
Abstract
Purpose
The influence of posture on breathing effort in patients with difficult weaning is unknown. We hypothesized that posture could modulate the breathing effort in difficult-to-wean patients.
Methods
A prospective, crossover, physiologic study was performed in 24 intubated patients breathing with pressure support who had already failed a spontaneous breathing trial or an extubation episode. Their median duration of mechanical ventilation before measurements was 25 days. Breathing pattern, occlusion pressure (P 0.1), intrinsic PEEP (PEEPi), and inspiratory muscle effort evaluated by the pressure–time product of the respiratory muscles and the work of breathing were measured during three postures: the seated position in bed (90°LD), simulating the position in a chair, the semi-seated (45°), and the supine (0°) positions consecutively applied in a random order. A comfort score was obtained in 17 cooperative patients. The influence of position on chest wall compliance was measured in another group of 11 sedated patients.
Results
The 45° position was associated with the lowest levels of effort (p ≤ 0.01) and occlusion pressure (p < 0.05), and tended to be more often comfortable. Respiratory effort was the lowest at 45° in 18/24 patients. PEEPi and PEEPi-related work were slightly higher in the supine position (p ≤ 0.01), whereas respiratory effort, heart rate, and P 0.1 values were increased in the seated position (p < 0.05).
Conclusion
A 45° position helps to unload the respiratory muscles, moderately reduces PEEPi, and is often considered as comfortable. The semi-seated position may help the weaning process in ventilator-dependent patients.
Similar content being viewed by others


Introduction
The influence of posture on the respiratory system has been studied in different situations. In healthy human subjects, the functional residual capacity is reduced when switching from the seated to the supine posture, whereas respiratory resistances are increased [1–4]. The esophageal pressure values are slightly less negative seated versus supine [5], but transdiaphragmatic pressures are unchanged [5, 6].
These postural variations probably have a limited relevance for healthy subjects [7, 8], but could influence respiratory pattern and dyspnea in patients with severe chronic pulmonary disease. The supine posture can increase intrinsic positive end-expiratory pressure (PEEPi), dynamic hyperinflation, airway resistances, expiratory flow limitation, or orthopnea in several patients with chronic obstructive pulmonary disease (COPD) [9–11], heart failure [12–14], or obesity [8, 15, 16]. Conversely, some authors have reported a relief of dyspnea for some non-ventilated COPD patients when supine versus seated [6, 17]. In patients with phrenic or neuromuscular paralysis, the functional residual capacity may also be markedly reduced supine versus seated [18, 19]. In mechanically ventilated patients, the supine posture can also induce increased expiratory flow limitation and PEEPi [20, 21].
No major modification was reported for breathing effort seated versus supine in stable COPD patients under noninvasive ventilation [22], in elderly [23] or obese subjects [8, 24]. In patients with prolonged or difficult weaning, weakness of the respiratory muscles is often present [25]. The effects of posture on the work of breathing in these patients may be clinically relevant [26, 27]. Although a semi-recumbent position in bed is often recommended for mechanically ventilated patients [28] because of the decreased risk of microaspirations through the endotracheal tube [29], it is often difficult to maintain in clinical practice [30]. The aim of this study was to assess the physiologic effects of the body position on the work of breathing in patients with weaning difficulties to seek an optimal position regarding respiratory effort.
Methods
An expanded methods section is available in the Electronic Supplementary Material (ESM). The French Society of Intensive Care Ethics Committee approved this prospective, monocentric, randomized, open, crossover clinical study. Informed consent was obtained from all patients.
Patients
Twenty-four invasively ventilated patients with or without tracheostomy and experiencing weaning difficulties were enrolled over a 16-month period. Inclusion criteria were as follows: at least one failure of spontaneous breathing trial before the end of a 2-h trial and/or one unexplained extubation failure (need for reintubation within the 72 h after extubation not related to an untreated cardiac failure or an intercurrent infectious disease or to laryngeal dyspnea). Exclusion criteria were as follows: hemodynamic instability, uncontrolled sepsis, patient refusal, age less than 18 years, and current esophageal pathology. Three positions were applied during the procedure, in random order using a predefined computer-generated list: the supine position (0°), the semi-seated position (45° backrest elevation), and the seated position in bed with legs down (90°LD), simulating sitting in a chair.
Measurements
The ventilator settings were not modified during the procedure. All measurements were performed while the patients were on the same level of pressure support ventilation for the three positions (mean 14 ± 4 cmH2O). Airway pressure (Paw) was measured at the Y connector with a pressure transducer (MP45; Validyne, Northridge, Ca). Flow was measured using a Fleisch no.1 pneumotachograph (Metabo, Lausanne, Switzerland), connected to a differential pressure transducer (DP45-16, Validyne, Northridge, Ca). Esophageal (Pes) and gastric pressures (Pga) were measured using a double-balloon catheter (Marquat, Boissy-Saint Léger, France). The correct placement of the catheter followed standard recommendations and was systematically assessed after each posture modification to obtain a Pes/Paw ratio as close as possible to unity during occlusion [31]. Pressure and flow signals were recorded using specific software (Acknowledge, version 3.5.3, Biopac, Santa Barbara, Ca) and were digitalized using an analog-to-digital converter system (MP100, Biopac, Santa Barbara, Ca).
Inspiratory work of breathing (WOB), esophageal pressure–time product (PTPes), inspiratory time (Ti), total duration of the respiratory cycle (Ttot), RR, V T, minute ventilation (V E), PEEPi, and the work due to PEEPi (W PEEPi) were calculated for each position after 15 min of stabilization, during a quiet tidal breathing period for 1 min [21]. As previously described, effort-to-breathe calculations, PEEPi, and respiratory center output, estimated by the decrease in Pes after 100 ms (P 0.1), were computed from Pes recordings [31]. The clinical values were also collected for each position. A global comfort score including dyspnea was assessed by asking the cooperative patients to compare the comfort of the current position versus the previous and the initial positions. These comparisons allowed a score to be attributed for each position. Consequently, 17 cooperative patients classified each posture as the most comfortable position (score of 1), the intermediate position (score of 2), or the less comfortable position (score of 3).
Static chest wall compliance (Ccw)
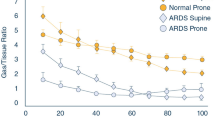
Knowing passive chest wall compliance is necessary for calculations of PTPes and WOB. This could not be measured in these spontaneously breathing patients without using deep sedation and/or hyperventilation. The theoretical value of Ccw in normal supine subjects was used, amounting to 4 % of the predicted value of the vital capacity per cmH2O [1]. This value, however, could be modified by posture and this could influence the WOB or PTPes calculations. To evaluate possible Ccw variations due to body position, we separately enrolled 11 sedated and paralyzed patients necessitating a pressure–volume curve determination with an esophageal pressure for another study (acute respiratory distress syndrome, 10 patients; acute lung injury, 1 patient). Patient characteristics for this substudy are reported in the ESM. Three positions were consecutively applied in these patients during 15 min: the supine position, the 45° semi-seated position, and the nearly seated position (simulating the 90°LD position), similar to the upright position proposed in these indications [32]. Pes was measured for each posture using a balloon catheter. The insertion of this esophageal catheter followed usual recommendations to ascertain a correct placement [33, 34]. For each posture, Ccw was calculated as the mean ratio between V T and the corresponding Pes variations. The Ccw values were compared between the three positions. The median Ccw was 200, 197, and 142 mL/cmH2O in the 0°, 45°, and 90°LD positions (p = 0.03), respectively. The first two positions had similar Ccw (p = 0.8), whereas it was significantly lower in the seated position versus the two others (p < 0.05). Thus, regarding the difficult-to-wean patients, a correcting factor was introduced for the seated Ccw values. The corrected Ccw in the 90°LD position (Ccwcorr 90°LD) was calculated as the product between the theoretical Ccw (Ccw90°LD) and this correcting factor, expressed as a percentage: Ccwcorr 90°LD = 0.72 × Ccw90°LD [35]. The corrected PTPes values in the 90°LD position were similarly calculated. WOB and PTPes values are expressed with this correcting factor for the 90°LD position.
Statistics
Results are expressed as median [25–75th percentiles]. The comparisons of quantitative values between the three groups were performed with the non-parametric Friedman test, and Wilcoxon test for pairwise comparisons when required. As appropriate, categorical qualitative variables were analyzed using Fisher’s test and quantitative continuous variables were compared using regression analyses. The two-sided level of significance was fixed at 0.05 or less.
Results
The characteristics of the difficult-to-wean patients are reported in Table 1. Nine patients suffered from a neurological disorder, five patients had a cardiac arrest, and nine were postoperative patients. Regarding inclusion criteria, 14 patients had experienced a spontaneous breathing failure and 15 patients had experienced at least one extubation failure. The patients were ventilated during the measurements with a pressure support level of 15 cmH2O [12–16], an external PEEP of 5 cmH2O [3–5], and an FiO2 of 38 % [35–40]. Arterial blood gases before measurements were pH = 7.41 [7.36–7.44], PaCO2 = 43 mmHg [39–48], and PaO2 = 85 mmHg [61–101]. Sixteen patients eventually received a tracheostomy (8 after the measurements).
Clinical values in the patient population during the three periods are reported in Table 2. Three patients found the three positions similar in terms of global comfort. In addition, four patients had two preferred or two non-preferred positions. The 45° position was associated 12 times with the best score, the 0° position 7 times, and the 90°LD 6 times (p = 0.09 between the three positions). Respiratory parameters for the three postures are reported in Table 3.
Table 4 illustrates the changes in respiratory center output, respiratory effort, and PEEPi. PEEPi was slightly and significantly higher supine compared with the 45° and the 90°LD positions (p < 0.01; all patients except two had a higher PEEPi supine). Similarly, W PEEPi was significantly lower in the 45° and the 90°LD positions than supine (p ≤ 0.01). All parameters of respiratory effort were significantly lower in the semi-seated position, as compared with the other two positions (Figs. 1, 2). The seated position was significantly associated with the highest effort-to-breathe and P 0.1 values (p = 0.01). Respiratory effort, assessed by PTPes, was the lowest at 45° in all but six patients. Subgroups analyses (tracheostomized patients and patient–ventilator asynchronies) are described in the ESM.

Individual work of breathing changes during the three studied postures (n = 24). WOB work of breathing; 0° supine position; 45° semi-seated position; 90°LD seated position (with legs down). *p = 0.001. Eighteen patients showed a lower WOB value in the semi-seated position compared with the supine and the seated postures

Individual changes of PTP/min during the three studied postures (n = 24). PTP/min pressure–time product of the respiratory muscles, expressed per minute; 0° supine position; 45° semi-seated position; 90°LD seated position (with legs down). *p = 0.002. Eighteen patients showed a lower PTP/min value in the semi-seated position compared with the supine and the seated postures
For all three positions, a correlation was observed between PEEPi values and the PTP expressed per minute (p < 0.001; r = 0.63; r 2 = 0.4; see the ESM), between PEEPi values and the WOB expressed as J/min (p < 0.001, r = 0.53; r 2 = 0.28), and between PEEPi and P 0.1 (p < 0.001; r = 0.67; r 2 = 0.45).
Discussion
To our knowledge, this is the first study evaluating the clinical and physiological effects of posture on the effort-to-breathe measurements during difficult weaning from mechanical ventilation. The main results of this study can be summarized as follows: (1) respiratory effort parameters were slightly but significantly decreased in the semi-seated position compared with the other two positions, (2) comfort in the semi-seated position was at least as good compared with the other positions, (3) the seated position was associated with the highest effort-to-breathe values, (4) the respiratory drive was significantly higher seated compared with the semi-seated position, (5) PEEPi and PEEPi-related work were moderately but significantly increased supine compared with the two other positions.
Effect of posture on the breathing pattern, PEEPi, and dyspnea
No significant modification regarding the respiratory pattern was found according to postural changes in our study. The slight PEEPi and dyspnea sensation changes according to posture are in accordance with several studies. In healthy subjects, respiratory pattern modifications according to posture have been thoroughly investigated. The functional residual capacity is reduced by 20–30 % when switching from the seated to the supine posture [1, 2, 4, 13]. This effect is related to the increased intrathoracic blood volume, the more cephalic position of the diaphragm, and small airway closure. This effect leads to increased resistances supine versus seated.
In COPD patients, the supine posture is associated with dyspnea, i.e. orthopnea, and expiratory flow limitation at rest is an earlier manifestation in supine than in sitting position [10, 11]. Although some COPD patients report a supine relief of dyspnea [6, 17], several patients with COPD experience more severe dyspnea in the supine position [9–11]. Increased dynamic hyperinflation, airway resistances, PEEPi, and expiratory flow limitation could play a role in orthopnea genesis. In several patients with heart failure [12–14] or obese subjects [8, 15, 16], airway resistances, PEEPi, expiratory flow limitation, and orthopnea are also increased supine versus seated. Patients with severe phrenic or neuromuscular paralysis experience a major reduction of functional residual capacity when supine [18, 19]. In mechanically ventilated patients [20], the supine posture can enhance expiratory flow limitation and can increase PEEPi and PEEPi-related work compared with the 30° position in adults with acute respiratory distress syndrome [21]. In ventilated patients with abdominal distension or obesity, comfort is reduced seated and supine in comparison with the semi-seated position [36].
The correlations observed between PEEPi and all respiratory effort parameters in our study support that PEEPi seems to be one of the determinants explaining the increased effort observed supine during weaning: the higher was the PEEPi, the higher was the inspiratory effort. A higher central respiratory drive and “stimulation” induced by the seated position itself could explain in part why the inspiratory muscles’ efforts are higher seated despite lower PEEPi. The potential role of the changes in Ccw when seated should be further evaluated: Ccw was not directly measured during weaning and results are based on the hypothesis that similar changes should occur as in our group of paralyzed patients.
Effect of posture on respiratory effort
The semi-seated position induces a decreased respiratory effort in the present study, as compared with the supine and the seated positions. This is the first study to evaluate the effects of posture in patients with difficult weaning using measurements of breathing effort. Patients with weaning failure experience a marked increase in respiratory load and respiratory muscle effort [25, 27]. One of the most important objectives of mechanical ventilation is to decrease the work of breathing to a level acceptable for the patient. Weaning failure often results from an imbalance between mechanical load and respiratory muscle activity.
Most studies evaluating the respiratory effort changes according to posture reported no difference or minor differences. In healthy subjects, the transdiaphragmatic pressures remained unchanged between the supine, semi-seated, and seated postures [5–8]. In elderly subjects, WOB, P 0.1, PTPes, and transdiaphragmatic pressures were found to be unchanged seated versus supine [23]. In stable COPD patients, the transdiaphragmatic pressures decreased seated versus supine [6, 17, 37], whereas the PTPes and the swings of Pes were similar [22]. In obese subjects, mean transdiaphragmatic pressures and WOB seemed unchanged supine versus seated [8, 24]. None of these studies evaluated the semi-seated position, and most of them included a small number of stable and not severe patients. Postural variations are probably not relevant for healthy or stable subjects [7, 8], but the influence of posture may be greater for the most severe patients, with little respiratory reserve and important respiratory efforts. The current study concerns a selected population with severe patients, as indicated by multiple co-morbidities, elevated severity scores at admission and mortality rate, and a prolonged mechanical ventilation duration and length of hospitalization. Indeed, the largest change obtained in adopting the semi-seated position was found for patients presenting the highest effort-to-breathe levels supine or seated (data shown in the ESM).
Study limitations
The simple score used in our study to assess the global comfort could lead to bias, as it represents a subjective evaluation and not a visual quantitative scale. Other more recognized scores should have been used to assess dyspnea. Our simplified score was adapted from a previous study to specifically evaluate this population of ventilated or tracheostomized patients [31]. Bias was prevented using the randomization to determine the order of postures and always asking the same question after stabilization for each position.
It was not possible to obtain the Ccw, which is an important factor for the respiratory effort calculations, in the studied patients during the effort-to-breathe measurements. Major differences in Ccw were found only in the seated position in our separate study performed in paralyzed patients. Although this may differ in sedated and spontaneously breathing patients, it was important to take it into account. Because Ccw was not directly measured in the difficult-to-wean patients, this constitutes a limitation of the study. It could be argued that the difficult-to-wean patients are not strictly comparable with these paralyzed patients. However, most of clinical characteristics were similar between these two groups: age, body mass index, SAPS II, and V T that could influence Ccw variations according to posture [38]. Because Ccw was different only in the seated position (90°LD) versus the other two positions, it could not have influenced the effort-to-breathe differences found between the supine and semi-seated positions. Conversely, the correcting factor increased the respiratory effort differences found between the semi-seated and seated positions.
The validity of the Pes measurements according to postural changes has been discussed elsewhere [8]. Additionally, the occlusion tests expressed as the Pes/Paw ratio were similar for all positions.
The pressure support ventilation with a median level of 15 cmH2O may explain the low respiratory efforts levels recorded in our patients. It could also explain in part why WOB and PTP values are statistically different between postures with differences which do not seem to be really clinically relevant at these levels of pressure support. Results could be different if measured at lower pressure support levels or during spontaneous unassisted breathing.
Clinical implications
Several studies pointed out that many ICU patients are not positioned in a semi-recumbent position despite recommendations to do so [39, 40]. The 45° position in the bed is recommended for mechanically ventilated patients [28], mainly because of the decreased risk of microaspirations along the endotracheal tube walls [29]. This position, however, is often difficult to maintain in clinical practice [30]. Our study provides a new rationale for implementing the semi-seated position when difficult weaning is considered. Difficult-to-wean patients are often ventilated for prolonged periods and postural recommendations could have a clinical impact, especially when weaning tests are performed using low levels of pressure support or T-tube tests.
In summary, the semi-seated position at 45° decreases the inspiratory effort and is found to be at least as comfortable as other positions for difficult-to-wean patients. PEEPi and PEEPi-related work are moderately higher supine and could explain part of these findings. In the seated position compared with supine, PEEPi and PEEPi-related work are lower but the effort-to-breathe is not, possibly because of a higher central respiratory drive. The potential role of a reduced chest wall compliance when seated, as measured in paralyzed patients, must be clarified. These results are clinically relevant because they show that the recommended semi-seated position represents a good compromise to decrease PEEPi and to unload the respiratory muscles in the situation of difficult weaning.
References
Agostoni E, Hyatt RE (1986) Static behaviour of the respiratory system. In: Handbook of physiology, sect 3, vol III, part 1, chap 9. American Physiological Society, Washington, pp 113–130
Behrakis PK, Baydur A, Jaeger MJ, Milic-Emili J (1983) Lung mechanics in sitting and horizontal body positions. Chest 83:643–646
Baydur A, Sassoon CS, Carlson M (1996) Measurement of lung mechanics at different lung volumes and esophageal levels in normal subjects: effect of posture change. Lung 174:139–151
Rehder K (1998) Postural changes in respiratory function. Acta Anaesthesiol Scand Suppl 113:13–16
Druz WS, Sharp JT (1981) Activity of respiratory muscles in upright and recumbent humans. J Appl Physiol 51:1552–1561
Druz WS, Sharp JT (1982) Electrical and mechanical activity of the diaphragm accompanying body position in severe chronic obstructive pulmonary disease. Am Rev Respir Dis 125:275–280
Koulouris N, Mulvey DA, Laroche CM, Goldstone J, Moxham J, Green M (1989) The effect of posture and abdominal binding on respiratory pressures. Eur Respir J 2:961–965
Pankow W, Podszus T, Gutheil T, Penzel T, Peter J, Von Wichert P (1998) Expiratory flow limitation and intrinsic positive end-expiratory pressure in obesity. J Appl Physiol 85:1236–1243
O’Neill S, McCarthy DS (1983) Postural relief of dyspnoea in severe chronic airflow limitation: relationship to respiratory muscle strength. Thorax 38:595–600
Popa V, Zumstein P (1993) Wheezing triggered by dorsal decubitus: pulmonary function changes. Respiration 60:257–263
Eltayara L, Ghezzo H, Milic-Emili J (2001) Orthopnea and tidal expiratory flow limitation in patients with stable COPD. Chest 119:99–104
Duguet A, Tantucci C, Lozinguez O, Isnard R, Thomas D, Zelter M, Derenne JP, Milic-Emili J, Similowski T (2000) Expiratory flow limitation as a determinant of orthopnea in acute left heart failure. J Am Coll Cardiol 35:690–700
Yap JC, Moore DM, Cleland JG, Pride NB (2000) Effect of supine posture on respiratory mechanics in chronic left ventricular failure. Am J Respir Crit Care Med 162:1285–1291
Torchio R, Gulotta C, Greco-Lucchina P, Perboni A, Avonto L, Ghezzo H, Milic-Emili J (2006) Orthopnea and tidal expiratory flow limitation in chronic heart failure. Chest 130:472–479
Yap JC, Watson RA, Gilbey S, Pride NB (1995) Effects of posture on respiratory mechanics in obesity. J Appl Physiol 79:1199–1205
Pelosi P, Croci M, Ravagnan I, Cerisara M, Vicardi P, Lissoni A, Gattinoni L (1997) Respiratory system mechanics in sedated, paralyzed, morbidly obese patients. J Appl Physiol 82:811–818
Sharp JT, Drutz WS, Moisan T, Foster J, Machnach W (1980) Postural relief of dyspnea in severe chronic obstructive pulmonary disease. Am Rev Respir Dis 122:201–211
Mier-Jedrzejowicz A, Brophy C, Moxham J, Green M (1988) Assessment of diaphragm weakness. Am Rev Respir Dis 137:877–883
Fromageot C, Lofaso F, Annane D, Falaize L, Lejaille M, Clair B, Gajdos P, Raphael JC (2001) Supine fall in lung volumes in the assessment of diaphragmatic weakness in neuromuscular disorders. Arch Phys Med Rehabil 82:123–128
Valta P, Corbeil C, Lavoie A, Campodonico R, Koulouris N, Chasse M, Braidy J, Milic-Emili J (1994) Detection of expiratory flow limitation during mechanical ventilation. Am J Respir Crit Care Med 150:1311–1317
Koutsoukou A, Armaganidis A, Stavrakaki-Kallergi C, Vassilakopoulos T, Lymberis A, Roussos C, Milic-Emili J (2000) Expiratory flow limitation and intrinsic positive end-expiratory pressure at zero positive end-expiratory pressure in patients with adult respiratory distress syndrome. Am J Respir Crit Care Med 161:1590–1596
Porta R, Vitacca M, Clini E, Ambrosino N (1999) Physiological effects of posture on mask ventilation in awake stable chronic hypercapnic COPD patients. Eur Respir J 14:517–522
Vitacca M, Clini E, Spassini W, Scaglia L, Negrini P, Quadri A (1996) Does the supine position worsen respiratory function in elderly subjects? Gerontology 42:46–53
Barchfeld T, Schonhofer B, Wenzel M, Kohler D (1997) Work of breathing in differentiation of various forms of sleep-related breathing disorders. Pneumologie 51:931–935
Tobin MJ, Laghi F, Brochard L (2009) Role of the respiratory muscles in acute respiratory failure of COPD: lessons from weaning failure. J Appl Physiol 107:962–970
Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, Pearl R, Silverman H, Stanchina M, Vieillard-Baron A, Welte T (2007) Weaning from mechanical ventilation. Eur Respir J 29:1033–1056
Brochard L, Thille AW (2009) What is the proper approach to liberating the weak from mechanical ventilation? Crit Care Med 37:S410–S415
Tablan OC, Anderson LJ, Besser R, Bridges C, Hajjeh R (2004) Guidelines for preventing health-care-associated pneumonia, 2003: recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR Recomm Rep 53:1–36
Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M (1999) Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet 354:1851–1858
van Nieuwenhoven CA, Vandenbroucke-Grauls C, van Tiel FH, Joore HC, van Schijndel RJ, van der Tweel I, Ramsay G, Bonten MJ (2006) Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: a randomized study. Crit Care Med 34:396–402
L’Her E, Deye N, Lellouche F, Taille S, Demoule A, Fraticelli A, Mancebo J, Brochard L (2005) Physiologic effects of noninvasive ventilation during acute lung injury. Am J Respir Crit Care Med 172:1112–1118
Richard JC, Maggiore SM, Mancebo J, Lemaire F, Jonson B, Brochard L (2006) Effects of vertical positioning on gas exchange and lung volumes in acute respiratory distress syndrome. Intensive Care Med 32:1623–1626
Servillo G, Svantesson C, Beydon L, Roupie E, Brochard L, Lemaire F, Jonson B (1997) Pressure-volume curves in acute respiratory failure: automated low flow inflation versus occlusion. Am J Respir Crit Care Med 155:1629–1636
Maggiore SM, Jonson B, Richard JC, Jaber S, Lemaire F, Brochard L (2001) Alveolar derecruitment at decremental positive end-expiratory pressure levels in acute lung injury: comparison with the lower inflection point, oxygenation, and compliance. Am J Respir Crit Care Med 164:795–801
Truwit JD, Marini JJ (1988) Evaluation of thoracic mechanics in the ventilated patient. Part II: applied mechanics. J Crit Care 3:199–213
Burns SM, Egloff MB, Ryan B, Carpenter R, Burns JE (1994) Effect of body position on spontaneous respiratory rate and tidal volume in patients with obesity, abdominal distension and ascites. Am J Crit Care 3:102–106
Heijdra YF, Dekhuijzen PN, van Herwaarden CL, Folgering HT (1994) Effects of body position, hyperinflation, and blood gas tensions on maximal respiratory pressures in patients with chronic obstructive pulmonary disease. Thorax 49:453–458
Knowles JH, Hong SK, Rahn H (1959) Possible errors using esophageal balloon in determination of pressure-volume characteristics of the lung and thoracic cage. J Appl Physiol 14:525–530
Reeve BK, Cook DJ (1999) Semi-recumbency amoung mechanically ventilated ICU patients: a multicenter observational study. Clin Intensive Care 10:241–244
Grap MJ, Munro CL, Hummel RS 3rd, Elswick RK Jr, McKinney JL, Sessler CN (2005) Effect of backrest elevation on the development of ventilator-associated pneumonia. Am J Crit Care 14:325–332
Acknowledgments
A part of this study was supported by a grant from Antadir (http://www.antadir.com).
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is dedicated to Professor A. Harf who died on 8 July 2003.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Deye, N., Lellouche, F., Maggiore, S.M. et al. The semi-seated position slightly reduces the effort to breathe during difficult weaning. Intensive Care Med 39, 85–92 (2013). https://doi.org/10.1007/s00134-012-2727-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-012-2727-5