
Abstract
Objective
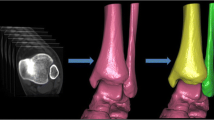
The purpose of this study was to determine the shape and measurements of the normal distal tibiofibular syndesmosis on computed tomographic scans and to identify features that could aid in the diagnosis of syndesmotic diastasis using computed tomography (CT).
Materials and methods
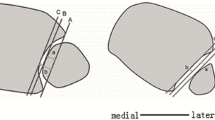
CT scans of 100 patients with normal distal tibiofibular syndesmoses were reviewed retrospectively. In 67% the incisura fibularis was deep, giving the syndesmosis a crescent shape. In 33% the incisura fibularis was shallow, giving the syndesmosis a rectangular shape. The measurements of both types were taken using the same reference points.
Results
The mean age of the patients was 40 years, and there were 53 men and 47 women. The mean width of the distal tibiofibular syndesmosis anteriorly between the tip of the anterior tibial tubercle and the nearest point of the fibula was 2 mm. The mean width of the distal tibiofibular syndesmosis posteriorly between the medial border of the fibula and the nearest point of the lateral border of the posterior tibial tubercle was 4 mm. In men the mean width of the distal tibiofibular syndesmosis, anterior and posterior, was 2 mm and 5 mm, respectively, and in women it was 2 mm and 4 mm, respectively.
Conclusion
This study provides measurements of the normal tibiofibular syndesmosis to aid in the diagnosis of occult diastasis.



Similar content being viewed by others

References
Ashhurst APC, Bromer RS. Classification and mechanism of fractures of the leg bones involving the ankle. Based on a study of three hundred cases from the Episcopal Hospital. Arch Surg. 1922;4:51–129.
Close JR. Some applications of the functional anatomy of the ankle joint. J Bone Joint Surg Am. 1956;38:761–81.
Joy G, Patzakis MJ, Harvey JP Jr. Precise evaluation of the reduction of severe ankle fractures: technique and correlation with end results. J Bone Joint Surg Am. 1974;56:979–93.
Sclafani SJ. Ligamentous injury of the lower tibiofibular syndesmosis: radiographic evidence. Radiology. 1985;156:21–7.
Stiehl JB. Ankle fractures with diastasis. In: Greene WB (editor). Instructional course lectures. Park Ridge, IL: The American Academy of Orthopaedic Surgeons; 1990. pp. 95–103.
Stiehl JB. Complex ankle fracture dislocations with syndesmotic diastasis. Orthop Rev. 1990;19:499–507.
Edwards GS, De Lee JC. Ankle diastasis without fracture. Foot Ankle Int. 1984;4:305–12.
Hopkinson WJ, St Pierre P, Ryan JB, Wheeler JH. Syndesmosis sprains of the ankle. Foot Ankle Int. 1990;10:325–30.
Ebraheim NA, Lu J, Yang H, Mekhail AO, Yeasting RA. Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: a cadaver study. Foot Ankle Int. 1997;18:693–8.
Fritschy D. An unusual ankle injury in top skiers. Am J Sports Med. 1989;17:282–6.
Lovell ES. An unusual rotary injury of the ankle. J Bone Joint Surg Am. 1968;50:163–5.
Marymont JV, Lynch MA, Henning CE. Acute ligamentous diastasis of the ankle without fracture: evaluation by radionuclide imaging. Am J Sports Med. 1986;14:407–9.
Olerud S. Subluxation of the ankle without fracture of the fibula: a case report. J Bone Joint Surg Am. 1971;53:594–6.
Wilson MJ, Michele AA, Jacobsen EW. Ankle dislocations without fracture. J Bone Joint Surg Am. 1939;21:198–204.
Cedell CA. Ankle lesions. Acta Orthop Scand. 1975;46:425–45.
Harper MC. An anatomic and radiologic investigation of the tibiofibular clear space. Foot Ankle Int. 1993;14:455–8.
Pettrone FA, Gail M, Pee D, Fitzpatrick T, Van Herpe L. Quantitative criteria for prediction of the results after displaced fracture of the ankle. J Bone Joint Surg Am. 1983;65:668–77.
Phillips WA, Schwartz HS, Keller CS, et al. A prospective randomized study of the management of severe ankle fractures. J Bone Joint Surg Am. 1985;67:67–78.
Hamilton WJ. Locomotor system. Textbook of human anatomy. 2nd ed. Saint Louis, MO: Mosby; 1976. pp. 125–126.
Williams PL, Warwick R, Dyson M, Bannister LH. Osteology. Gray’s anatomy. 37th ed. Edinburgh: Churchill Livingstone; 1989. pp. 446–447.
Wuest TK. Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg. 1997;5:172–81.
Leeds HC, Ehrlich MG. Instability of the distal tibiofibular syndesmosis after bimalleolar and trimalleolar ankle fractures. J Bone Joint Surg Am. 1950;66:490–503.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Elgafy, H., Semaan, H.B., Blessinger, B. et al. Computed tomography of normal distal tibiofibular syndesmosis. Skeletal Radiol 39, 559–564 (2010). https://doi.org/10.1007/s00256-009-0809-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-009-0809-4