
Abstract
Objective
The purpose of this study is to explore the diagnostic accuracy of CT measurements in predicting syndesmosis instability of injured ankle, with correlation to operative findings.
Methods
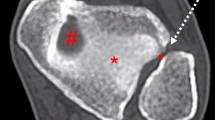
From July 2006 to June 2013, 123 patients presented to a single tertiary hospital who received pre-operative CT for ankle fractures were retrospectively reviewed. All patients underwent open reduction and internal fixation for fractures and intra-operative syndesmosis integrity tests. The morphology of incisura fibularis was categorized as deep or shallow. The tibiofibular distance (TFD) between the medial border of the fibula and the nearest point of the lateral border of tibia were measured at anterior (aTFD), middle (mTFD), posterior (pTFD), and maximal (maxTFD) portions across the syndesmosis on axial CT images at 10 mm proximal to the tibial plafond. Statistical analysis was performed with independent samples t test and ROC curve analysis. Intraobserver reproducibility and inter-observers agreement were also evaluated.
Results
Of the 123 patients, 39 (31.7 %) were operatively diagnosed with syndesmosis instability. No significant difference of incisura fibularis morphology (deep or shallow) and TFDs was demonstrated respective to genders. The axial CT measurements were significantly higher in ankles diagnosed with syndesmosis instability than the group without (maxTFD means 7.2 ± 2.96 mm vs. 4.6 ± 1.4 mm, aTFD mean 4.9 ± 3.7 mm vs. 1.8 ± 1.4 mm, mTFD mean 5.3 ± 2.4 mm vs. 3.2 ± 1.6 mm, pTFD mean 5.3 ± 1.8 mm vs. 4.1 ± 1.3 mm, p < 0.05). Their respective cutoff values with best sensitivity and specificity were calculated; the aTFD (AUC 0.798) and maxTFD (AUC 0.794) achieved the highest diagnostic accuracy. The optimal cutoff levels were aTFD = 4 mm (sensitivity, 56.4 %; specificity, 91.7 %) and maxTFD = 5.65 mm (sensitivity, 74.4 %; specificity, 79.8 %). The inter-observer agreement was good for all aTFD, mTFD, pTFD, and maxTFD measurements (ICC 0.959, 0.799, 0.783, and 0.865). The ICC for intraobserver agreement was also very good, ranging from 0.826 to 0.923.
Conclusions
Axial CT measurements of tibiofibular distance were useful predictors for syndesmosis instability in fractured ankles. The aTFD and maxTFD are the most powerful parameters to predict positive operative instability.




Similar content being viewed by others
References
Riegels-Nielsen P, Christensen J, Greiff J. The stability of the tibio-fibular syndesmosis following rigid internal fixation for type C malleolar fractures: an experimental and clinical study. Injury. 1983;14:357–60.
Van den Bekerrom MP, de Leeuw PA, van Dijk CN. Delayed operative treatment of syndesmotic instability. Current concepts review. Injury. 2009;40(11):1137–42.
Chissell HR, Jones J. The influence of a diastasis screw on the outcome of Weber type-C ankle fractures. J Bone Joint Surg (Br). 1995;77:435–8.
Pettrone FA, Gail M, Pee D, et al. Quantitative criteria for prediction of the results after displaced fracture of the ankle. J Bone Joint Surg Am. 1983;65:667–77.
Leeds HC, Ehrlich MG. Instability of the distal tibiofibular syndesmosis after bimalleolar and trimalleolar ankle fractures. J Bone Joint Surg Am. 1984;66:490–503.
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989;10:156–60.
Beumer A, van Hemert WL, Niesing R, Entius CA, Ginai AZ, Mulder PG, et al. Radiographic measurement of the distal tibiofibular syndesmosis has limited use. Clin Orthop Relat Res. 2004; 227–234.
Pneumaticos SG, Noble PC, Chatziioannou SN, Trevino SG. The effects of rotation on radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle Int. 2002;23:107–11.
Beumer A, Swierstra BA. The influence of ankle positioning on the radiography of the distal tibial tubercles. Surg Radiol Anat. 2003;25:446–50.
Magid D, Michelson JD, Ney DR, et al. Adult ankle fractures: comparison of plain films and interactive two- and three-dimensional CT scans. Am J Roentgenol. 1990;154:1017–23.
Ebraheim NA, Lu J, Yang H, et al. Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: a cadaver study. Foot Ankle Int. 1997;18(11):693–8.
Taşer F, Toker S, Kılınçoğlu V. Evaluation of morphometric characteristics of the fibular incisura on dry bones. Jt Dis Rel Surg. 2009;20(1):52–8.
Gregory DD, Jason HDO, Robert HC, Timothy GW. Normal tibiofibular relationships at the syndesmosis on axial CT imaging. J Orthop Trauma. 2012;26:43–438.
Williams PL, Warwick R, Dyson M, Bannister LH. Gray’s anatomy. 37th ed. Edinburgh: Churchill Livingston; 1989. p. 446–7.
Procter P, Paul JP. Ankle joint biomechanics. J Biomech. 1982;15:627–34.
Harris J, Fallat L. Effects of isolated Weber B fibular fractures on the tibiotalar contact area. J Foot Ankle Surg. 2004;43:3–9.
Ramsey PL, Hamilton W. Changes in tibiotalar area of contact caused by lateral talar shift. J Bone Joint Surg Am. 1976;58:356–7.
Nielson JH, Gardner MJ, Peterson MG, Sallis JG, Potter HG, Helfet DL, et al. Radiographic measurements do not predict syndesmotic injury in ankle fractures: an MRI study. Clin Orthop Relat Res. 2005;436:216–21.
Acute Trauma to the Ankle. American College of Radiology (ACR) Appropriateness Criteria. 2014.
Elgafy H, Semaan HB, Blessinger B, Wassef A, Ebraheim NA. Computed tomography of normal distal tibiofibular syndesmosis. Skelet Radiol. 2010;39:559–64.
Sclafani SJ. Ligamentous injury of the lower tibiofibular syndesmosis: radiographic evidence. Radiology. 1985;156:21–7.
Conflict of interest
The authors have no conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yeung, T.W., Chan, C.Y.G., Chan, W.C.S. et al. Can pre-operative axial CT imaging predict syndesmosis instability in patients sustaining ankle fractures? Seven years’ experience in a tertiary trauma center. Skeletal Radiol 44, 823–829 (2015). https://doi.org/10.1007/s00256-015-2107-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-015-2107-7