.5; p < 0.001) and distant metastases SUVmax (mSUVmax)(8.0 ± 4.9 vs. 9.5 ± 5.7; p = 0.005) were lower in the EGFR-mutant NSCLCs than in the EGFR wild-type NSCLCs. There were no differences in the pSUVmax results between the different EGFR mutation types, including in-frame deletion in exon 19 and substitution mutation in exon 21 (Fig. 1 b). Representative PET/CT images of two patients with EGFR mutant or wild-type NSCLC were shown (Fig. 2). The ROC curve analysis revealed that the cutoff point for the pSUVmax was 7.0; 72.8% sensitivity, 38.5% specificity, a 54.6% positive predictive value, a 58.2% negative predictive value, and 57.1% accuracy were achieved, and the area under curve (AUC) was 0.557 (95%CI, 0.517–0.596) with p = 0.001. Thus, although EGFR mutations were more frequently found in patients with pSUVmax < 7.0 (p = 0.001), pSUVmax was only a marginal significant predictor of EGFR mutations.

Comparison of non-small cell lung cancer 18F–FDG uptake according to EGFR mutation status. Primary tumor SUVmax are shown for subjects categorized according to epidermal growth factor receptor (EGFR) mutation status including wild-type EGFR (EGFR WT) and mutations in EGFR exon 19 and exon 21

Representative EGFR status and 18F–FDG PET/CT findings. Top panel,findings of a 53-year-old man with EGFR-wild type lung adenocarcinoma. CT (a) and PET (b) images show a 2.9-cm-sized hypermetabolic mass in the right upper lobe (pSUVmax = 18.8). Hematoxylin-eosin staining (c) shows histological type of adenocarcinoma and the ARMS method (d) demonstrates wild type EGFR status. Bottom panel, findings of a 62-year-old woman with EGFR-mutant lung adenocarcinoma. CT (e) and PET (f) show a 2.6-cm-sized mass with mild 18F–FDG uptake (pSUVmax = 4.8) in the right lower lobe. Hematoxylin-eosin staining (g) shows histological type of adenocarcinoma and the ARMS method (h) demonstrates L858R substitution mutation in EGFR exon 21
Due to the large differences in the EGFR mutation rates and 18F–FDG avidity between ADC and non-ADC, the ADC-only group was separately analyzed; the data are summarized in Table 2. The results were similar to those of the NSCLC group, except for CK7, which was not associated with EGFR mutations.
Association between clinical characteristics and ALK status
The ALK-positive NSCLC patients were more frequently younger age (50.5 ± 9.7 vs. 58.8 ± 9.6; p = 0.001). Positive ALK expression was observed only in the ADC patients (17/190 vs. 0/33), although the p value was 0.083 because the population of non-ADC patients was relatively small (Table 1). Although there was no significant difference in sex and smoking history between the ALK-positive and ALK-negative groups, females (8.9% vs. 6.6%) and non-smokers (9.4% vs. 4.8%) tended to have higher positivity rates than men and ever-smokers. Interestingly, positive expression of ALK was exclusively observed in TTF-1-, NaspinA- and CK7-positive NSCLC patients regardless of ADC or non-ADC status. The Ki67 scores (16.9 ± 9.6 vs. 38.4 ± 26.1; p = 0.026) were lower in the ALK-positive group than in the ALK-negative group. The nSUVmax was the only PET parameter that was higher in the ALK-positive patients than in the ALK-negative patients (10.6 ± 3.5 vs. 8.6 ± 4.9), with a marginal p value (0.091). The pSUVmax and mSUVmax were not significantly different between the two groups.
When the ADC group was separately analyzed, a young age (50.6 ± 11.4 vs. 58.9 ± 9.5; p < 0.001), high nSUVmax (10.7 ± 4.6 vs. 8.3 ± 5.2; p = 0.004) and low Ki67 score were significantly associated with positive ALK expression (Table 2).The other results were similar to those of the NSCLC groups.
Prediction of the EGFR mutation status
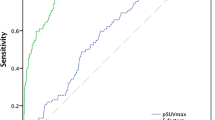
For the NSCLC group (Table 3), the univariate logistic regression analysis showed that sex, smoking status, histology, pSUVmax, tumor size, nodal involvement, distant metastasis, and tumor stage were significantly correlated with EGFR mutations. Then inclusion of these factors together in the multivariate regression analysis revealed that sex, smoking status, histology and pSUVmax remained independent variables for predicting EGFR mutations. Female sex (odds ratio [OR], 1.83; p = 0.003), non-smoker status (OR, 1.79; p = 0.006), ADC (OR, 7.09; p < 0.001) and pSUVmax < 7.0 (OR, 1.48; p = 0.041) were significant predictors of EGFR mutations. Additionally, a ROC curve analysis was conducted to evaluate the predictive value of these factors (Fig. 3), and the AUC of the categorical pSUVmax < 7.0 was 0.557. When the four criteria were used together, the AUC was 0.697.

Receiver operating characteristic curves of primary tumor SUVmax and combination of four factors (pSUVmax, sex, smoking history and histological type) for predicting EGFR mutation
For the ADC-only group (Table 4), the univariate logistic regression analysis showed that sex, smoking status, pSUVmax, tumor size, nodal involvement and tumor stage were associated with EGFR mutations. In the multivariate logistic regression analysis, female sex (OR, 1.91; p = 0.002), non-smoker status (OR, 1.74; p = 0.010), and pSUVmax < 7.0 (OR, 1.51; p = 0.036) were independent factors for predicting EGFR mutations in ADC patients.
Prediction for ALK status
For the NSCLC group (Table 5), which included 190 ADC patients and 33 non-ADC patients, univariate regression showed that a young age was the only statistically significant variate that was associated with positive ALK expression (OR, 0.92). Patients with distant metastasis also tended to be ALK positive (OR, 1.66; 95% CI, 0.98–2.81), although the p value was 0.058. In the multivariate analysis, sex, smoking history, histology, and the pSUVmax were analyzed together with age and distant metastasis. Younger age was still the only independent predictor of ALK positivity, although the OR of distant metastasis was 4.23 (p = 0.071). The pSUVmax was not associated with ALK status.
The results of the separate analysis of the 190 ADC patients were similar to those of the NSCLC group (Table 6). Notably, the nSUVmax was not included the multivariate analysis because of the small sample size. Likewise, too few of the ADC patients were negative for TTF-1, NaspinA and CK7, so TTF-1, NaspinA and CK7 were also not included.
Discussion
TKIs have shown remarkable therapeutic effects and prolonged PFS in NSCLC patients with EGFR mutations or the ALK rearrangement [2,3,4,5]. These discoveries have led to the recommendation of molecular profiling as the standard of care for advanced NSCLC patients [6, 7]. However, the availability of sufficient good-quality tumor tissues for the gene alteration analyses is often challenging in advanced NSCLC patients. In this study, we demonstrate that NSCLC patients with EGFR mutations had lower pSUVmax measurements based on 18F–FDG PET than NSCLC patients with wild-type EGFR and that low pSUVmax could be integrated with other clinical factors to enhance the discriminability on the EGFR mutation status in some NSCLC patients whose EGFR testing is unavailable.
Data from previous studies that have investigated the value of 18F–FDG PET for predicting EGFR status are conflicting. Na et al. [18] and Cho et al. [21] revealed that a lower pSUVmax was an independent variate for predicting EGFR mutations. Two other groups reported the opposite result, where a higher pSUVmax predicted EGFR mutations [10, 14]. Moreover, multiple groups reported no association between the pSUVmax and EGFR status [12, 22].
Our data were consistent with observation by Na et al. [18]and Cho et al. [21], whereby a lower pSUVmax was an independent variate for predicting EGFR mutations. Cho et al. included 58 ADC and three non-ADC patients regardless of tumor stage; the study was conducted in Korea, and the EGFR mutation rate was 50%. The OR in the multivariate analysis that assessed the predictive value of a low pSUVmax for EGFR mutations was 12.97 (p = 0.005) [21]. The study by Na et al. contained 100 NSCLC patients, including 53 ADC and 47 non-ADC patients regardless of tumor stage; the study was also conducted in Korea, and the EGFR mutation rate was 21%. The OR of a low pSUVmax being predictive of EGFR mutations in the study by Na et al. was 1.3 (p = 0.025), which was similar to our result [18].
Several possible reasons may underlie these contradictory results. Our study included NSCLCs of all stages and histological types. In a separate analysis of stage IV ADC, the pSUVmax was not different between the EGFR-mutant and wild-type stage IV ADC patients, which was consistent with the result from Lee’s group [13]. Hence, the tumor stage and histological type of the studied patient population could significantly influence the results concerning this topic. Only two groups reported that a high pSUVmax was positively associated with EGFR mutations [10, 14]. However, all other studies revealed that EGFR-mutant patients tended to have a lower pSUVmax than EGFR wild-type patients, although the results were not statistically significant in the studies by Huang et al. [14] and Ko et al. [10]. Huang’s group included 77 stage III and stage IV ADC patients (excluding the bronchoalveolar subtype), and Ko’s group included 132 stage I-IV ADC patients who also had pretreatment serum CEA and CT assessments. The high EGFR mutation rate (64%) may suggest patient selection bias, and the patient population size in Huang’s study was relatively small. In Ko’s study, the requirement for pretreatment serum CEA and CT assessments may have promoted patient selection bias compared to other studies.
The results from the studies by Chung et al. [23] and Mak et al. [12] showed no statistically significant difference in the pSUVmax between the EGFR-mutant and wild-type patients. Lee et al. revealed that the pSUVmax was statistically significant only in the univariate regression analysis but not in the multivariate regression analysis. Our results showed that despite the statistically significant predictive role of pSUVmax for determining the EGFR mutation status, the pSUVmax measurements between the EGFR-mutant and wild-type groups substantially overlapped. Moreover, the AUC was only 0.557. The ADC patient population sizes were only 106, 90, and 135 in the studies by Chung et al., Mak et al. and Lee et al., respectively. Therefore, the small number of patients and modest discriminating power of the pSUVmax can explain these discrepant results.
Guan's group identified tumor size as a predictor for EGFR mutation on multivariate analysis, which is not consistent with our study. The higher proportion of non-ADC patients in Guan group’s data may cause this discrepancy. The primary tumor size of ADC patients tend to be smaller than that of non-ADC NSCLC patients. In our data, the average tumor size of ADC patients was 3.28 cm vs. 5.13 cm in non-ADC NSCLC patients. According to the cutoff value of 5 cm in Guan group’s study, the patients with primary tumor size >5 cm was 46.6% in non-ADC patients vs. 13.6% in ADC patients in our cohort. Thus, non-ADC NSCLC patient population composed much higher proportion patients with primary tumor size >5 cm and generally accepted much lower EGFR mutant rate than ADC patient population. Thus, the proportion of non-ADC patients in studied cohort will significantly affect the statistical result of the correlation between tumor size and EGFR mutation status. The proportion of non-ADC patients in Guan group’s study was 23.4% vs. 9.5% in our data. Actually, when ADC patients and non-ADC NSCLC patients were analyzed as a whole in our study, the primary tumor size of EGFR mutant patients was also smaller than that of EGFR wild-type patients (p = 0.02). However, there was no significant difference of tumor size between EGFR mutant patients and EGFR wild-type patients when ADC-only group was separately analyzed. Thus, the higher proportion of non-ADC NSCLC patients in Guan group’s data compared with our included population may cause this discrepancy.
In our study, the pSUVmax was associated with mutant EGFR status. The AUC was 0.697 when the four criteria, including pSUVmax < 7.0, female, non-smoker and histologic type of ADC were analyzed together for predicting EGFR mutation status. The result of the separate analysis of the ADC group was similar. An important notable issue is that the clinicians preferred to select ADC patients for EGFR mutation analysis, resulting in the included patient population is quite different with actually clinical status. The non-ADC NSCLC patient population accounted for only 77 patients (9.5%) of the 808 NSCLC population in our study population compared with about 38.9% in the actually clinical practice from the Chinese National Office for Cancer Prevention and Control data [24,25,26]. The pSUVmax of non-ADC patients was much higher than that of ADC population in our study (14.30 vs. 9.29, p < 0.001) and previously published studies [27, 28]. The EGFR mutant rate of non-ADC NSCLC patients was universally accepted much lower than ADC population. Thus the discriminability of pSUVmax for EGFR mutation may be underestimated in our study population as compared to actually clinical practice due to extremely small proportion of non-ADC patients. As commonly applied method to imitate the actually ratio between ADC and non-ADC NSCLC in clinic, the SPSS software enabled us to randomly select 122 ADC patients (16% of those total 731 ADC patients). Then we combined those 122 ADC patients with 77 non-ADC patients for analysis. When pSUVmax, smoking status, sex and histology of ADC were used together, the AUC of ROC analysis increased from 0.697 to 0.782 (data not shown), which indicated that those four factors could provide relative good performance for predicting EGFR mutation status.
EGFR mutant status from the tissue genetic analysis was the gold standard for first-line treatment with EGFR-TKIs. The guidelines for NSCLC treatment of China [29], ESMO [30], ASCO [31] and NCCN [32] all suggest EGFR mutation testing from tissue assays prior to first-line treatment with EGFR-TKIs. However, EGFR mutation testing was sometimes unavailable for oncologists to decide the therapeutic regimen. In European and North America approximate one-quarter advanced NSCLC patients were not available with EGFR mutation testing in 2015 [33]. In China, EGFR testing rate was only 9.6% in 2010 from a national survey [34], 18.3% in 2011 from nine sites including 12,086 NSCLC patients [35], and 42.5% in 2014 from a non-interventional real world study on EGFR testing in patients with IIIB/IV NSCLC in northern China [36]. An unpublicized investigation from our institution including 4062 NSCLC patients revealed the EGFR mutation testing rate was 45.2% in 2015 and 49.6% in 2016.
Several reasons may account for the low EGFR mutation testing rate in China. First, many patients were not available with tumor tissues. The Health and Social Care Information Centre recorded that about 23% patients were not available with tumor tissues in the United Kingdom [37]. From our clinical experience, about 30% of patients cannot obtain samples owing to personal subjective refusal of invasive examination or several objective reasons resulting in ineligible for sampling including coagulation abnormalities, severe cardiopulmonary insufficiency, arterial and venous pulmonary hypertension, high risk of pneumothorax, usage of anticoagulant drugs and patient uncooperativeness. Second, the diagnosis of NSCLC has been more and more relying on small biopsy or cytologic specimens which however sometimes were not of good quality or sufficient number of tumor cells for EGFR mutation testing. The data from a study concerning “real-world” EGFR mutation testing practices in Asia in 2011 showed that 53.8% sample tested for EGFR mutation were small biopsy or cytology specimens in China [35]. The data from our institute in the last 5 years showed that small biopsy and cytology specimens account for 68.4% of all samples tested for EGFR (data not shown). Minimally invasive examinations for diagnosis of lung cancer included fine-needle aspiration (FNA), core biopsy, bronchoscopy with biopsy and transbronchial needle aspiration (TBNA), endobronchial ultrasound (EBUS)-guided biopsy, and the cytologic specimen from bronchial washing, bronchial brushing, sputum, bronchoalveolar lavage fluid (BALF) and pleural effusion [38]. Those minimal invasive examinations have significantly improved lung cancer diagnosis; however, small samples and cytologic specimens were sometimes not sufficient of quality or quantity for EGFR mutation testing in which the reported failure rates are about 5% to 30% [39,40,41]. Third, limited medical resource and incomplete implementation of guidelines in some medical institutions may also result in low EGFR mutation testing rate.
Thus, a natural question is how to select the patients potentially benefited from EGFR-TKIs treatment among the patients without available EGFR testing and those who cannot tolerate chemotherapy. Two previous randomized head-to-head clinical trials showed that among patients with unknown EGFR status, patients selected by only clinical factors had a greater response and better PFS with EGFR-TKI treatment than with chemotherapy in the first-line treatment [42,43,44]. The aim of our study is to investigate whether 18F–FDG PET/CT could be a useful modality to enhance patient stratification in some NSCLC patients whose EGFR testing is unavailable. Our result showed that low pSUVmax is associated with mutant EGFR status. It could be integrated with other clinical factors to enhance the discriminability on the EGFR mutation status and be used by oncologists to decide the treatment strategy in some NSCLC patients without available EGFR testing.
Different EGFR mutation types can drive distinct downstream signaling, TKI affinities and treatment responses [45, 46]. In-frame deletion in exon 19 and L858R substitution mutation in exon 21 account for most EGFR mutations in NSCLC [47]. A previous study indicated that exon 19 in-frame deletions showed longer PFS following an EGFR TKI treatment [45]. The 18F–FDG avidity of these two mutation types was also evaluated previously. Choi et al. showed that the pSUVmax of NSCLC patients with the L858R mutation was significantly higher than that of NSCLC patients with the exon 19 mutation (11.6 vs. 8.2) [48]. However, Lee’s group revealed no difference between the two mutation types [22]. Consistent with the result by Lee et al., the pSUVmax measurements of the two mutation types were not significantly different in our study.
The EML4-ALK rearrangement is another driver mutation and druggable target in NSCLC. The ALK rearrangement in NSCLC patients shows a dramatic response and prolonged PFS with an ALK TKI treatment [4, 5]. Our study investigated the metabolic features of ALK-positive NSCLC patients. Among the ADC patients, the nSUVmax was higher in the ALK-positive group than in the ALK-negative group. However, there was no difference in the pSUVmax between the two groups. Jeong et al. reported that a higher pSUVmax was an independent predictor of ALK positivity [19]. There are two possible explanations for this discrepancy. First, 53 previously treated patients were included in the study by Jeong et al. Second, selection bias may have influenced the results; the ALK analysis was conducted after evaluating the EGFR and K-ras status, and the ALK positivity (18.6%) of the patient population in the study may have strengthened the statistical significance. Another study that included 5.4% ALK-positive ADCs also showed a higher pSUVmax in ALK-positive patients than in ALK-negative patients [20]. These two studies identified ALK-positive patients by FISH, whereas the Ventana IHC system was used to determine the ALK status in our study. The different detection methods may explain the discrepant results. However, the Ventana IHC system is a fully automated IHC assay, with a sensitivity of 100% and specificity of 98%, that has been approved by the US FDA and China FDA for the identification of NSCLC patients who are eligible for treatment with ALK TKIs [49]. Moreover, multiple studies have reported that Ventana ALK IHC is a better predictor of the ALK inhibition outcome than ALK-FISH for advanced NSCLC [50]. The response rates to the ALK inhibitors were 100% in the FISH-negative/IHC-positive cases (7/7) and 46% in the FISH-positive/IHC-negative cases (13/28) [51].
There are several limitations to this study. First, the retrospective design may have introduced bias, including patient selection bias and sample availability bias. Second, the Asia-Pacific region NSCLC/ADC subgroup have the highest EGFR mutation frequency at 47% compared with other regions [52]. The patients in our study were all Chinese and thus had a genetic alteration pattern that was distinct from other races, which may impede the application of our results to other races. Although two studies from Spain and the U.S. also showed lower pSUVmax in EGFR mutant NSCLC patients than that in EGFR wild-type patients [11, 12], it is still necessary to note the potential difference between different regions and races. Third, many lymph nodes and distant metastases were not histologically verified. Hence, we did not include nSUVmax and mSUVmax in the multivariate analysis. Fourth, 18F–FDG uptake is actually nonspecific and is a net result of microvasculature for delivering nutrients, glucose transporter of transporting 18F–FDG into the cell, HK for entering 18F–FDG into glycolysis and the number of tumor cells [53]. Any factors that can regulate those steps will influence 18F–FDG uptake. For example, intracellular pH is an important factor influencing glycolysis and 18F–FDG uptake [54]. An alkaline intracellular pH could promote glycolysis which depends on the pH-sensitive activity and abundance of several glycolytic enzymes including lactate dehydrogenase [55, 56], phosphofructokinase 1 [57, 58], phosphorylase kinase [56] and fructose-1,6-bisphosphatase [56]. However, different driver mutations may also result in distinct pathways activation and glycolytic features [59,60,61]. Moreover, driver mutations including K-ras mutation, EGFR mutation, ALK rearrangement, ROS1 rearrangement, PI3K mutation et al. are almost mutually exclusive in NSCLC patients [62]. So it is still reasonable to use 18F–FDG uptake to distinguish different driver mutations in NSCLC. A study by Carlos group showed that pSUVmax of NSCLC patients with K-ras mutation was much higher than that of NSCLC patitents with EGFR mutation [11].
In conclusion, our study aimed to investigate whether or not 18F–FDG PET could be a valuable noninvasive method for predicting EGFR mutations and ALK positivity in NSCLC using the largest patient population to date. We identified that pSUVmac < 7.0 was associated with EGFR mutation in NSCLC patients The AUC of the ROC curve analysis of four factors, including pSUVmax < 7.0, female sex, non-smoker status and histologic type of ADC was 0.697. When the ratio between ADC and non-ADC NSCLC patients mimicked the actually clinic status, the AUC increased to 0.782 indicating that those four factors could provide relative good performance for predicting EGFR mutation status. The pSUVmax measurements were not different between the ALK-positive and ALK-negative groups in our study. Other noninvasive biomarkers could be investigated and integrated with 18F–FDG PET in the future to optimize the predictive power for the EGFR and ALK status when tissues for genetic analysis are unavailable. For example, exquisite algorithms for analyzing diagnostic CTs and PET/CTs have already been developed to obtain more information for predicting genetic alterations in NSCLC patients [16, 17, 63]. Radiolabled EGFR-TKI and anti-EGFR antibody for TKI-PET and immuno-PET are also very promising modalities for predicting EGFR mutation status and clinical efficiency of TKI treatment [64]. Exnograft mouse models and several clinical studies [65,66,67] have showed exciting results and two clinical trials are ongoing.
References
Minguet J, Smith KH, Bramlage P. Targeted therapies for treatment of non-small cell lung cancer--recent advances and future perspectives. Int J Cancer. 2016;138:2549–61. https://doi.org/10.1002/ijc.29915.
Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947–57. https://doi.org/10.1056/NEJMoa0810699.
Pao W, Miller V, Zakowski M, Doherty J, Politi K, Sarkaria I, et al. EGF receptor gene mutations are common in lung cancers from "never smokers" and are associated with sensitivity of tumors to gefitinib and erlotinib. Proc Natl Acad Sci U S A. 2004;101:13306–11. https://doi.org/10.1073/pnas.0405220101.
Solomon BJ, Mok T, Kim DW, Wu YL, Nakagawa K, Mekhail T, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014;371:2167–77. https://doi.org/10.1056/NEJMoa1408440.
Shaw AT, Kim DW, Nakagawa K, Seto T, Crino L, Ahn MJ, et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med. 2013;368:2385–94. https://doi.org/10.1056/NEJMoa1214886.
Lindeman NI, Cagle PT, Beasley MB, Chitale DA, Dacic S, Giaccone G, et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Mol Diagnostics : JMD. 2013;15:415–53. https://doi.org/10.1016/j.jmoldx.2013.03.001.
Leighl NB, Rekhtman N, Biermann WA, Huang J, Mino-Kenudson M, Ramalingam SS, et al. Molecular testing for selection of patients with lung cancer for epidermal growth factor receptor and anaplastic lymphoma kinase tyrosine kinase inhibitors: American Society of Clinical Oncology endorsement of the College of American Pathologists/international association for the study of lung cancer/association for molecular pathology guideline. J Clin Oncol : Off J Am Soc Clin Oncol. 2014;32:3673–9. https://doi.org/10.1200/JCO.2014.57.3055.
Makinoshima H, Takita M, Matsumoto S, Yagishita A, Owada S, Esumi H, et al. Epidermal growth factor receptor (EGFR) signaling regulates global metabolic pathways in EGFR-mutated lung adenocarcinoma. J Biol Chem. 2014;289:20813–23. https://doi.org/10.1074/jbc.M114.575464.
De Rosa V, Iommelli F, Monti M, Fonti R, Votta G, Stoppelli MP, et al. Reversal of Warburg effect and reactivation of oxidative Phosphorylation by differential inhibition of EGFR signaling pathways in non-small cell lung cancer. Clin Cancer Res : Off J Am Assoc Cancer Res. 2015;21:5110–20. https://doi.org/10.1158/1078-0432.CCR-15-0375.
Ko KH, Hsu HH, Huang TW, Gao HW, Shen DH, Chang WC, et al. Value of (1)(8)F-FDG uptake on PET/CT and CEA level to predict epidermal growth factor receptor mutations in pulmonary adenocarcinoma. Eur J Nucl Med Mol Imaging. 2014;41:1889–97. https://doi.org/10.1007/s00259-014-2802-y.
Caicedo C, Garcia-Velloso MJ, Lozano MD, Labiano T, Vigil Diaz C, Lopez-Picazo JM, et al. Role of [(1)(8)F]FDG PET in prediction of KRAS and EGFR mutation status in patients with advanced non-small-cell lung cancer. Eur J Nucl Med Mol Imaging. 2014;41:2058–65. https://doi.org/10.1007/s00259-014-2833-4.
Mak RH, Digumarthy SR, Muzikansky A, Engelman JA, Shepard JA, Choi NC, et al. Role of 18F-fluorodeoxyglucose positron emission tomography in predicting epidermal growth factor receptor mutations in non-small cell lung cancer. Oncologist. 2011;16:319–26. https://doi.org/10.1634/theoncologist.2010-0300.
Lee EY, Khong PL, Lee VH, Qian W, Yu X, Wong MP. Metabolic phenotype of stage IV lung adenocarcinoma: relationship with epidermal growth factor receptor mutation. Clin Nucl Med. 2015;40:e190–5. https://doi.org/10.1097/RLU.0000000000000684.
Huang CT, Yen RF, Cheng MF, Hsu YC, Wei PF, Tsai YJ, et al. Correlation of F-18 fluorodeoxyglucose-positron emission tomography maximal standardized uptake value and EGFR mutations in advanced lung adenocarcinoma. Med Oncol. 2010;27:9–15. https://doi.org/10.1007/s12032-008-9160-1.
Kanmaz ZD, Aras G, Tuncay E, Bahadir A, Kocaturk C, Yasar ZA, et al. Contribution of (1)(8)Fluorodeoxyglucose positron emission tomography uptake and TTF-1 expression in the evaluation of the EGFR mutation in patients with lung adenocarcinoma. Cancer Biomarkers : Section A Dis Markers. 2016;16:489–98. https://doi.org/10.3233/CBM-160588.
Yip SS, Kim J, Coroller TP, Parmar C, Velazquez ER, Huynh E, et al. Associations between somatic mutations and metabolic imaging phenotypes in non-small cell lung cancer. J Nucl Med : Off Publ Soc Nucl Med. 2017;58:569–76. https://doi.org/10.2967/jnumed.116.181826.
Apostolova I, Ego K, Steffen IG, Buchert R, Wertzel H, Achenbach HJ, et al. The asphericity of the metabolic tumour volume in NSCLC: correlation with histopathology and molecular markers. Eur J Nucl Med Mol Imaging. 2016;43:2360–73. https://doi.org/10.1007/s00259-016-3452-z.
Na II, Byun BH, Kim KM, Cheon GJ, du Choe H, Koh JS, et al. 18F-FDG uptake and EGFR mutations in patients with non-small cell lung cancer: a single-institution retrospective analysis. Lung Cancer. 2010;67:76–80. https://doi.org/10.1016/j.lungcan.2009.03.010.
Jeong CJ, Lee HY, Han J, Jeong JY, Lee KS, Choi YL, et al. Role of imaging biomarkers in predicting anaplastic lymphoma kinase-positive lung adenocarcinoma. Clin Nucl Med. 2015;40:e34–9. https://doi.org/10.1097/RLU.0000000000000581.
Choi H, Paeng JC, Kim DW, Lee JK, Park CM, Kang KW, et al. Metabolic and metastatic characteristics of ALK-rearranged lung adenocarcinoma on FDG PET/CT. Lung Cancer. 2013;79:242–7. https://doi.org/10.1016/j.lungcan.2012.11.021.
Cho A, Hur J, Moon YW, Hong SR, Suh YJ, Kim YJ, et al. Correlation between EGFR gene mutation, cytologic tumor markers, 18F-FDG uptake in non-small cell lung cancer. BMC Cancer. 2016;16:224. https://doi.org/10.1186/s12885-016-2251-z.
Lee SM, Bae SK, Jung SJ, Kim CK. FDG uptake in non-small cell lung cancer is not an independent predictor of EGFR or KRAS mutation status: a retrospective analysis of 206 patients. Clin Nucl Med. 2015;40:950–8. https://doi.org/10.1097/RLU.0000000000000975.
Chung HW, Lee KY, Kim HJ, Kim WS, So Y. FDG PET/CT metabolic tumor volume and total lesion glycolysis predict prognosis in patients with advanced lung adenocarcinoma. J Cancer Res Clin Oncol. 2014;140:89–98. https://doi.org/10.1007/s00432-013-1545-7.
Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–32. https://doi.org/10.3322/caac.21338.
Zou XN, Lin DM, Wan X, Chao A, Feng QF, Dai Z, et al. Histological subtypes of lung cancer in Chinese males from 2000 to 2012. Biomed Environ Sci : BES. 2014;27:3–9. https://doi.org/10.3967/bes2014.010.
Zou XN, Lin D, Chao A, Wan X, Feng Q, Li J, et al. Histological subtypes of lung cancer in Chinese women from 2000 to 2012. Thorac Cancer. 2014;5:447–54. https://doi.org/10.1111/1759-7714.12121.
Jiang R, Dong X, Zhu W, Duan Q, Xue Y, Shen Y, et al. Combining PET/CT with serum tumor markers to improve the evaluation of histological type of suspicious lung cancers. PLoS One. 2017;12:e0184338. https://doi.org/10.1371/journal.pone.0184338.
Goodwin J, Neugent ML, Lee SY, Choe JH, Choi H, Jenkins DMR, et al. The distinct metabolic phenotype of lung squamous cell carcinoma defines selective vulnerability to glycolytic inhibition. Nat Commun. 2017;8:15503. https://doi.org/10.1038/ncomms15503.
Zhi X, Shi Y, Yu J. Chinese primary lung cancer diagnosis and treatment standard (2015 edition). Chin J Oncol. 2015;37:67–78. https://doi.org/10.3760/cma.j.issn.0253-3766.2015.01.014.
Novello S, Barlesi F, Califano R, Cufer T, Ekman S, Levra MG, et al. Metastatic non-small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol : Off J Eur Soc Med Oncol. 2016;27:v1–v27. https://doi.org/10.1093/annonc/mdw326.
Hanna N, Johnson D, Temin S, Baker S Jr, Brahmer J, Ellis PM, et al. Systemic therapy for stage IV non-small-cell lung cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol : Off J Am Soc Clin Oncol. 2017;35:3484–515. https://doi.org/10.1200/JCO.2017.74.6065.
Ettinger DS, Wood DE, Aisner DL, Akerley W, Bauman J, Chirieac LR, et al. Non-small cell lung cancer, version 5.2017, NCCN clinical practice guidelines in oncology. J Nat Comprehensive Cancer Netw : JNCCN. 2017;15:504–35.
Spicer JBT, Tischer B. EGFR mutation testing and oncologist treatment choice in advanced NSCLC: global trends and differences. Ann Oncol : Off J Eur Soc Med Oncol. 2015;26:i57–61. https://doi.org/10.1093/annonc/mdv128.4.
Xue C, Hu Z, Jiang W, Zhao Y, Xu F, Huang Y, et al. National survey of the medical treatment status for non-small cell lung cancer (NSCLC) in China. Lung Cancer. 2012;77:371–5. https://doi.org/10.1016/j.lungcan.2012.04.014.
Yatabe Y, Kerr KM, Utomo A, Rajadurai P, Tran VK, Du X, et al. EGFR mutation testing practices within the Asia Pacific region: results of a multicenter diagnostic survey. J Thorac Oncol : Off Publ Int Assoc Stud Lung Cancer. 2015;10:438–45. https://doi.org/10.1097/JTO.0000000000000422.
Cheng YYW, J. Zhao, Y. Liu, H. Gao, K. Ma, S. Zhang. A multicenter, non-interverntional study on real world EGFR testing and in patients with IIIB/IV NSCLC in northern China. IASLC 18th World Conference on Lung Cancer / Abstracts. 2017.
NLCA HaSCIC. National Lung Cancer Audit Report 2012 Available at: http://www.hqip.org.uk/assets/NCAPOP-Library/NCAPOP-2012–13/Lung-Cancer-National-Audit-Report-pub-2012.pdf. Accessed September 27, 2013.
Thunnissen E, Kerr KM, Herth FJ, Lantuejoul S, Papotti M, Rintoul RC, et al. The challenge of NSCLC diagnosis and predictive analysis on small samples. Practical approach of a working group. Lung Cancer. 2012;76:1–18. https://doi.org/10.1016/j.lungcan.2011.10.017.
Shiau CJ, Babwah JP, da Cunha SG, Sykes JR, Boerner SL, Geddie WR, et al. Sample features associated with success rates in population-based EGFR mutation testing. J Thorac Oncol : Off Publ Int Assoc Stud Lung Cancer. 2014;9:947–56. https://doi.org/10.1097/JTO.0000000000000196.
Leary AF, Castro DG, Nicholson AG, Ashley S, Wotherspoon A, O'Brien ME, et al. Establishing an EGFR mutation screening service for non-small cell lung cancer - sample quality criteria and candidate histological predictors. Eur J Cancer. 2012;48:61–7. https://doi.org/10.1016/j.ejca.2011.09.022.
Hlinkova K, Babal P, Berzinec P, Majer I, Mikle-Barathova Z, Piackova B, et al. Evaluation of 2-year experience with EGFR mutation analysis of small diagnostic samples. Diagn Mol Pathol : Am J Surg Pathol Part B. 2013;22:70–5. https://doi.org/10.1097/PDM.0b013e31827e6984.
Fukuoka M, Wu YL, Thongprasert S, Sunpaweravong P, Leong SS, Sriuranpong V, et al. Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). J Clin Oncol : Off J Am Soc Clin Oncol. 2011;29:2866–74. https://doi.org/10.1200/JCO.2010.33.4235.
Han JY, Park K, Kim SW, Lee DH, Kim HY, Kim HT, et al. First-SIGNAL: first-line single-agent iressa versus gemcitabine and cisplatin trial in never-smokers with adenocarcinoma of the lung. J Clin Oncol : Off J Am Soc Clin Oncol. 2012;30:1122–8. https://doi.org/10.1200/JCO.2011.36.8456.
Xu C, Zhou Q, Wu YL. Can EGFR-TKIs be used in first line treatment for advanced non-small cell lung cancer based on selection according to clinical factors? - a literature-based meta-analysis. J Hematol Oncol. 2012;5:62. https://doi.org/10.1186/1756-8722-5-62.
Won YW, Han JY, Lee GK, Park SY, Lim KY, Yoon KA, et al. Comparison of clinical outcome of patients with non-small-cell lung cancer harbouring epidermal growth factor receptor exon 19 or exon 21 mutations. J Clin Pathol. 2011;64:947–52. https://doi.org/10.1136/jclinpath-2011-200169.
Carey KD, Garton AJ, Romero MS, Kahler J, Thomson S, Ross S, et al. Kinetic analysis of epidermal growth factor receptor somatic mutant proteins shows increased sensitivity to the epidermal growth factor receptor tyrosine kinase inhibitor, erlotinib. Cancer Res. 2006;66:8163–71. https://doi.org/10.1158/0008-5472.CAN-06-0453.
Kumar A, Petri ET, Halmos B, Boggon TJ. Structure and clinical relevance of the epidermal growth factor receptor in human cancer. J Clin Oncol : Off J Am Soc Clin Oncol. 2008;26:1742–51. https://doi.org/10.1200/JCO.2007.12.1178.
Choi YJ, Cho BC, Jeong YH, Seo HJ, Kim HJ, Cho A, et al. Correlation between (18)f-fluorodeoxyglucose uptake and epidermal growth factor receptor mutations in advanced lung cancer. Nucl Med Mol Imaging. 2012;46:169–75. https://doi.org/10.1007/s13139-012-0142-z.
Ying J, Guo L, Qiu T, Shan L, Ling Y, Liu X, et al. Diagnostic value of a novel fully automated immunochemistry assay for detection of ALK rearrangement in primary lung adenocarcinoma. Ann Oncol : Off J Eur Soc Med Oncol. 2013;24:2589–93. https://doi.org/10.1093/annonc/mdt295.
van der Wekken AJ, Pelgrim R, Hart TN, Werner N, Mastik MF, Hendriks L, et al. Dichotomous ALK-IHC is a better predictor for ALK inhibition outcome than traditional ALK-FISH in advanced non-small cell lung cancer. Clin Cancer Res : Off J Am Assoc Cancer Res. 2017; https://doi.org/10.1158/1078-0432.CCR-16-1631.
Marchetti A, Di Lorito A, Pace MV, Iezzi M, Felicioni L, D'Antuono T, et al. ALK protein analysis by IHC staining after recent regulatory changes: a comparison of two widely used approaches, revision of the literature, and a new testing algorithm. J Thorac Oncol : Off Publ Int Assoc Stud Lung Cancer. 2016;11:487–95. https://doi.org/10.1016/j.jtho.2015.12.111.
Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5:2892–911.
Tian M, Zhang H, Endo K, Mogi K. Expression of Glut-1, HK-II, HIF-1 alpha, VEGF, p53 and Ki-67 in head and neck squamous cell carcinoma: Correlation with FDG uptake measured by PET. AACR; 2005.
Webb BA, Chimenti M, Jacobson MP, Barber DL. Dysregulated pH: a perfect storm for cancer progression. Nat Rev Cancer. 2011;11:671–7. https://doi.org/10.1038/nrc3110.
Gray JA. Kinetics of enamel dissolution during formation of incipient caries-like lesions. Arch Oral Biol. 1966;11:397–422.
Putney LK, Barber DL. Expression profile of genes regulated by activity of the Na-H exchanger NHE1. BMC Genomics. 2004;5:46. https://doi.org/10.1186/1471-2164-5-46.
Andres V, Carreras J, Cusso R. Regulation of muscle phosphofructokinase by physiological concentrations of bisphosphorylated hexoses: effect of alkalinization. Biochem Biophys Res Commun. 1990;172:328–34.
Trivedi B, Danforth WH. Effect of pH on the kinetics of frog muscle phosphofructokinase. J Biol Chem. 1966;241:4110–2.
Babic I, Anderson ES, Tanaka K, Guo D, Masui K, Li B, et al. EGFR mutation-induced alternative splicing of max contributes to growth of glycolytic tumors in brain cancer. Cell Metab. 2013;17:1000–8. https://doi.org/10.1016/j.cmet.2013.04.013.
Makinoshima H, Takita M, Saruwatari K, Umemura S, Obata Y, Ishii G, et al. Signaling through the Phosphatidylinositol 3-Kinase (PI3K)/mammalian target of Rapamycin (mTOR) Axis is responsible for aerobic Glycolysis mediated by glucose transporter in epidermal growth factor receptor (EGFR)-mutated lung Adenocarcinoma. J Biol Chem. 2015;290:17495–504. https://doi.org/10.1074/jbc.M115.660498.
Velpula KK, Bhasin A, Asuthkar S, Tsung AJ. Combined targeting of PDK1 and EGFR triggers regression of glioblastoma by reversing the Warburg effect. Cancer Res. 2013;73:7277–89. https://doi.org/10.1158/0008-5472.CAN-13-1868.
Alamgeer M, Ganju V, Watkins DN. Novel therapeutic targets in non-small cell lung cancer. Curr Opin Pharmacol. 2013;13:394–401. https://doi.org/10.1016/j.coph.2013.03.010.
Rios Velazquez E, Parmar C, Liu Y, Coroller TP, Cruz G, Stringfield O, et al. Somatic mutations drive distinct imaging phenotypes in lung cancer. Cancer Res. 2017;77:3922–30. https://doi.org/10.1158/0008-5472.CAN-17-0122.
Bahce I, Yaqub M, Smit EF, Lammertsma AA, van Dongen GA, Hendrikse NH. Personalizing NSCLC therapy by characterizing tumors using TKI-PET and immuno-PET. Lung Cancer. 2017;107:1–13. https://doi.org/10.1016/j.lungcan.2016.05.025.
Bahce I, Smit EF, Lubberink M, van der Veldt AA, Yaqub M, Windhorst AD, et al. Development of [(11)C]erlotinib positron emission tomography for in vivo evaluation of EGF receptor mutational status. Clin Cancer Res : Off J Am Assoc Cancer Res. 2013;19:183–93. https://doi.org/10.1158/1078-0432.CCR-12-0289.
Memon AA, Weber B, Winterdahl M, Jakobsen S, Meldgaard P, Madsen HH, et al. PET imaging of patients with non-small cell lung cancer employing an EGF receptor targeting drug as tracer. Br J Cancer. 2011;105:1850–5. https://doi.org/10.1038/bjc.2011.493.
Meng X, Loo BW Jr, Ma L, Murphy JD, Sun X, Yu J. Molecular imaging with 11C-PD153035 PET/CT predicts survival in non-small cell lung cancer treated with EGFR-TKI: a pilot study. J Nucl Med : Off Publ Soc Nucl Med. 2011;52:1573–9. https://doi.org/10.2967/jnumed.111.092874.
Funding
This paper was supported by the National Natural Science Foundation of China (no.81572942), the Natural Science Foundation of Hubei Province (no. 2014CFA057), the Health and Planning Commission Fund of Hubei Province (WJ2017M098), the Science and Technology Support Program of Hubei Province (YSF2015001294), the Wuhan Planning Project of Science and Technology (no. 2014060101010036), the Special Fund for Industrail Transformation and Upgrading, the Independent Innovation Research Fund for Huazhong University of Science and Technology (no. 017KFYXJJ253) and the Scientific Training Program for Young Talents from Union Hospital of Tongji Medical College, Huazhong University of Science and Technology (to Jinshuo Fan).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required. This article does not contain any animal experiments.
Conflict of interest
There was no conflict of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Lv, Z., Fan, J., Xu, J. et al. Value of 18F–FDG PET/CT for predicting EGFR mutations and positive ALK expression in patients with non-small cell lung cancer: a retrospective analysis of 849 Chinese patients. Eur J Nucl Med Mol Imaging 45, 735–750 (2018). https://doi.org/10.1007/s00259-017-3885-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-017-3885-z